International Journal of Anesthesiology & Research (IJAR) / IJAR-2332-2780-02-301
Addition of Dexomedetomidine to Local Anaesthesia for Retrobulbar Block: Does It Improve The Quality of Anaesthesia?
Dief Abdel Gelil Ahmed
Department of Anaesthesia, Faculty of Medicine, Zagazaig University, Egypt.
*Corresponding Author
Dief Abdel Gelil Ahmed,
Department of Anaesthesia,
Faculty of Medicine, Zagazaig University,
Egypt.
Tel: 0507577584
E-mail: daif12@hotmail.com
Article Type: Research Article
Accepted: March 31, 2014; Published: April 02, 2014
Citation: Gelil Ahmed D A (2014) Addition of Dexomedetomidine to Local Anaesthesia for Retrobulbar Block: Does It Improve The Quality of Anaesthesia?. Int J Anesth Res. 2(3), 35-39. doi: dx.doi.org/10.19070/2332-2780-1400010
Copyright: Gelil Ahmed D A © 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: We evaluate addition of dexmedetomidine to local anesthesia in retrobulbar block in patient underwent primary retinal detachment surgery.
Methods: Sixty patients were randomly allocated into two equal groups (n=30). In both retrobulbar block was perfomed. In addition, group B received dexomedetomidine 1μg/kg with local anesthesia. Motor kinesia, motor and sensory block duration, postoperative pain was assessed by visual analog scale time and first demand for analgesia were recorded. Also degree of sedation evaluated during surgery.
Results: In group B with addition of dexmedetomidine the number of patient who developed akinesia more and requirement of supplementary injection were lowered. Also duration motor and sensory block was longer and requirement for postoperative analgesic were significantly less with mean sedation scores were higher in patients receiving dexmedetomindine with local anesthesia.
Conclusion: We are concluded that addition of dexmedetomidine to local anesthesia will improve the quality of block, increase the duration of block, prolong the duration of postoperative analgesia and decrease requirements for postoperative analgesic without side effects.
2.Introduction
3.Patient and Methods
4.Patient Monitoring
5. Statistical Analysis
6. Results
7. VAS
8. Discussion
9. Conclusion
8. Declaration of Interest
9. References
Keywords
Dexomedetomidine; Retrobulbar block; Lidocaine.
Introduction
Retrobulbar block involves desposition of local anesthetic inside muscle cone. It aim to block the ciliary nerves, the ciliary ganglion and cranial neves II, III and VI. Cranial nerve IV not affected since it lies outside the muscle cone [1]. The characterisitics of patients for vitroretinal surgery, most of them elderly and associated with diseases such as diabetes mellitus and cardiac problems, make L.A. advisable to reduce risks and morbidity. Retinal detachment surgery associated with high incidence of postoperative pain as a result inactivation of ocular muscle and sclera and or increase intraocular pressure from expansion if gas bubble or tight bucking or encirclement [2, 3].
For many ophthalmic surgeons, LA has become more preferred over general anesthesia (GA) owing to quicker patient rehabilitation, avoidance of probable complications from GA and better analgesic properties postoperatively [4]. Dexmedetomidine is a potent highly selective and specific α2 adrenoreceptor agonist that has both sedative and analgesic effects with no respiratory depression. In addition it possesses sympatholytic and antinociceptive effects that allow hemodynamic stability during surgical stimulation [5, 6]. Compared with clonidine, dexmedetomidine is about eight times more specific for α 2: α1 selectively ratio of 1600:1 [7]. We designed this study to evaluate the effect of addition of dexamedetomidine to LA for retrobulbar blockand does it improve quality of block or not?
Patient and Methods
After the approval of the study by ethical committee and informed consent from patients, 60 patients of ASA (American Society of Anesthesiologists) Grade I – III between the ages of 46 and 72 years were enrolled in this study that underwent for primary retinal detachment surgery.
The patient with hematological disease, bleeding or coagulation abnormalities, psychiatric diseases, history of allergy to use drug were excluded from study. All operations were performed by the same experienced surgeon.
Patients were randomly allocated to one of the following, two equal groups (N=30 in each group).
All patients received retrobular block injected at junction of lateral one third and medial two thirds of infra-orbital rim, using a 24 G disposable 35mm needle. The injection consisted of a 60:40 mixture of 2% Lidocaine and 0.5% Bupivacaine with 10 I.U./ml of Hyaluronidase, while patients in group B received 1μg/Kg mixed with local anesthesia. The drug syringes were prepared by anesthesia technician, who unaware of proceeding.
After negative aspiration 5-7ml of the local anesthesia solution was slowly injected until a complete drop and fullness of upper eyelid. To decrease intra-ocular pressure, mechanical orbital compression applied for 10 min. in all patients by using Honan ballon, adjusted to 30mmHg. Patients were evaluated for motor akinesia from Grade 0-2; Zero if there was free movement, one if there was a partial movement and 2 if there was no movement. This was done for each of four recti, levator superiors and orbicularis oculi muscles.
The maximum score was 12 indicates total akinesia. An eye with a score less than 8, received a repeat 3ml injection of the same anesthetic mixture and recorded. No intra-ocular local supplementation was used in any patient. A nasal cannula applied and supplemental oxygen was given throughout the procedure at rate of 3L/min for all patients. Sensory block was considered with ablation of corneal reflex after installation of drops of physiological solution on the conjunctiva and cornea. The motor and sensory block durations (min.) were evaluated frequenty in postoperative period every hour. Post-operative pain was assessed by visual analog scale (0= no pain, 10= worest pain). If VAS for pain was >4 Diclofenac 1mg/Kg was given intramuscularly. If pain severe VAS >7 in addition to Diclofenac Tramadol 100mg I.M was given as well. The time for first demand for analgesia, dosage and number of patients asked for analgesia during first 24 hours post-operatively were recorded. In operating theater, a good intravenous access was secured and monitoring devices were attached, which include heart rate, electrocardiograph (ECG), pulse oximetry (SPO2). Non-invasive blood pressure (NIBP), respiratory rate and baseline parameters were recorded. The success of block was measured by motor akinesia of eye and by assessment of hemodynamic stability as indicated by the absence of increase in heart rate and or systolic blood pressure or more than 20% compared with baseline values obtained in pre-operative period.
Hypotension defined as systolic arterial pressure falling more than 20% mmHg was treated with Ephedrine and heart rate <50 beats/min was treated with Atropine. Intravenous fluids were given according to body weight and operative loss requirement.During surgical procedure adverse event like nausea, vomiting, pruritis, and shivering were recorded and treated.
Patient Monitoring
Hemodynamic variable (heart rate and mean arterial blood pressure) at baseline and after the retrobular block every 10 minutes until end of surgery. Pain assessment by Visual Analog Scale (0= No pain, 10= Worest pain). Pain score was assessed during surgery, at the end of surgery and every 4 hours for 24 hours postoperatively.
The degree of sedation evaluated also by Ramsay Scale during surgery [8].
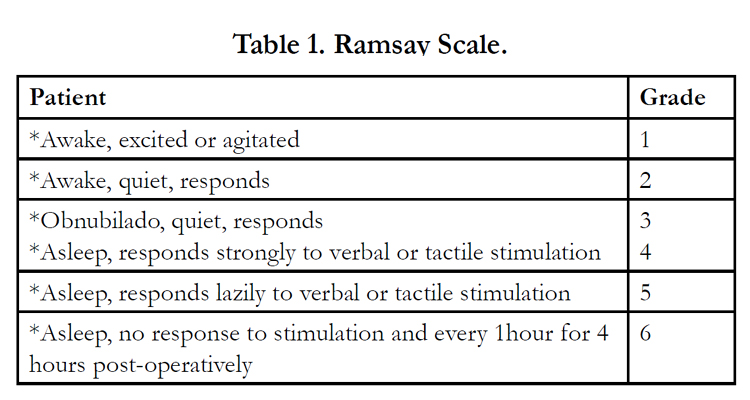

Table 1. Ramsay Scale.
Statistical Analysis
At the end of Study, all data complied systematically and analyzed using analysis of variance and chi-square test. Chicago III was used to compare the continuous variables between the two groups. Values of P <0.05 was considered significant and P <0.0001 as highly significant. Pain and Sedation Scores were analyzed with the Mann-Whitney U Test – SPSS U15.0 for Windows Software (SPSS, Inc, Chicago, Illinois USA) was used for statistical analysis.
Results
A total of 60 patients underwent retinal detachment surgery enrolled in this study and randomly divided into two groups. The demographics profiles of the patients in both groups were comparable with regards to age, weight, and ASA physical status was similar in both groups and mean duration of surgery was comparable in both groups and statistically non significant (P>0.05).(Table 2).
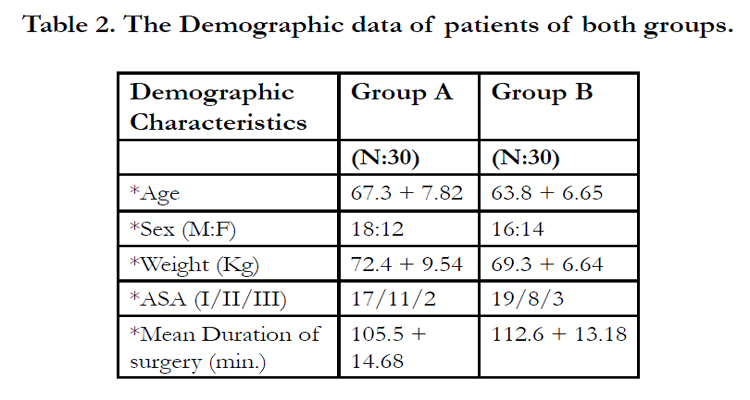
Table 2. The Demographic data of patients of both groups.
In group B, heart rate and systolic blood pressure decreased significantly relative to baseline values, however there was no statistical difference between groups when compared for MAP, HR, SPO2 intra-operatively and post-operatively (Fig. 1,2).
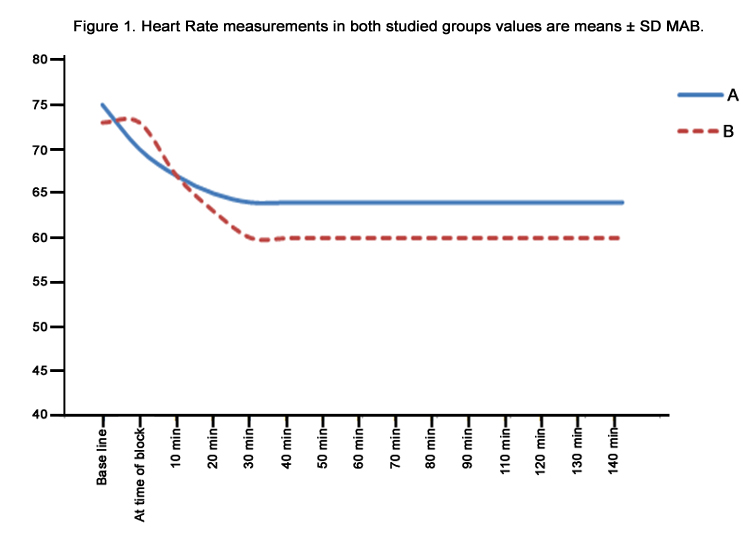
Figure 1. Heart Rate measurements in both studied groups values are means ± SD MAB.
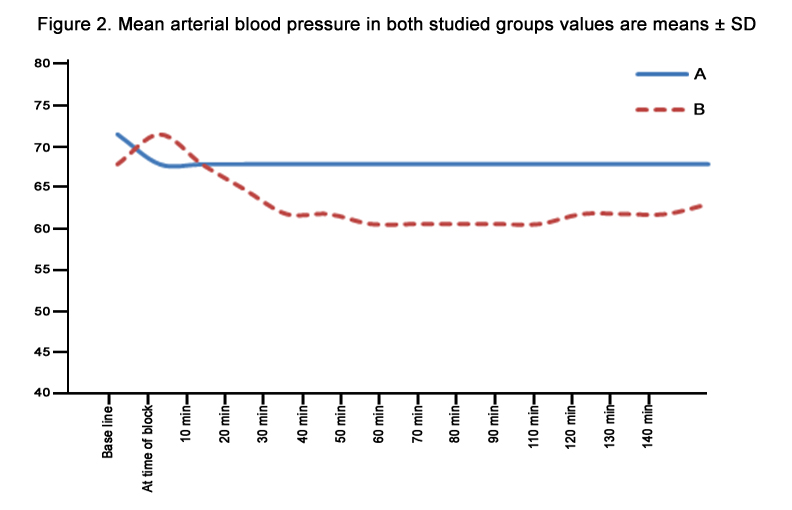
Figure 2. Mean arterial blood pressure in both studied groups values are means ± SD
The number of patients developed global akinesia (15 min after block) higher in group B, 29 patients (96.6%) while 25 patients(83.3%) in group A develop akinesia (P=0.024). The number of patients who required supplementary injection were significantly lower (P=0.024) in group B, 1 patient (3.33%) compared with 5 patients (16.6%) in group A. The total volume of L.A. injected in group B which is 7.2 ml, which is significantly less (P= 0.029) than the volume of L.A. in group A 8.3 ml. The duration of motor block (min) was significantly longer (P= 0.001) in group B (182 + 15) compared with patients in group A (125 + 17). As well as sensory block duration time (min) was significantly longer (P=0.001) in group B (402 +19) compared with patients in group A (245 + 25) [Table 3].
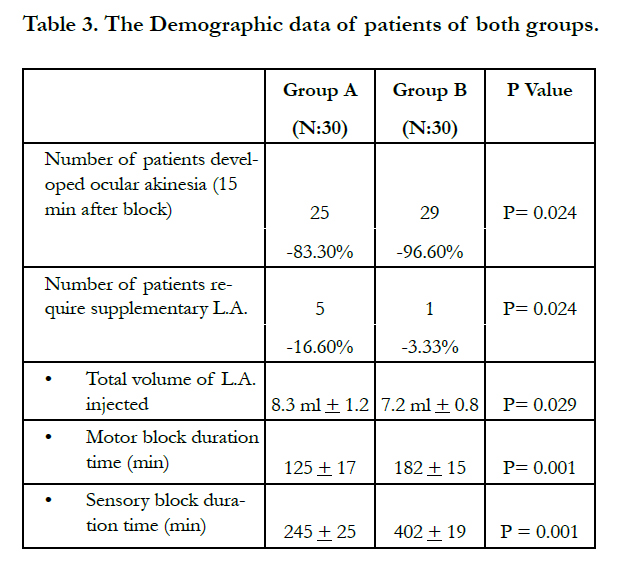
Table 3. The Demographic data of patients of both groups.
Table 4 shows the degree of sedation observed in both studied groups. Mean sedation scores were significantly higher in group B compared to patients in group A as 10 patients (33.3%), in group B had sedation score of 3as compared to 3 patients (10%) in group A. Only 9 patients (30%) in group A had sedation scores of 1 compared with 3 patients (10%) in group B, which was highly significant statistical entity. Table 4.
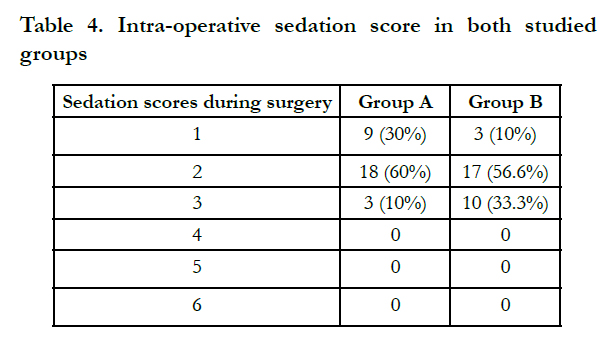
Table 4. Intra-operative sedation score in both studied groups
In first 24 hours post-operatively patients in group B had lower values of visual analog scale of pain compared with patients in group A. (Fig. 3)
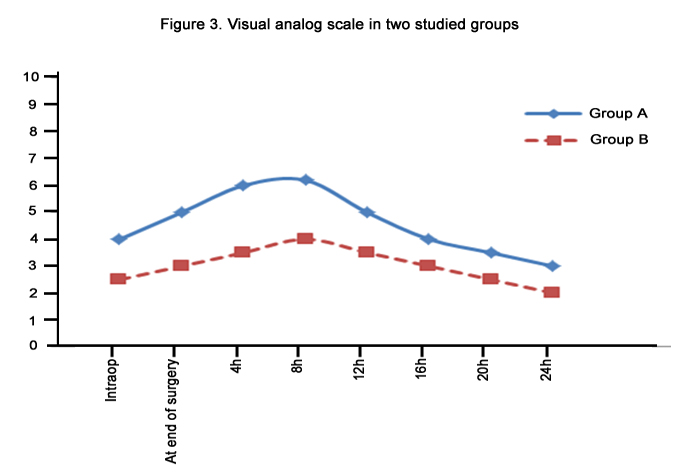
Figure 3. Visual analog scale in two studied groups
VAS
All patients in group A required postoperative pain medication during the first 24 hour compared with 20 patients (66.6%) in group B (P= 0.04). The time of first request to analgesia was longer in patients of group B [mean 16 (14-18) hour]as compared with those who in group A [mean 9 (7-11) hour]. The diclofenac consumption (mg) was significantly less in group B (88.6 + 12.5) compared with patients of group A (195.3 + 32.5). Also, the percentage of patient who required tramadol injection were significantly less in group B 3 patients (10%) compared with group A 9 patients (30%). Table 5.
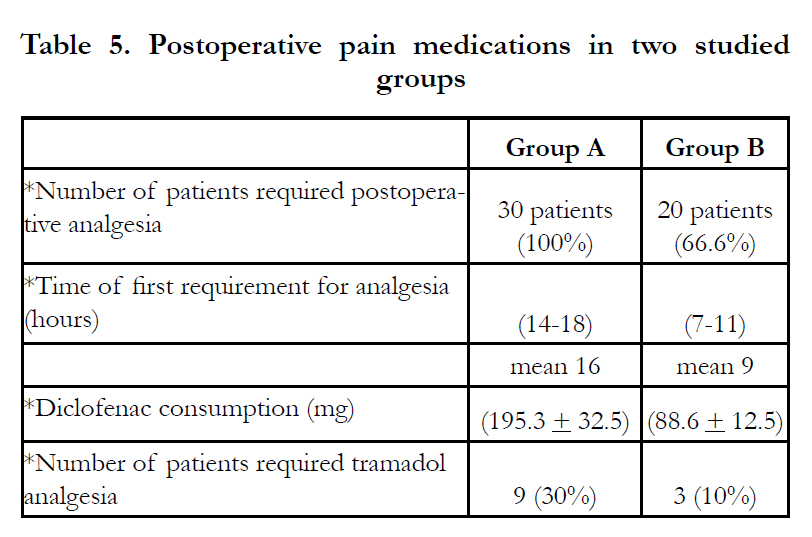
Table 5. Postoperative pain medications in two studied groups
The incidence of various side effects in both groups were observed in intraop and postop period. Dry mouth was higher in both studied group but with no significant difference (P>0.05). we did not observe respiratory depression in any patient from both group. The incidence of other side effects like nausea, vomiting, headache, dizziness, hypotension, bradycardia, shivering and pruritis observed and treated. Table 6.
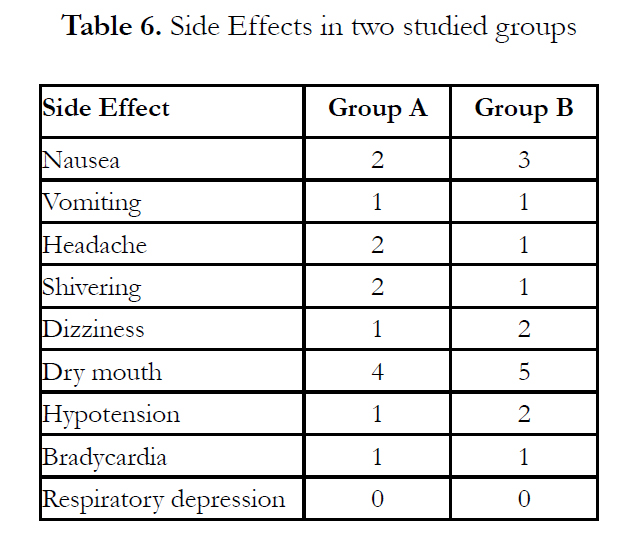
Table 6. Side Effects in two studied groups.
Discussion
The study of pharmacological properties of α-2 agonists have been extensively studied to achieve the desired effects in regional anesthesia. [9, 10, 11, 12] Regional administration of these drugs associated with sedation; analgesia, anxiolysis, hypnosis, and sympatholysis. [13, 14] Clonidine has been used successfully over the last decade for the said purpose and with introduction of dexmedetomide has further widened the scope of α-2 agonist in regional anesthesia [15, 16] The faster onset of action of local anesthetics, rapid establishment of both sensory and motor block prolonged duration of postoperative period and stable cardiovascular parameters makes these agents a very effective adjuvant in regional anesthesia [17, 18, 19, 20, 21]. This study has demonstrated that the use of dexmedetomidine with lidocaine for retrobulbar block for primary retinal detachment surgery provided more effective retrobulbar block with more patients who developed successful block and fewer patients who required supplementary injection and less volume of L.A. solution used compared with control group. Furthermore, the motor block duration and sensory block duration was significantly longer in the patients receiving dexmedetomidine also postoperative analgesia more prolonged with lower consumption of diclofenac and tramadol in patients receiving dexmedetomidine.
In previous studies designed for different clinical applications Bajwa and colleagues [22] Compared dexmedetomidine with clonidine in epidural anesthesia for patients underwent for vaginal hysterectomies. They found that dexmedetomidine is better neuraxial adjuvant compared to clonidine for providing early onset of sensory analgesia, adequate sedation and prolonged postoperative analgesia. Memis et.al. [23] in their studies of adding dexmedetomidine to lidocaine for intravenous regional anaesthesia, they reported that it improved the quality of anaesthesia and intraoperative, postoperative analgesia without causing side effects . Mauro et.al [24] in their study of clonidine and dexmedetomidine via epidural for postoperative analgesia and sedation in choleystectomy they found statistically significant differences were found between groups in relation to sedation and analgesia, this difference were favorable for dexmedetomidine as the drug effectively inhibits transmission of nociceptive signals through the spinal cord when it joins to pre and post synaptic receptors causing sedation, analgesia and adequate quality anesthesia. Sensory block is installed quickly, in which surgical area can be manipulated, no matter which the motor block is not fully installed [25]. This results close to results obtained by Oril-Lopez et.al who use epidural dexmedetomidine plus local anesthetics to reduce anexity and keep patient in a state of active sedation, which reduces the likehood of respiratory depression which arise when adjuvant drugs are administered intravenously [26]. Brummett et.al found that the sensory and motor block in rats was enhanced significantly by addition of dexmedetomidine in combination with bupivacaine insciatic nerve block [27]. Results of the present study in agreement of study done by Obayah et.al. They found addition of dexmedetomidine to bupivcacaine for greater palatine nerve block after cleft palate repair appeared to extend significant duration of sensory block and prolonged the duration of postoperative pain relief [28].
Conclusion
In conclusion., addition of dexmedetomidine to lidocaine in retrobulbar anesthesia will improve quality of local anesthesia and prolong postoperative pain relief and decrease requirement for analgesics with no side effects.
Declaration of Interest
• This study done in Bin RushdOpthalmic Center in Riyadh,K.S.A.
• The author indicates no financial support for any sources for this study.
References
- Stewart J. Kellett N, Castro D. The central nervous system and cardiovascular effects of levobupivacaine and ropivacaine in healthy volunteers. AnesthAnalg 2003;97;412-6.
- Newsom RS, Wainwright AC, Canning CR. Local anesthesia for 1221 viteoretinal procedures. Br J Opthalmol 2001;85:225-7.
- Shende D, Sadhasivam S, Madan R. Effects of peribulbar bupivacaine as an adjunct to general anesthesia on perioperative outcome following retinal detachment surgery. Anesthesia 2000;55:970-5.
- Eke T, Thompson J. The national survey of local anesthesia for ocular surgery II. Survey methodology and current practice. Eye 1999;13:196-204.
- Rizzo L, Marini M, Rosati C, Calamai I, Nesi M, Salvini R, et.al. Peribulbar anesthesia: A percuteneous single injection technique with a small volume of anesthetic. AnesthAnalg 2005;100:94-6.
- Frow MW, Miranda-CaraballoJl, Akhtar TM, Hugkulstone CE. Single injection peribulbar anesthesia, total upper eyelid drop as an endpoint marker. Anesthesia 2000;55:750-6.
- Casati A, Borghi B, Fanelli G, Cerchierini E, Santorsola R, Sassoli V, et.al. A double blinded randomized comparison of either 0.5% levobupivacaine or 0.5% ropivacaine for sciatic nerve block. AnesthAnalg 2002;94:987-90.
- Ramsay MA, Savage TM, Simpson BR, Goodwin R. Controlled sedation with alphaxolone-alphadolone. Br Med J 1974;2:656-659.
- Kamibayashi T, Maze M. Clinical uses of alpha-2 adrenergic agonist. Anesthesiology 2000;93:1345-9.
- Scafati A. Analgesia and alpha agonist 2. Medens Rev 2004;4-7.
- Hall JE, Uhrich TD, Ebert TJ. Sedative analgesic and cognitive effects of clonidine infusions in humans. Br. J Anesth 2001;86:5-11.
- Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative amnesic and analgesic properties of small dose dexmedetomidine infusions. AnesthAnalg 2000;90:699-705.
- Mauro VA, Brandai ST. Clonidine and dexmedetomidine through epidural route for post-operative analgesia and sedation in a colecistectomy. Rev Bras Anesthesiol 2004;4:1-10.
- Gabriel JS, Gordin V. Alpha 2 agonist in regional anesthesia and analgesia. CurrOpinAnesthesiol 2001;14:751-3.
- Getler R, Brown HC, Mitchell DH, Silvius EN. Dexmedetomidine: A novel sedative-analgesic agent. Proc (BaylUniv Med Cent) 2001;8:13-21.
- Paris A, Tonner PH. Dexmedetomindine in anesthesia. CurrOpinAnesthesiol 2005;18:412-8.
- Coskuner I, Tekin M, Kati I. Effects of dexmedetomidine on the duration of anesthesia and wakefulness in bupivacaine epidural block. Eur J Anesthesiol 2007;24:535-40.
- El-Hennawy AM, Abd-Elwahab AM, And-Elmaksoud AM, El-Ozairy HS, Boulis SR. Addition of clonidine or dexmedetomidine to bupivacaine prolongs caudal analgesia in children. Br J Anesth 2009;103:268-74.
- Sia AT. Optimal dose of intrathecal clonidine added to sufentanmil plus bupivaccaine for labor analgesia. Can J Anesth 2000;47:875-80.
- Benhamou D, Thorin D, Brichant JF, Dailand P, Milon D, Schneider M. Intrathecalclonidine and fentanyl with hyperbaric bupivacaine improves analgesia during cesarean section. AnesthAnalg 1998;87:609-13.
- Aantaa R, Kanto J, Scheinin M, Kallio A, Scheinin H. Dexmedetomidine, an alpha 2-adrenoceptor agonist, reduces anesthetic requirements for patients undergoing minor gynecologic surgery. Anesthesiology 1990;76:230-5.
- SukhminderBajwa, Sukhwinder K. Bajawa, Jasbir Kauri, Gurpreet Sigh, VikramjitArora, Sachin Gupta, AshishKulshreStha, Amarjit Singh, SS Parmar, Anita Singh, SPS Goraya. Dexmedetomidine and clonidine in epidural anesthesia: A comparative evaluation. Indian Journal of Anesthesia 2011;55:116-121.
- DilekMemis, AlparslanTuran, BeyhanKaramanlioglu, ZaferPamukcu and Imran Kurt. Adding dexmedetomidine to lidocaine for intravenous regional anesthesia. AnesthAnalg 2004;98:835-40.
- Mauro VA, Brandao ST. Clonidine and dexmedetomidine through epidural route for post-operative analgesia and sedation in acolecistectomy. Rev. Bras Anesthsiol 2004;4:1-10.
- Gabriel JS, Gordin V. Alpha 2 agonist in regional anesthesia and analgesia. CurrOpinAnesthesiol 2001;14:751-3.
- Oriol-Lopez, Maldonado-Sanchez, CE Hernandez, JA Caslelazo A, and L Moctezuma. Epidural dexmedetomidine in regional anesthesia to reduce anxiety. RevistaMexicanadeAnesthesiologia 2008;31:271-277.
- Brummett CM, Norat MA, Palmisano JM, Lydic R. Perineural administration of dexmedetomidine in combination with bupivacaine enhances sensory and motor blockade in sciatic nerve block without inducing neurotoxicity in rat. Anesthesiology 2008;109:502-511.
- Obayah GM, Rafaie A, Aboushanab O, Ibraheem N and Mossad A. Addition of dexmedetomidine to bupivacaine for greater palatine nerve block prolongs postoperative analgesia after cleft palate repair. European Society of Anesthesiology 2010;27:1-5.





