Dexmedetomidine-based Total Endovenous Anesthesia in Radical Surgery for Breast Cancer. An observational case series study involving 10 patients.
Perez-Arellano J1, Torres-Hernandez R1, Anaya-Martel E1**, Bermea-Perez E2**, Navarrete-Aleman J2, Sanchez-Valdivieso E2,3*.
1 Department of Anesthesia,Ministry of Health’s High Specialty Hospital, Veracruz City, Mexico.
2 Department of Oncology, Ministry of Health’s High Specialty Hospital, Veracruz City, Mexico.
3 Department of Research, Cristobal Colon University School of Medicine, Boca del Rio, Mexico.
** AME is Senior Resident in Anesthesiology; BPEA is Senior Resident in General Surgery.
*Corresponding Author
Enrique A. Sanchez-Valdivieso M.D., Ph.D.,
Paseos del Campestre, Condominio Costa No.40,
Fracc. Paseos del Campestre, Medellin de Bravo,
Veracruz, Mexico.
Tel: +52 229 2021260; Fax: +52 229 2021260
E-Mail: easanchezv@gmail.com
Article Type: Research Article
Received: August 27, 2014; Accepted: October 12, 2014; Published: October 14, 2014
Citation: Sanchez-Valdivieso E A et al (2014) The use of dexmedetomidine in radical surgery for breast cancer. Int J Anesth Res. 2(7), 63-67. doi: dx.doi.org/10.19070/2332-2780-1400016
Copyright: Sanchez-Valdivieso E A© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Ambulatory treatment of breast cancer is limited by vomiting and post-operative pain, and general anesthesia is implicated in these effects. Dexmedetomidine supplies analgesia and sedation without respiratory depression when it is administered intravenously. We demonstrate the usefulness of Dexmedetomidine as a general endovenous anesthesia.
Methods: Female patients were included with ages ranging between 42 and 83 years old and with a breast cancer diagnosis. They werescheduled for radical surgery between May 2009 and April 2011. Dexmedetomidine plus Propofol and Fentanyl were administered.
Intra-operative monitoring included electrocardiography, arterial blood gas analysis, blood pressure, heart rate, respiratory rate, and arterial oxygen saturation. We registered surgery and sedation according to the bispectralindexand Ramsay scales.
Results: The patients were maintained with 95% oxygen saturation and breathed spontaneously during the entire procedure with supplementary oxygen.Their blood pressure remained constant;heart rate showed only a mild reduction, bispectral index was maintained at 50, and the Ramsey scale-at IV. The infusion was discontinued without the patients experiencing dizziness or vomiting; the patients had an easy response-to-voice a wakening and remained in the recovery room for at least 2 h. They were physiologically stable, and were left with additional supplementary oxygen. There was no pain or agitation observed during the recovery period and no narcotic was administered.
Conclusion: Dexmedetomidine is a useful intravenous anesthetic agent in procedures such as radical breast surgery, with faster recovery and residual analgesia.
2.Introductiont
3.Case Series
4.Anesthetic procedure
5.Statistical Analyses
6.Discussion
7.Limitations of this study
8.Conclusion
9.Acknowledgments
10.References
Keywords
General Anesthesia; Intravenous Anesthetics, Dexmedetomidine; Breast Cancer.
Introduction
In the U.S, cancer is the second most common cause of death (one of every four deaths), only surpassed by cardiac disease [1]. The most frequent cancer in women is breast cancer and it is estimated that 30 - 40% of patients with breast cancer will die of metastatic disease [2]. Due to the high number of patients annually hospitalized for surgical treatment of breast cancer, efforts have been focused on reducing hospital costs and hospital stay time [3]. Breast surgery as an ambulatory procedure, however, has been limited because of the presence of nausea, vomiting, and post-operative pain. General anesthesia can be primarily implicated in these effects and its emetic properties have the highest incidence in women, particularly in patients with breast surgery [4].
Dexmedetomidine (Precedex; Hospira, Inc., Lake Forest, IL,USA) is a selective α2 adrenoceptor agonist with unique properties. Dexmedetomidine (DEX) provides analgesia and sedation without respiratory depression when it is administered intravenously (i.v.) [5,6].The U.S. Food and Drug Administration have approved DEX for procedural sedation in non-intubated patients and the approved dose for continuous i.v. sedation in intensive therapy in patients who are mechanically ventilated is a bolus of DEX (1 μg/kg) for administration in 10 min, followed by an infusion of 0.2–0.7 μg/kg/h [7]. Indications for DEX include premedication and as an adjuvant for general and regional anesthesia, with a sedative and analgesic effect. DEX has been employed as base anesthesia or unique anesthesia in short procedures as indicated by endoscopic studies, difficult upper airways surgeries, or in patients with morbid obesity [6], even at doses of 5–10μg/kg/h [5]. At excessive doses, At excessive doses, DEX does not cause significant
hemodynamic or respiratory adverese effects. Higher i.v.infusion has been described without harmful effects [5].
The objective of the present work is to report our experience in the management of radical breast cancer surgery with DEX in a series of patients.
Case Series
Ten non-smoker female patientsdiagnosed with breast cancer, regardless of age and clinical stage, scheduled to undergo radical breast surgery were included. TheInstitutional Ethics Committee approved the study; all patients gave written informed consent. The inclusion/exclusion criteria are depicted in table 1.
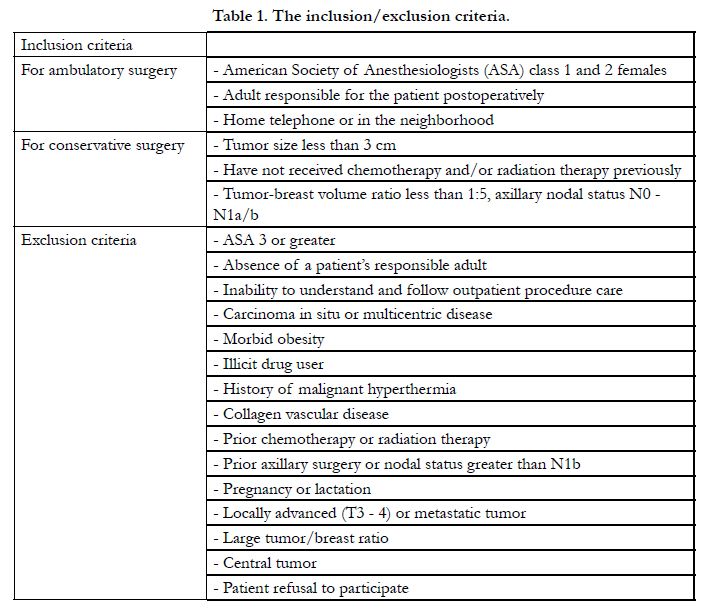

Table 1. The inclusion/exclusion criteria.
Mean age of the patients was 54.6 years (range 42 to 83 years).History was unremarkable for previous surgeries and for treatments with analgesics;there was no need to take analgesics 30 days prior to surgery. Pre-operative diagnosis included ductal carcinoma (eight patients) and lobular carcinoma (two patients). The clinico-pathological characteristics of the patients are depicted in table 2.
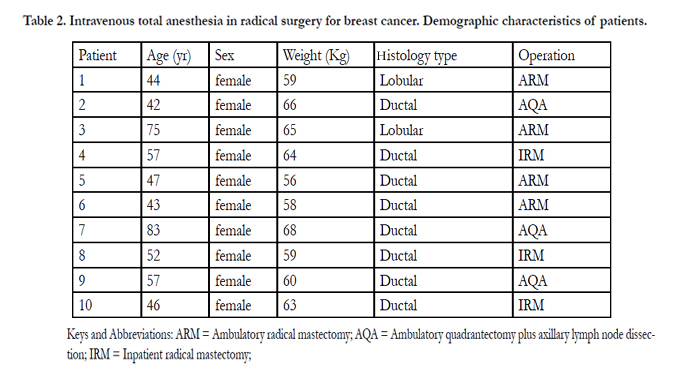
Table 2. Intravenous total anesthesia in radical surgery for breast cancer. Demographic characteristics of patients.
Keys and Abbreviations: ARM = Ambulatory radical mastectomy; AQA = Ambulatory quadrantectomy plus axillary lymph node dissection;IRM = Inpatient radical mastectomy;
Patients presented on the same day of their surgery. Intervention type was mastectomy in seven cases and quadrantectomy in the remaining three; all but three underwent a short-stay ambulatory surgery. The mean duration of surgical procedures was 135 min (range, 60–195 min) and no intra-operative complications were registered. Histopathological examination revealed negative margins on all of the mastectomy and quadrantectomy specimens.
Anesthetic procedure
In the pre-anesthetic care unitand after obtaining baseline measurement of heart rate (HR), respiratory rate (RR) and blood pressure (BP), DEX was startedwith a pre-induction dose of 1 μg/ kg/min by continuous i.v. infusion for 15 min immediately prior to breast surgery. The pre-induction doses were then followed by DEX infusion at 0.4 μg/kg/h. This resulted in conscious sedation without respiratory or cardiovascular compromise (Ramsay III/IV). Induction of anesthesia was performed using DEX, propofol (1 mg/kg-1), and fentanyl (2 μg/kg/h) without the need for endotracheal intubation, with the patients spontaneouslybreathingthroughout the procedure (oxygen saturation at >95%);the patient dozed, with easy response to the voice and integral consciousness. Intraoperatively, the anesthesia was maintained with DEX infusion at 0.5–0.7 μg/kg/h and, by an alternative intravenous route, propofol (1 μg/kg/min). Supplementary analgesia was achieved by administering fentanyl.Intraoperative sedation scoring was done every 10 minutes.The BIS index values between 40 and 60 indicated general anesthesia.When the patients were sedated (Ramsay IV, BIS 60), we proceeded to the radical mastectomy or quadrantectomy.The average DEX dose used was 200 ± 50 μg (0.3 - 0.5 μ/kg/min). Of note, BP was usually maintained with no significant variations during the whole procedure (table 3) and no significant changes or fluctuations were observed in HR. The BIS was maintained at 50 (range 42 to 64) and the Ramsay level was maintained at IV during the entire procedure.
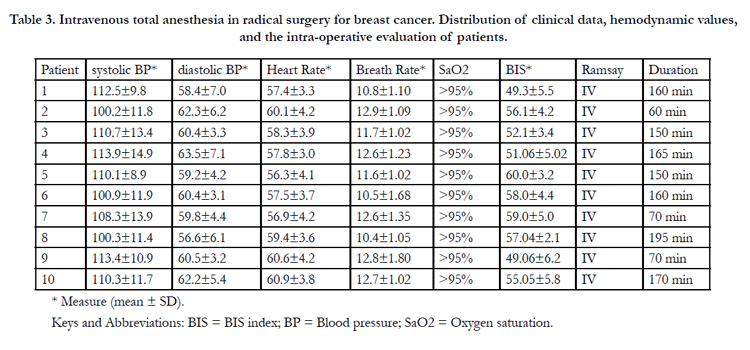
Table 3. Intravenous total anesthesia in radical surgery for breast cancer. Distribution of clinical data, hemodynamic values,and the intra-operative evaluation of patients.
* Measure (mean ± SD).
Keys and Abbreviations: BIS = BIS index; BP = Blood pressure; SaO2 = Oxygen saturation.
At the end of the surgical procedure,propofol and DEX infusions were discontinued with patients spontaneously breathing without dizziness, nausea, or vomiting; therefore, there was no need for postoperative nausea and vomiting management.Ketorolac, (if requested by patient) was the endovenous postoperative analgesic administered in the post-anesthetic care unit (PACU).Patients recovered were maintained for at least 2 h. They were asked to rate their pain on a 0 to 10 numeric rating scale, with 0 representing "no pain" and 10 "the worst possible pain"; average pain was 0/10 at 1 h and 2/10 at 3 h, when the patients were discharged from PACU. An oral antibiotic was indicated (Cephalexin, 500 mg four times daily) for 5 days and oral Ketorolac in case of need. Patients scheduled for ambulatory surgery were discharged from the hospital after a PACU stay of approximately 3 h..
Statistical Analyses
Variables are expressed in terms of the mean and standard deviation. The Kolmogorov–Smirnov test was used to test the normal distribution of data. Comparisons of ordered data were performed by the Wilcoxon–Mann–Whitney test. Categorivcal data were analyzed by the Fisher’s exact test. Serial measurements and changes in the vital measurements from baseline were analyzed by using one-way analysis of variance (ANOVA). Significance was expressed byP-values. P-values < 0.05 were considered statistically significant.
Discussion
The sedative effect of DEX is similar to that of natural sleep; subjects under sedation with DEX awaken easily on their being stimulated and return to the sedation state rapidly. Superficial sedation with easy awakening employing DEX is preferable for certain patients due to the lack of respiratory depression. Similarly, some of the accompanying effects (low BP, diminution of HR, dryness of mucosas) can, in certain cases, be of clinical usefulness. Recovery time with DEX is comparable with other anesthesia types, but with softer emersion without the need of a narcotic [10]. Adding a small dose of Propofol i.v. to the DEX aids in achieving better surgical conditions and diminishes the doses of both drugs necessary for obtaining an optimal surgical state.
The analgesic effect of DEX has also been reported as a main parameter during monitorized anesthetic care and after major surgical procedures [11-13]. Administration of DEX prior to the end of a major surgical procedure associated with post-operative pain reduced the early post-operative need for morphine by 66%; additional analgesia is not needed in the first hour of recovery [14]. Other groups [15-17] have already reported the use of intraoperative DEX infusion in laparoscopic bariatric surgery and supratentorial craniotomiesbut followed by tracheal intubation, different from our procedure with no patient necessitating invasive respiratory support.
Conventional sedation point systems based on clinical observations may not work well with DEX-induced sedation [8]. The Ramsay scale (Ramsay Sedation Score) is characterized by significant interobserver variability [9]. The BIS is a number derived from the bispectral analysis of the EEG that provides information on the interactions between the cortical and subcortical area that change under the influence of sedatives and hypnotics [9]. Conscious sedation corresponds to a BIS index of 70 - 80 and general anesthesia is reflected by a BIS index within the range of 40 - 609. BIS values were approximately 20 points lower with DEX-induced sedation than with that induced by propofol [8]. Thus, BIS is considered very useful monitoring in these cases.
Some patients with breast cancer will carry micrometastasis up to the moment of the procedure.There are peri-operative period factors that can result in immunosuppression, promoting metastatic development [18]. The surgical act, then, can lead to the releasing of malignant cells within the blood and lymph node systems. This dissemination can become manifested with local and distant recurrences of the patient’s immunocompetence. It has been postulated that there can be a “decisive period” during which the microscopic disease cannot be controlled and it can remain during the development of recurrences. The recurrence of certain anesthetics can then be a factor for the success or failure in the control of this microscopic disease [19,20].
Propofol has to be combined with an opioid when it is utilized in total intravenous anesthesia and opioids possess various actions that can cause the dissemination of malignant cells [21,22]. Opioids suppress post-operative cytotoxicity in NK lymphocytes
in humans [23]. In addition, opioids stimulate angiogenesis and
tumor progression, in part via activating cyclooxygenase-2 and increasing the production of prostaglandin E2 [24]. In addition to diminishing the requirements of the anesthetic and opioid agents,DEX hypothetically could reduce the recurrence risk in breast cancer [25 ,26], via the α2 adrenergic effect on human mammary cells [27] as a significant increase in mammary tumor growth induced by clonidine in mouse have been described [28]. There is evidence that post-operative pain is an important mediator of the tumor promoter effects of surgery [29]; by extending postoperative anesthesia, DEX can attenuate the negative impact of post-operative pain.Patient outcomes in our study were characteristically associated with low postoperative pain scores, low PONV rates and short PACU lengths of stay; however, the primary outcomes of interest were neither the incidence of PONV nor the length of PACU stay.Moreover, no consideration was done on patients’ satisfaction using this technique.
In the decade of the eighties, 46.9 of the 117,982 patients submitted to mastectomy in the U.S. remained hospitalized for 6 or more days after the procedure and in 1995, 10.8% of mastectomies were ambulatory [30]. Since 1998, the routine use has been proposed of Ambulatory radical surgery (ARS) in breast cancer [31]. While only a modest increase (3 - 3.5%) in the proportion of readmitted patients [30], performing (ARS) has not been adopted in routine fashion, which would afford economic incentives, because this can result in substantial savings of means in times of economic crisis.
The technique used here is novel, with spontaneous breathing, on an outpatient basis and with no hemodynamic or respiratorycomplications. Several advantages of this technique have been observed: reduced requirements for intraoperative propofol and - fentanyl; there was no need for tracheal intubation and use of muscle relaxants; recovery time was comparable with that of other anesthesia types,but with softer emersion with DEX; a good 24-hour control of postoperative pain was achieved with lower requirements for analgesic support.
Limitations of this study
The main limitation of our study was the small number of cases. The fact that only 10 patients were studied makes it underpowered and difficult to make a conclusion on whether dexmedetomidine actually helped these patients. Nevertheless, we believe that this method is promising. Our preliminary results are encouraging and further studies are desirable.
Conclusion
DEX is a useful anesthetic/analgesic not only as an adjuvant to anesthesia, but also as a unique anesthetic agent, for short procedures including difficult endoscopic procedures, surgery on upper airways obese patients, as well as for major procedures such as radical and extensive surgeries for cancer with an important shortening of the recovery period and affording the opportunity of performing ambulatory radical surgery for breast cancer, which has been attempted for two decades [32].
Acknowledgments
* Assistance with the study:none.
* Financial support and sponsorship:none.
* Conflict of interest:none declared.
References
- American Cancer Society. Cancer Facts and Figures 2007. Atlanta: ACS,2007.
- Van Diest PJ, van der Wall E, Baak JPA (2004). Prognostic value of proliferation in invasive breast cancer: a review. J ClinPathol; 57: 675–681.
- Pedersen SH, Douville LM, Eberlein TJ (1994). Accelerated surgical stay programs: a mechanism to reduce health care costs. Ann Surg; 219: 374-381.
- Quinn AC, Brown JH, Wallace PG, Asbury AJ (1994). Studies in postoperative sequelae: nausea and vomiting –still a problema. Anesthesia; 49: 62-65.
- Ramsay MA, Luterman DL (2004): Dexmedetomidine as a total intravenous anesthetic agent. Anesthesiology; 101:787–790
- Ramsay MA, Saha D, Hebeler RF (2006): Tracheal resection in the morbidly obese patient: The role of dexmedetomidine. J ClinAnesth; 18:452–454.
- Brummett CM,Padda AK,Amodeo FS,Welch KB, Lydic R (2009).Perineural Dexmedetomidine added to Ropivacaine causes a dose-dependent increase in the duration of thermal antinociception in sciatic nerve block in rat.Anesthesiology; 111: 1111-1119.
- Kasuya Y, Govinda R, Rauch S, Mascha EJ, Sessler DI, et al(2009). The correlation between bispectral index and observational sedation scale in volunteers sedated with dexmedetomidine and propofol. Anesth Anal; 109:1811-1815.
- Hernández-Gancedo C, Pestaña D, Peña N, RoyoC, Pérez-Chrzanowska H, et al(2006). Monitoring sedation in critically ill patients. Bispectral index,Ramsay and observer scales.Eur J Anesth; 23: 649-653.
- Shukry M,Kennedy K (2006). Dexmedetomidine as a total intravenous anesthetic in infants. Pediatric Anesthesia; 17: 581-583.
- Tobias JD, Berkenbosch JW (2002). Initial experience with dexmedetomidine in pediatric-aged patients.Pediatric Anesthesia; 12: 171-175.
- Venn RM, Bradshaw CJ, Spencer R, Brealey D, Caudwell E, et al (1999). Preliminary UK experience of dexmedetomidine, a novel agent for postoperative sedation in the intensive care unit. Anaesthesia; 54: 1136–1142.
- Aho MS, Erkola OA, Scheinin H, Lehtinen AM, Korttila KT (1991). Effect of intravenously administered dexmedetomidine on pain after laparoscopic tubal ligation. AnesthAnalg; 73: 112–118.
- Arain SR, Ruehlow RM, Uhrich TD, Ebert TJ (2004). The Efficacy of Dexmedetomidine Versus Morphine for Postoperative Analgesia After Major Inpatient Surgery.AnesthAnalg; 98: 153–158.
- Tufanogullari B, White PF, Peixoto MP, Kianpour D, Lacour T, et al (2008). Dexmedetomidine Infusion During Laparoscopic BariatricSurgery: The Effect on Recovery Outcome Variables. AnesthAnalg; 106: 1741–1748.
- Bakhamees HS, El-Halafawy YM, El-Kerdawy HM, Gouda NM, Altemyatt S (2007). Effects Of Dexmedetomidine In Morbidly Obese Patients Undergoing Laparoscopic Gastric Bypass. M.E.J. Anesth; 19: 537- 551.
- Turgut N, Turkmen A, Ali A, Altan A (2009). Remifentanil-Propofol Vs Dexmedetomidine-Propofol- Anesthesia For Supratentorial Craniotomy -. M.E.J. Anesth; 20: 63-70.
- Snyder GL,Greenberg S (2010). Effect of anaesthetic technique and other perioperative factors on cancer recurrence. Br J Anaesth; 105: 106–115.
- Biki B,Mascha E,Moriarty DC,Fitzpatrick JM, Sessler DI,et al (2008). Anesthetic Technique for Radical Prostatectomy SurgeryAffects Cancer Recurrence. A Retrospective Analysis.Anesthesiology; 109: 180–187.
- O’Rian SC, Buggy DJ, Kerin MJ, Watson RW, Moriarty DC (2005). Inhibition of the stress response to breast cancer surgery by regional anesthesia and analgesia does not affect vascular endotelial growth factor and prostaglandin E2. AnesthAnalg; 100: 244–249.
- Shapiro J, Jersky J, Katzav S, Feldman M, Segal S (1981). Anesthetic drugs accelerate the progression of postoperative metastases of mouse tumors. J Clin Invest; 68: 678–685.
- Sacerdote P, Bianchi M, Gaspani L, Manfredi B, Maucione A, et al (2000). The effects of tramadol and morphine on immune responses and pain after surgery in cancer patients.AnesthAnalg; 90: 1411–1414.
- Beilin B, Shavit Y, Hart J, Mordashov V, Cohn S, et al (1996). Effects of anesthesia based on large versus small doses of fentanyl on natural killer cell cytotoxicity in the perioperative period. AnesthAnalg; 82: 492–497.
- Amano H, Ito Y, Suzuki T, Kato S, Matsui Y, et al (2009). Roles of a prostaglandin E-type receptor, EP3, in upregulation of matrix metalloproteinase-9 and vascular endothelial growth factor during enhancement of tumor metastasis. Cancer Sci; 100: 2318–2324.
- Wu CL, Fleisher LA (2000). Outcomes research in regional anesthesia and analgesia. AnesthAnalg; 99: 1232–1242.
- Sessler DI, Ben-Eliyahu S, Mascha EJ, Parat MO, Buggy DJ (2008). Can regional analgesia reduce the risk of recurrence after breast cancer? Methodology of a multicenter randomized trial. ContempClin Trials; 29: 517–526.
- Vazquez SM, Mladovan AG, Perez C, Bruzzone A, Baldi A, et al (2006). Human breast cell lines exhibit functional alpha2- adrenoceptors. Cancer ChemotherPharmacol; 58: 50–61.
- Bruzzone A, Pinero CP, Castillo LF, Sarappa MG, Rojas P, et al (2008). Alpha2-adrenoceptor action on cell proliferation and mammary tumour growth in mice. Br J Pharmacol; 155: 494–504.
- Page GG, Blakely WP, Ben-Eliyahu S (2001). Evidence that postoperative pain is a mediator of the tumor promoting effects of surgery in rats. Pain; 90: 191–199.
- Warren JL, Riley GF, Potosky AL, Klabunde CN, Richter E, et al (1998). Trends and Outcomes of Outpatient Mastectomy inElderly Women. J Natl Cancer Inst; 90: 833–840.
- President, Congress decry practice of ‘‘drive-through mastectomies.’’ The Cancer Letter 1997 Feb 21; 1.
- Goodman AA, Mendez AL (1993). Definitive surgery for breast cancer performed on an outpatient basis. Arch Surg; 128: 1149–1152.





