Incidence and Risk Factors of Severe Bradycardia During Spinal Anesthesia with Chronic
β-Blockade
Lee JH1*, Nam Da Jeong2, Park Jungho2
1 Clinical Assistant Professor, Department of Anesthesiology and Pain Medicine, National Health Insurance Corporation, Ilsan Hospital, Republic of Korea.
2 Department of Anesthesiology and Pain medicine, Yonsei University College of Medicine, Republic of Korea.
*Corresponding Author
Jae Ho Lee M.D,
Clinical Assistant Professor,
Department of Anesthesiology and Pain Medicine,
National Health Insurance Corporation, Ilsan Hospital,
100 Ilsan-ro, Ilsan-donggu, Goyang-si, Gyeonggi-do, 410-719,
Republic of Korea.
Tel: +82 31 900 0299
Fax: +82 31 900 0319
E-mail: lijhmd71@hotmail.com and lijhmd@nhimc.or.kr
Article Type: Research Article
Received: April 20, 2015; Accepted: May 20, 2015;Published: May 22, 2015
Citation: Lee JH, Nam Da Jeong, Park Jungho (2015) Incidence and Risk Factors of Severe Bradycardia during Spinal Anesthesia with Chronic β-blockade. Int J Anesth Res. 3(4), 105-108. doi: dx.doi.org/10.19070/2332-2780-1500027
Copyright: Lee JH© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Severe bradycardia and asystole after spinal anesthesia was considered a serious side effect. Beta (β)-blockers lower blood pressure with decrease resting heart rate and left ventricular function. In this study, we retrospectively recorded the incidence of severe bradycardia and asystole during spinal anesthesia in patients medicated with β-blockers and investigated risk factors contributing to the incidence of severe bradycardia.
Methods: Anesthesia chart of 693 cases were retrospectively examined. All patients receive elective surgery in our institute ith spinal anesthesia and received β-blockers until the day of operation. Bradycardia was defined as a heart rate <50 beats per minute for at least 1 minute. Ten variables as risk factors contributing to bradycardia were selected: gender, age, body mass index, spinal drug dose, and peak sensory block height, baseline heart rate, baseline systolic blood pressure, baseline diastolic blood pressure, baseline mean blood pressure, and history of diabetes.
Results: Eighty six of the 693 (13.4%) patients experienced bradycardia. No asystole occurred. On univariate analysis, male gender, absence of diabetes, low baseline heart rate was associated with statistically higher incidence of bradycardia. In multivariate logistic regression, low baseline heart rate, absence of diabetes elevated the risk of bradycardia (Odds Ratio, 10.44 and 2.6 respectively).
Conclusions: The incidence of severe bradycardia during spinal anesthesia was 13.4% in the patient receiving the β-blockers. Those with low baseline heart rate and absence of diabetes were more vulnerable to develop severe bradycardia.
2.Introduction
3.Materials and Methods
4.Results
5.Discussions
6.Conclusion
7.Acknowledgement
8.References
Keywords
Bradycardia; Spinal Anesthesia; Beta-Blocker.
Introduction
Spinal anesthesia has been considered a safer technique than general anesthesia. But, it has many side effects too. These are hypotension, bradycardia, nausea, vomiting, and neurologic injury [1,2].
Severe bradycardia asystole after induction of spinal anesthesia can cause serious consequences [3, 4]. Studies and case reports of this bradycardia and asystole have been published, but the exact causes and mechanisms remain unclear [5-8].
Beta (β)-blockers are among the most commonly prescribed drug in patients presenting for surgery [9, 10]. Its indications include ischemic heart disease, postinfarction management, hypertrophic cardiomyopathy, heart failure and hypertension. β-blockers lower blood pressure with a decrease in resting heart rate and left ventricular function. Therefore, patients who take β-blockers at the time of surgery with spinal anesthesia may be more vulnerable to severe bradycardia and asystole during surgery than the patients who do not.
In this study, we retrospectively recorded the incidence of severe bradycardia and asystole during spinal anesthesia in patients who received β-blockers. and investigated the risk factors contributing to the incidence of severe bradycardia.
Materials and Methods
This was a single-center, retrospective study designed to find out the incidence and risk factors of severe bradycardia during spinal anesthesia in patients who received β-blockers. The Institutional Review Board of our institute approved the study protocol (approval date: 2014, September, 23; approval number: Suyon 2014-166). Anesthesia chart from March, 2009 to June, 2014, involving 693 cases were retrospectively examined. All patients receive elective surgery in our institute with spinal anesthesia and took β-blockers until the day of operation. Bradycardia was defined as a heart rate <50 beats per minute for at least 1 minute. Ten variables were selected as risk factors contributing to bradycardia: gender, age, body mass index (BMI), spinal drug dose (0.5% hyperbaric bupivacaine), peak sensory block height, baseline heart rate (HR), baseline systolic blood pressure (SBP), baseline diastolic blood pressure (DBP), baseline mean blood pressure (MBP), history of diabetes (DM). Blood pressure was measured and recorded every 5 minute and heart rate was measured continuously but recorded every 5 minute. All data concerning incidence of bradycardia, heart rate of bradycardia during entire period of anesthesia and variables were recorded by expert anesthesiologists. We excluded all possible influences to heart rate of the patients.
Patients who medicated any other cardiac drugs except β-blocker preoperatively, who received opioids and benzodiazepines preoperatively and intraoperatively, who were premedicated with glycopyrrolate or atropine, obstetric patients, cases in which epinephrine additive to spinal local anesthetics, use general anesthesia after spinal anesthesia, and loss of at least one of the variables on the anesthesia chart were criteria for exclusion.
For the purpose of analysis, patients were separated into groups based on age (<65 and ≥65years), BMI (<25 and ≥25kg/m2), baseline heart rate (<60 and ≥60 beats per minute), baseline SBP (<150 and ≥150 mmHg), baseline DBP (<90 and ≥90 mmHg), baseline MBP (<110 and ≥110 mmHg), spinal drug dose (<12 and ≥12 mg), and peak sensory block height (<T5, and ≥T5). We chose T5 to divide peak sensory height because T5 is the lowest level of cardiac acceleration fiber.
Summary statistics were performed to identify the correlation between bradycardia and the 10 variables. Because all patients were grouped by each variable, they were assessed by chi-square or Fisher’s exact test. Potentially significant variables (P < 0.10) after univariate intergroup comparisons were assessed by forward and backward stepwise multivariate logistic regression analyses. Data are presented as numbers (percentage) for results from the univariate analyses and odds ratio (95% confidence interval, CI) for those from the multivariate logistic regression analyses. The sensitivity and unbiased estimate of the logistic predicting model and the cutoff values of individual predictors from multivariate analysis were evaluated by area under the receiver operating characteristic curve (AUC) analysis. All tests were two-sided, and p< 0.05 were considered to indicate statistical significance. SPSS software (ver. 15.0 SPSS, Chicago, IL, USA) was used for statistical analysis.
Based on previous study, in which the incidence of bradycardia during spinal anesthesia taking in case of β-blockers was 17.6% [11], we assumed a 95% CI; allowable limit of error was 3% with an α of 0.05. According to this assumption, calculated sample size was 610. Considering the possibility of loss in the course of data collection, 693 cases were studied.
Results
Fifty one of the 693 cases, were excluded due to combined general anesthesia with spinal anesthesia (n=2), premedicated with grycopyrrolate or midazolam (n=30), use of epinephrine or fentanyl in 0.5% hyperbaric bupivacaine (n=10), and incomplete anesthesia chart (n=9). The remaining 642 cases were included. 86 patients experienced bradycardia, representing an incidence rate of 13.4%, and the lowest heart rate was 36 beats per minute. Asystole did not occur (Table 1). Among the 86 cases, 20 were administered ephedrine, atropine was given in one case, and glycopyrrolate was given in one case. Hemodynamic instability from the severe bradycardia did not happen and all of the patients received their scheduled surgery uneventfully.
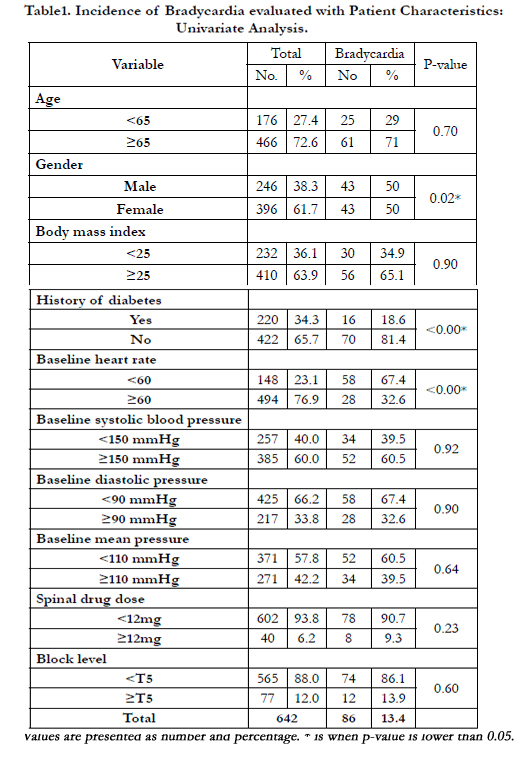

Table1. Incidence of Bradycardia evaluated with Patient Characteristics: Univariate Analysis.
On univariate analysis, male gender, absence of diabetes, low baseline heart rate were statistically associated with a higher incidence of bradycardia (p=0.02, <0.00, <0.00; Table 1). In multivariate logistic regression (Table 2), risk of bradycardia was elevated 10.44- fold (95% CI, 6.26 – 17.42) in the case of low baseline heart rate (<60 beats per minute). In cases where diabetes was absent, the risk of bradycardia was elevated 2.6-fold (95% CI, 1.40-4.81). For male gender, risk of bradycardia was elevated 1.65-fold (95% CI, 1.0-2.74), but was not statistically significant (p=0.06). The AUC curve was 0.79 (95% CI 0.73-0.84), which indicated the value of predicting the occurrence of bradycardia during spinal anesthesia (Figure 1).
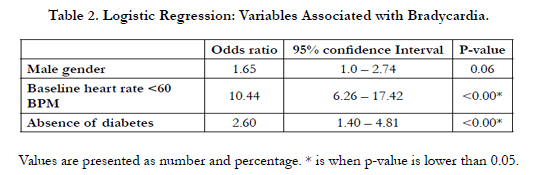
Table 2. Logistic Regression: Variables Associated with Bradycardia.
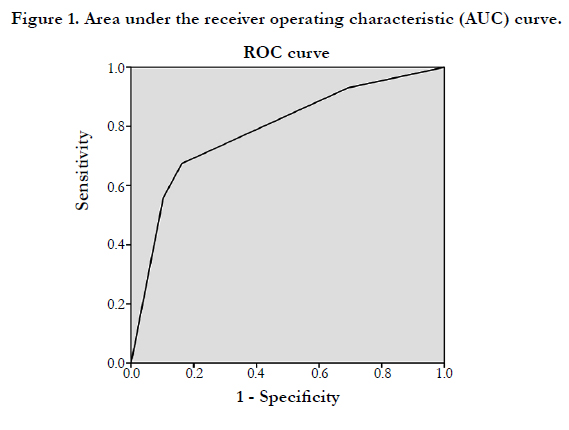
Figure 1. Area under the receiver operating characteristic (AUC) curve.
Discussions
Severe bradycardia and asystole are side effects of spinal anesthesia that can cause undesirable results [3, 8, 12]. β-blockers lower the resting heart rate. β-blockers may be a risk factor of severe bradycardia after spinal anesthesia [2, 11]. Therefore we retrospectively evaluated the incidence and risk factors of bradycardia after spinal anesthesia among the patients who received taking β-blockers.
The overall incidence of severe bradycardia of 13.4% is somewhat lower than previous studies. According to the lesser [11], the incidence of bradycardia (<50 BPM) was 17.3% (72 case in 416) during spinal and epidural anesthesia within the patients taking beta-blockers. Carpenter et al., [2] reported that the incidence of bradycardia (<50 BPM) was 23.6 % (25 cases in 106).
There may be several reasons for this difference. The mean age was our patients group (69.8 years) was much higher. We can assume that as age increased, vagal tone decreased, so the incidence of bradycardia will decrease. Secondary, contrary to other studies, there was fewer male gender. Male presently displayed a 1.6-fold increases in the odds of developing bradycardia. Finally, the number of patients who had peak sensory block level higher than T5 (62%) was much lower than the 20% reported previously [2]. The latter authors reported that low ASA classification and high peak sensory block height was risk factors of bradycardia with spinal anesthesia.
On regression analysis, baseline heart rate and the absence of diabetes were contributing variables affecting bradycardia during spinal anesthesia. Male gender increased the risk of bradycardia 1.65 fold but it was not statistically significant. This analysis was identical previous studies [2, 11]. History of diabetes with the absence of bradycardia is associated with cardiac denervation syndrome [13]. As the duration of diabetes lengthens, there is first an increase in parasympathetic tone which leads to increased heart rate. Subsequently, the heart rate decreases due to continued loss of sympathetic tone. Finally the heart is denervated completely, resulting in a fixed heart rate.
In the patients who are taking β-blockers, a baseline heart rate lower than 60 beats per minute was evident in 23.1%. In these patients, the incidence of bradycardia was 39%. Carpenter [2] reported a rate of this baseline heart rate of 10.6% (100 in 947 patients), regardless of β-blocker use. The incidence of bradycardia in that group was 37%. This result suggests that β-blockers lower the baseline heart rate, but do not specially lower the heart rate during spinal anesthesia.
Mackey et al., [7] suggested the Bezold-Jarisch reflex as the main causes of severe bradycardia and asystole after spinal anesthesia. This reflex paradoxically increases cardiac inhibitory neural activity from an underfilled hypercontractile left ventricle. Sensory receptors present in the heart; inhibitory receptors are associated with nonmyelinated C fiber that appears to constitute the afferent limb of the Bezold-Jarisch reflex. Many of these receptors, which result in increased vagal activity, can also be stimulated mechanically and by distortion of myocardium, such as low filling pressure, and rapid contraction of empty chamber [14]. Jacobsen [15] reported the effect of epidural anesthesia on left ventricular diameter in eight human volunteers using echocardiography. Two of the subjects developed bradycardia and hypotension with sensory level at T8 accompanied by a 22% reduction in the left ventricular diameter. These changes were reversed by rapid intravenous infusion of saline. Pathak [16] reported that with reduced atrial filling, stretch in the pacemaker region is reduced and heart rate decreased. This situation is compatible with reduced venous return, sympathetic blockade and venodilation normally associated with spinal or epidural anesthesia. Presently we were unable to check the amount of intravenous infusion around the time of spinal anesthesia and total intake and output balance during surgery. This is limitation.
Spinal anesthesia can inhibit the preganglionic sympathetic efferent limb of the autonomic nervous system. This can occur by blockade of cardiac accelerator fibers when the level of sympathetic blockade extends above T5 [11]. Presently the peak sensory level blockade was not associated with bradycardia. Carpenter [2] also indicated that this has the weakest correlation to bradycardia and suggested that the balance between sympathetic and parasympathetic tone may play an important role in susceptibility to development of bradycardia after spinal anesthesia.
Conclusion
In conclusion, the incidence of severe bradycardia during spinal anesthesia was 13.4% in patient receiving β-blockers. Hemodynamic instability did not occurred with bradycardia. But, nondiabetic patients with a low baseline heart rate were vulnerable to develop severe bradycardia.
Acknowledgement
This article was supported by the Ilan hospital research fund.
References
- Leroy D (1996) Complications of spinal and epidural anesthesia: complications in anesthesiology (1st edtn), Lippincott-Raven,philadelpfia.
- Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R (1992) Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology76(6): 906-916.
- Caplan RA, Ward RJ, Posner K, Cheney FW (1998) Unexpected cardiac arrest during spinal anesthesia: A closed claims analysis of predisposing factors. Anesthesiology 68(1): 5-11.
- Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, et al., (1997) Serious complications related to regional anesthesia: Results of a prospective survey in france. Anesthesiology 87(3): 479-486.
- Geffin B, Shapiro L (1998) Sinus bradycardia and asystole during spinal and epidural anesthesia: A report of 13 cases. J ClinAnesth 10(4): 278-285.
- Lovstad RZ, Granhus G, Hetland S (2000) Bradycardia and asystolic cardiac arrest during spinal anaesthesia: A report of five cases. ActaAnaesthesiolScand 44(1): 48-52.
- Mackey DC, Carpenter RL, Thompson GE, Brown DL, Bodily MN (1989) Bradycardia and asystole during spinal anesthesia: A report of three cases without morbidity. Anesthesiology 70(5): 866-868.
- Pollard JB (2001) Cardiac arrest during spinal anesthesia: Common mechanisms and strategies for prevention. AnesthAnalg 92(1): 252-256.
- Giles JW, Sear JW, Foex P (2004) Effect of chronic beta-blockade on perioperative outcome in patients undergoing non-cardiac surgery: An analysis of observational and case control studies. Anaesthesia 59(6): 574-583.
- Kadoi Y, Saito S (2010) Possible indications of beta-blockers in the perioperative period other than prevention of cardiac ischemia. J Anesth 24(1): 81-95.
- Lesser JB, Sanborn KV, Valskys R, Kuroda M (2003) Severe bradycardia during spinal and epidural anesthesia recorded by an anesthesia information management system. Anesthesiology 99(4): 859-866.
- Pollard JB (2002) High incidence of cardiac arrest following spinal anesthesia. Anesthesiology 96(2): 515-516.
- Broadstone VL, Roy T, Self M, Pfeifer MA (1991) Cardiovascular autonomic dysfunction: Diagnosis and prognosis. Diabet Med 8(2): S88-893.
- Thoren P (1979) Role of cardiac vagal C-fibers in cardiovascular control. Rev Physiol Biochem Pharmacol 86: 91-94.
- Jacobsen J, Sofelt S, Brocks V, Fernandes A, Warberg J, et al., (1992) Reduced left ventricular diameters at onset of bradycardia during epidural anaesthesia. Acta Anaesthesiol Scand 36: 831-836.
- Pathak CL (1973) Autoregulation of chronotropic response of the heart through pacemaker stretch. Cardiology 58: 45-64.





