Subcutaneous benign Fibrous Histiocytoma of upper eyelid: A Review of the histopathological Database at a Single Faculty in Japan
Honma M*, Minami-Hori M, Komatsu S, Hashimoto M, Ishida-Yamamoto A
Department of Dermatology, Asahikawa Medical University, Midorigaoka-Higashi, Asahikawa, Japan.
*Corresponding Author
Masaru Honma MD PhD,
Department of Dermatology,
Asahikawa Medical University,
2-1-1-1 Midorigaoka-Higashi, Asahikawa 078-8510, Japan.
Tel: +81-166-68-2523
Fax: +81-166-68-2529
E-mail: wanwan@asahikawa-med.ac.jp
Article Type: Case Report
Received: May 26, 2015; Accepted: June 20, 2015; Published: June 24, 2015
Citation: Honma M, et al., (2015) Subcutaneous benign Fibrous Histiocytoma of upper eyelid: A Review of the Histopathological Database at a single faculty in Japan. Int J Clin Dermatol Res. 3(3), 65-67. doi: dx.doi.org/10.19070/2332-2977-1500017
Copyright: Honma M© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A 57 year-old Japanese man presented with an asymptomatic, ϕ7 mm subcutaneous nodule on his right upper eyelid.
Findings of histopathology and immunohistochemistry led to the diagnosis of benign fibrous histiocytoma (BFH) (i.e. dermatofibroma).
At the department of dermatology, Asahikawa Medical University, 803 lesions of 777 cases have been registered as BFH with histopathological database. Nine lesions (1.12%) occurred on the face and only the present case showed subcutaneous facial BFH. While 5 cases of disseminated BFH associated with autoimmune diseases, exemplified by systemic lupus erythematosus, showed multiple lesions on the trunk and extremities, the face was completely spared, suggesting distinct histogenesis. However, immunohistochemistry for the markers associated with BFH, such as CD34, factor XIIIa, podoplanin, S-100, α-smooth muscle actin, and CD68, could not determine any difference from typical BFH.
Subcutaneous BFH on the face is extremely rare, however, both facial and subcutaneous BFH show more frequent recurrence rate than the classical subtype. Surgeon should be aware of BFH as one of subcutaneous tumors on the face, and careful observation is mandatory following surgical excision. (175 words)
2.Introduction
3.Case Report
4.Analysis of BFH lesions registered with the histopathological database at the department of dermatology, Asahikawa Medical University
5.Discussion
6.References
Keywords
Dermatofibroma; Podoplanin; D2-40; Face.
Introduction
Benign fibrous histiocytoma (BFH) (i.e. dermatofibroma) is one of the most common cutaneous tumors with clonal cellular proliferation [1]. It usually occurs in dermis of trunk or extremities, and subcutaneous or facial lesions are extremely rare [2]. Here, we report a case of subcutaneous BFH on upper eyelid. In addition, BFH registered with the histopathological database at the department of dermatology, Asahikawa Medical University were reviewed and analyzed using immunohistochemistry.
Case Report
A 57 year-old Japanese man presented with an asymptomatic, ϕ7 mm, skin-colored, elastic hard, subcutaneous nodule on his right upper eyelid (Figure 1). He had noticed the lesion without any trigger or preceding change a year ago. Computed tomography revealed a ϕ7 mm, subcutaneous isodensity nodule adjacent to the frontal bone. The nodule was excisionally removed and the histopathology showed a non-encapsulated, unclearly defined fibrous tumor consisted of striform-arranged collagen bundles, spindleshaped fibroblasts, histiocytes and multinucleated giant cells without any cell atypia or increased mitotic figures (0-1/HPF). Immunohistochemistry revealed that the tumor is strongly positive for factor XIIIa, CD68 and podoplanin (clone D2-40), but not for CD34, α-smooth muscle actin and Bcl-2. These clinical and histopathological findings led to the diagnosis of subcutaneous BFH arising on the upper eyelid.
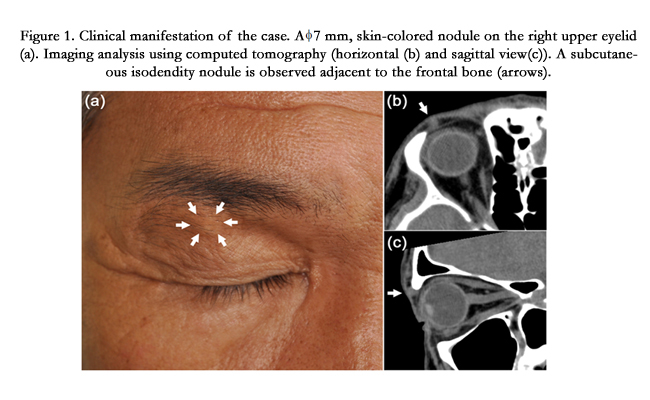
Figure 1. Clinical manifestation of the case. A ϕ7 mm, skin-colored nodule on the right upper eyelid (a). Imaging analysis using computed tomography (horizontal (b) and sagittal view(c)). A subcutaneous isodendity nodule is observed adjacent to the frontal bone (arrows).
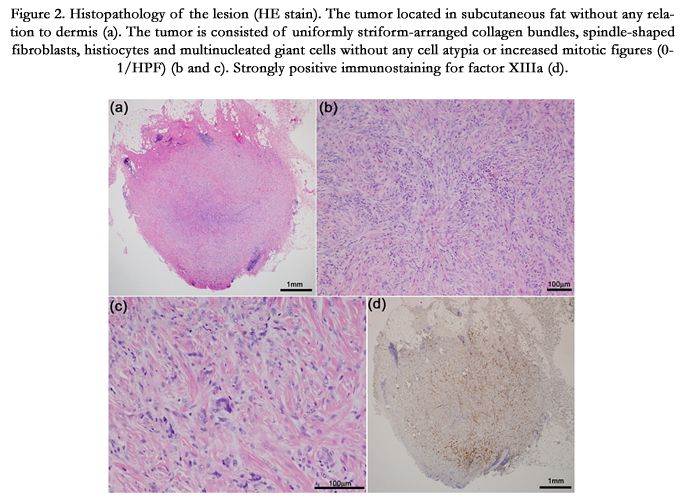
Figure 2. Histopathology of the lesion (HE stain). The tumor located in subcutaneous fat without any relation to dermis (a). The tumor is consisted of uniformly striform-arranged collagen bundles, spindle-shaped fibroblasts, histiocytes and multinucleated giant cells without any cell atypia or increased mitotic figures (0-1/HPF) (b and c). Strongly positive immunostaining for factor XIIIa (d).
Analysis of BFH lesions registered with the histopathological database at the department of dermatology, Asahikawa Medical University
Since 1978, 803 lesions of 777 cases have histopathologically been diagnosed as BFH at the department of dermatology, Asahikawa Medical University. Only nine lesions (1.12%) including the present case occurred on the face, and 525 lesions (65.5%) and 232 lesions (28.9%) arose on the extremities and the trunk, respectively. While five cases (0.64%) show disseminated BFH related to autoimmune diseases, such as systemic lupus erythematosus, the face was completely spared even in these cases. Six lesions of nine facial BFH showed relatively deep dermal lesions without typical epidermal hyperplasia and basal pigmentation as observed in conventional BFH. Immunohistochemistry for CD34, factor XIIIa, podoplanin, S-100, α-smooth muscle actin, and CD68 performed on the 7 lesions of facial BFH, in which immunostaining could be carried out, does not show any distinct features from typical BFH (Table 1).
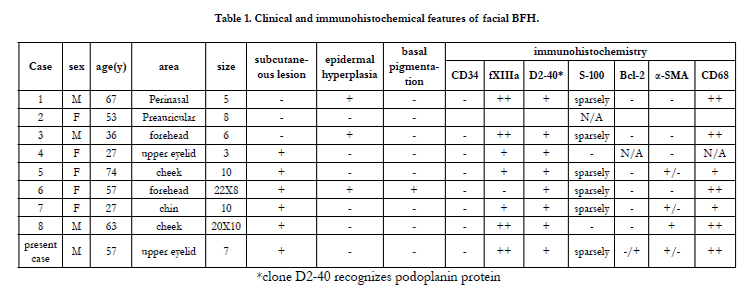

Table 1. Clinical and immunohistochemical features of facial BFH.
Discussion
BFH is the most frequent cutaneous mesenchymal tumor which mainly occurs on extremities suggesting close relation with minor trauma. According to the histopathological database of our faculty, 94.4% of BFH arose on the extremities and the trunk, and only 1.12% of BFH occurred on the face. Interestingly, even in disseminated cases associated with autoimmune disease, the face was completely spared, suggesting site-specific pathomechanism. According to a single center analysis in Germany, facial BFH is extremely rare and accounts for only 0.1% of total BFH [3]. Since surgical removal of facial BFH is most likely to be performed especially for cosmetic reasons, the actual occurrence rate of facial BFH might be much less than these numbers.
Subcutaneous or deep BFH is an uncommon variant, which ratio is estimated as 1% of all BFH [4]. Subcutaneous BFH on the face is much less and only 13 cases have been reported [5]. Six lesions of nine facial BFH diagnosed in our department showed relativelydeep dermal lesions without epidermal hyperplasia as described previously [3]. In the six lesions, subcutaneous tissues and muscle were involved. Only the present case was confined to subcutaneous tissue. This case is the second case of subcutaneous BFH arising on periorbital area [5].
Histogenesis of subcutaneous BFH is not fully elucidated. The previously reported subcutaneous BFH arising on eyebrow area involved supratrochlear nerve [5], whereas the present case did not show any close association with peripheral nerve. Immunostaining of S-100 protein, one of marker proteins for both dermal dendritic cells and Schwann cells, was sparsely positive in our study suggesting mixture of dermal dendritic cells in the tumor. Immunohistochemistry of the facial BFH lesions for other marker proteins associated with BFH failed to determine any specific features distinct from classical BFH lesions (Table). On the periorbital area, several more invasive fibrous tumors, such as solitary fibrous tumor (SFT), should be excluded. Histological features, such as a striform pattern with uniform cellularity or paternless with variety of cellularity, are the point to distinguish BFH from SFT [6]. Immunostaining for CD34 and Bcl-2 is usually negative in the former but positive for both markers in the latter [7], but CD34 can be positive in 40% of deep BFH [6]. Novel markers, such as podoplanin recognized by D2-40 monoclonal antibody [8], might additionally be informative for the differential diagnosis. Immunostaining for podoplanin shows strong and uniform positivity in almost all of BFH [8], but focally positive in a part of SFT cases [9]. In this study, all of facial BFH are uniformly positive for D2-40 staining.
Subcutaneous BFH on the face is extremely rare, however, reflecting the infiltrative feature into subcutaneous tissues, both facial and subcutaneous BFH show more frequent recurrence rates than the conventional subtype. Surgeon should be aware of BFH as one of subcutaneous tumors on the face, and careful observation is indispensable following surgical excision.
References
- Vanni R, Fletcher CD, Sciot R, Dal Cin P, De Wever I, et al. (2000) Cytogenetic evidence of clonality in cutaneous benign fibrous histiocytomas: a report of the CHAMP study group. Histopathology 37(3): 212-217.
- Han TY, Chang HS, Lee JH, Lee WM, Son SJ (2011) A clinical and histopathological study of 122 cases of dermatofibroma (benign fibrous histiocytoma). Ann Dermatol 23(2): 185-192.
- Mentzel T, Kutzner H, Rütten A, Hügel H (2001) Benign fibrous histiocytoma (dermatofibroma) of the face: clinicopathologic and immunohistochemical study of 34 cases associated with an aggressive clinical course. Am J Dermatopathol 23(5): 419-426.
- Fletcher CD (1990) Benign fibrous histiocytoma of subcutaneous and deep soft tissue: a clinicopathologic analysis of 21 cases. Am J Surg Pathol 14 9): 801-809.
- Ito T, Yoshida Y, Furue M, Yamamoto O (2013) Subcutaneous benign fibrous histiocytoma showing nerve involvement on the eyebrow region. Acta Derm Venereol 93(3): 371-372.
- Gleason BC, Fletcher CD (2008) Deep "benign" fibrous histiocytoma: clinicopathologic analysis of 69 cases of a rare tumor indicating occasional metastatic potential. Am J Surg Pathol 32(3): 354-362.
- Krishnakumar S, Subramanian N, Mohan ER, Mahesh L, Biswas J, et al. (2003) Solitary fibrous tumor of the orbit: a clinicopathologic study of six cases with review of the literature. Surv Ophthalmol 48(5): 544-554.
- Bandarchi B, Ma L, Marginean C, Hafezi S, Zubovits J, et al. (2010) D2- 40, a novel immunohistochemical marker in differentiating dermatofibroma from dermatofibrosarcoma protuberans. Mod Pathol 23(3): 434-438.
- Naito Y, Ishii G, Kawai O, Hasebe T, Nishiwaki Y, et al. (2007) D2-40-positive solitary fibrous tumors of the pleura: diagnostic pitfall of biopsy specimen. Pathol Int 57(9): 618-621.





