Effect of Induced Refractive Error and Nuclear Sclerotic Cataracts on Ishihara Colour Plate Testing
Eneh AA, Rogalska T, Urton T, Schweitzer KD*
Queen’s University Ophthalmology, Kingston, Ontario, Canada.
*Corresponding Author
Kelly Schweitzer,
Hotel Dieu Hospital,
166 Brock St., Kingston, ON, Canada.
Tel: 613-544-3310
E-mail: schweitk@hdh.kari.net
Article Type: Research Article
Received: April 09, 2014; Accepted: April 28, 2014; Published: April 30, 2014
Citation: Schweitzer KD , Eneh A, Rogalska T, Urton T. (2014). Effect of Induced Refractive Error and Nuclear Sclerotic Cataracts on Ishihara Colour Plate Testing, Int J Ophthalmol Eye Res, 2(1), 14-16. doi: dx.doi.org/10.19070/2332-290X-140003
Copyright: Schweitzer KD© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To determine the effect of induced refractive blur and nuclear sclerotic (NS) cataracts on Ishihara colour plate (ICP) scores. Design: Prospective evaluation of a diagnostic test
Participants: Patients who presented to Hotel Dieu Hospital Eye clinic between January and March 2010 with either a lone diagnosis of
nuclear sclerotic cataracts, or with no identified ocular disease with complete examination.
Methods: Patients were divided into two groups: those having no identified ocular disease on examination, and those with a lone diagnosis of NS cataracts. The first group was refractively blurred with +3D, +6D, +9D and +12D lenses. Best corrected visual acuity (BCVA) at near and ICP scores was obtained from both groups.
Results: There were 20 patients in each group. BCVA at near and ICP values declined with increasing amounts of plus lenses as expected. With the application of the +3D, +6D, +9D, and +12D lenses, the association between ICP scores and BCVA at near decreased (-0.845, -0.678, -0.374, and -0.363 respectively). There was little clinical decline in absolute ICP scores until lenses of +9D (mean BCVA at near = 20/400) or greater were applied. The correlation between ICP scores and BCVA at near declines due to NS cataracts was -0.53.
Conclusion: ICP testing is valid to BCVA at near of 20/100 when the acuity decline is due solely to NS cataracts. Further study is required
to determine whether or not severe vision loss due to NS cataracts affects ICP scores and at what visual acuity.
2.Introduction
3.Methods
4.Results
5.Discussion
6.Acknowledgements and Disclosure
7.References
Keywords
Assessment; Cataracts; Colour Vision Defects; Colour Perception Tests; Low Vision.
Introduction
Ishihara Pseudoisochromatic Colour Plates (ICP) are one of the most commonly used clinical tools used to detect red-green colour vision defects. [1] It consists of a series of plates containing coloured dots of varying brightness. A figure is embedded among the dots, and it can only be detected by discriminating between different colours.
Impaired colour vision can have several causes including glaucoma [2], optic neuropathy [3], and diabetic retinopathy [4]. In patients with colour vision defects who have more than one ocular disease, the ophthalmologist must determine the exact cause of the colour vision defect. Conventional wisdom dictates that when a patient’s loss of colour vision is out of proportion to the loss of visual acuity, optic nerve involvement should be suspected. This was recently confirmed in a study by Almog and Nemet. [5]
However, in order to properly apply this rule of thumb, it is first necessary to determine the validity of Ishihara Colour Plate (ICP) testing in patients with low visual acuity. Accordingly, the goal of our study was to establish the validity of ICP tests in the setting of nuclear sclerotic (NS) cataracts as the sole cause of decreased visual acuity.
Methods
This study was a prospective evaluation of a diagnostic test. The research followed the tenets of the Declaration of Helsinki, and informed consent was obtained from all patients after explanation of the nature of the study. Enrolment was offered to all patients who presented to Hotel Dieu Hospital Eye clinic between January 2010 and March 2010 with either a lone diagnosis of nuclear sclerotic cataracts, or with no known history of ocular disease, a normal examination and the following optometric measurements: Best corrected visual acuity (BCVA) at near > 20/25, spherical equivalent < +/- 1.50D, and ICP scores of >14/15.
For the group with the lone diagnosis of NS cataracts, BCVA at near was determined using the logMAR scales and a near vision card held at 50cm. ICP testing was also performed at 50cm. Likewise, the group with no known ocular history were refractively blurred with +3D, +6D, +9D and +12D lenses, BCVA at near was measured, and ICP testing was performed. All patients were tested under uniform lighting conditions with a Snellen visual acuity chart. Plus lenses were placed in a trial lens frame. The order of the testing was from lowest to highest visual acuity.
The results were analysed using Microsoft Excel (Microsoft Corp,Washington). In the group with no known ocular disease, linear regression was used to determine the correlation between ICP scores and BCVA at near, but controlling for the degree of induced refractive blur. In the NS cataract group, linear regression was again used to determine the same correlation.
Results
Both groups contained 20 patients. Male to female ratio was 11:9 and 9:11 in the group with no known ocular history and the group with NS cataracts respectively. Average age was 50.2 and 65.1 respectively.
In the group with normal ocular exam, BCVA for distance ranged from 20/20 to 20/25. This corresponded to logMAR scores of 0 to 0.1 with a mean of 0.05 logMAR. As expected, BCVA at near decreased with increasing induced refractive blur. With the application of +3D, +6D, +9D and +12D lenses, mean BCVA at near was 20/25, 20/100, 20/400, and 20/1000 respectively. Additionally, ICP scores decreased with increasing induced refractive blur. Interestingly, as induced refractive blur increased, the correlation between BCVA at near and ICP decreased. The correlation coefficients between ICP scores and BCVA at near were -0.845, -0.678, -0.374, and -0.363 for BCVA at near of 20/25, 20/100, 20/400, and 20/1000 respectively. The negative value is due to the inverse relationship between logMAR values and actual visual acuity. Moreover, actual ICP scores decreased at induced refractive blur of +9D and +12D. (Figure 1 a-d).
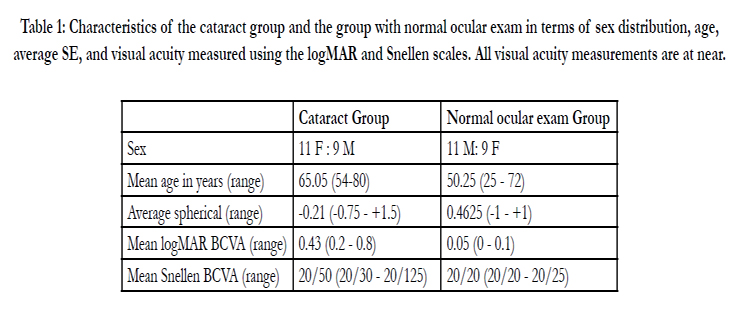

Table 1: Characteristics of the cataract group and the group with normal ocular exam in terms of sex distribution, age,average SE, and visual acuity measured using the logMAR and Snellen scales. All visual acuity measurements are at near.
.JPG)
.JPG)
.JPG)
.JPG)
.JPG)
Table 4: Intravenous antihypertensive medications.
Figure 1 a-d: Graphs of best corrected visual acuity at near Vs. Ishihara colour plate scores in the patient group with no known ocular disease. Refractive blur was induced with +3 (figure 1a), +6 (figure 1b), +9 (figure 1c), and +12 (figure 1d) lenses. The resultant mean visual acuity at near were 20/25, 20/100, 20/400, and 20/1000 respectively.
In the cataract group, BCVA at near ranged from 0.2 to 0.8 log-MAR, which roughly corresponds to Snellen values of 20/30 to 20/125. The correlation coefficient between ICP scores and BCVA at near was -0.53, p=0.016.
Discussion
The correlation coefficient between ICP and BCVA at near scores in the cataract group was -0.53, which implies that a little over half of the variability in ICP scores is explained by visual acuity. The remaining variability may still be caused by optic neuropathy[5]. This implies that ICP testing should be carried out with caution among patients with cataracts even if the best corrected atnear visual acuity is good.
This study has several limitations. Firstly, the use of induced refractive blur at 0.5 logMAR unit intervals decreases the precision of this study. Similar studies used intervals of 0.1 logMAR [6] Secondly, our nucleus sclerosis cataract group had visual acuities ranging from 0.1 logMAR to 1.7 logMAR, and analysis was performed on this group as a whole. There were not enough patients in this group to create the same four visual acuity categories as the group with normal ocular exam.
In the group with normal ocular exam, the actual ICP scores began to decline when induced refractive blur produced a mean BCVA at near of 20/400. This indicates that ICP scores are valid until BCVA at near of 20/100. Further studying is required to determine if severe vision loss due to NS cataracts effects ICP testing. If so, the subsequent step is to determine the level of vision loss at which the effect begins to manifest itself.
Acknowledgements and Disclosure
All investigators had access to the study data at all times and take responsibility for the integrity of the data and the accuracy of the data analysis. There are no financial interests or conflicts of interest to report and no external funding was received from any source. There are no additional contributors.
References
- Birch J (1997) Efficiency of the Ishihara test for identifying red-green colour deficiency. Ophthalmic. Physiol. Opt 17:403–408.
- Pacheco-Cutillas M, Edgar DF, Sahraie A (1999) Acquired colour vision defects in glaucoma – their detection and clinical significance. Br. J. Ophthalmol 83:1396–1402.
- Schneck ME, Haegerstrom-Portnoy G (1997) Color vision defect type and spatial vision in the optic neuritis treatment trial. Invest . Ophth. Vis. Sci 38:2278–2289.
- Tregear SJ, Knowles PJ, Ripley LG, Casswell AG (1997) Chromatic-contrast threshold impairment in diabetes. Eye 11:537–546.
- Almog Y, NEMET A (2010) The Correlation Between Visual Acuity and Color Vision as an Indicator of the Cause of Visual Loss. Am J Ophthalmol 149:1000–1004.
- McCulley TJ, Golnik KC, Lam BL, Feuer WJ (2006) The Effect of Decreased Visual Acuity on Clinical Color Vision Testing. Am J Ophthalmol 141:194-6.





