Dry Eye Changes after Phacoemulsification and Manual Small Incision Cataract Surgery (MSICS)
Saif MYS1*, Saif ATS2, Saif PS3, AbdElKhalek MO1, Mahran W1
1 Ophthalmology Department, Beni-Suef University, Egypt.
2 Ophthalmology Department, Fayoum University, Egypt.
3 Ophthalmology Department, Misr University for Science and Technology, Egypt.
*Corresponding Author
Mohamed Yasser Sayed Saif,
Assistant professor of Ophthalmology,
Beni Suef University, 5 sherif st,
Babel Louk sq. Cairo, 11111, Egypt.
Tel: +20 100 6699288
E-mail: ysaif@med.bsu.edu.eg
ysaif@sayedsaif.com
Received: January 17, 2016; Accepted: February 12, 2016; Published: February 15, 2016
Citation: Saif MYS et al., (2016) Dry Eye Changes after Phacoemulsification and Manual Small Incision Cataract Surgery (MSICS). Int J Ophthalmol Eye Res. 4(2), 184-191.DOI : dx.doi.org/10.19070/2332-290X-1500038
Copyright: Saif MYS© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: Evaluation of tear film stability and tear secretion after phacoemulsification and manual small incision cataract surgery (MSICS).
Design: Prospective comparative randomized clinical study.
Subject and methods: 40 Patients included in this study divided into, Group A: 20 eyes with phacoemulsification. Group B: 20 eyes with MSICS. All patients had full ophthalmic examination including Tear film break-up time (TF-BUT), schirmer test, corneal fluorescein staining and dry eye symptoms recorded pre- and post- operatively. All patients were done by the same surgeon randomly selected standard coaxial phacoemulsification or MSICS.
Results: The mean age in group A 55.8 ± 15.8 while, 60.65 ± 9.2 in group B. Most of patients in group B were females (90%) versus 45% in group A with statistically significant difference (p-value < 0.05). Grade of dry eye symptoms (DES) has significantly increased 1 week after each procedure and remained increased after 4 weeks of surgery. After 3 months, the grade of DES has decreased again and returned to near baseline data. There was no statistically significant difference between both groups regarding TF-BUT, Cornea fluorescein staining, and Schirmer test.
Conclusion: The present study has shown that MSICS is as effective as phacoemulsification with no difference between both techniques as regarding effect on tear film stability and tear secretion.
2.Introduction
3.Aim of the work
4.Subjects and Methods
4.1.Type of study
4.2.Setting
4.3.Approvals
4.4.Inclusion criteria
4.5.Exclusion criteria
4.6.The tear film break up time test
4.7.The basal schirmer 2 test
4.8.The corneal fluorescein staining
4.9.Dry eye symptoms
4.10.Postoperative examination
4.11.Statistical Methodology
5.Results
6.Discussion
7.Conclusion
8.References
Keywords
Tear Film Break-Up Time; Schirmer Test; Corneal Fluorescein Staining; Dry Eye Symptoms.
Introduction
Cataract is currently the main cause of avoidable blindness especially in the developing world accounting for about three quarters of blindness. In developed world phacoemulsification is the primary method of performing cataract surgery. However, in many developing countries involving the majority of cataract blindness in the world today, phacoemulsification is not viable due to density of cataract involved and high cost of the equipment [1].
Phacoemulsification has become the preferred method of cataract extraction over the last 15 years. The smaller incision of phacoemulsification is associated with little induced postoperative astigmatism and early stabilization of refraction [2, 3].
MSICS is a good alternative to phacoemulsification in areas where very high volume surgery with inexpensive instrumentation is required. The procedure is fast and has a low rate of complications and can be performed in the dense cataract [2, 3].
Phacoemulsification affect tear production post operatively in diabetic cataract patient, whose schirmer 1 test had decreased, causing a risk for the cornea to be damaged and dry eye symptoms [4].
Aim of the work
Evaluation of tear film stability and tear secretion after phacoemulsification compared with after manual small incision cataract surgery.
Subjects and Methods
Prospective comparative randomized clinical study.
Multicenter study at Beni-Suef University, Fayoum University and Misr University for Science and Technology.
The Beni Suef Ophthalmology council and IRB approved the study. An approval consent was signed by all patients before enrollment in the study.
Eyes with cataract of any type.
Diabetics, rheumatoid and Sjogren syndrome.
This study included 40 eyes divided into two groups.
Group A: 20 eyes with phacoemulsification.
Group B: 20 eyes with MSICS.
All patients had a full ophthalmic examination including visual acuity, slit lamp examination, fundus examination, intraocular pressure (IOP) measurement and ultrasonography if the fundus is not seen.
The ocular examinations include a tear film break up time (TFBUT) measurement, schirmer II test and corneal fluorescein staining. Dry eye symptoms were also recorded.
The tear film break up time test was performed using a commercial available fluorescein test paper that contacted with bottom conjunctiva. The subjects were instructed to blink 3 times, and then look straight forward without any blink. Tear film was observed using a blue cobalt filter under wide lighting. The interval between the last blink and the appearance of the first corneal dry spot was measured. The last procedure was repeated 3 times and the mean value was recorded. A TFBUT value less than 10 seconds is abnormal.
The basal schirmer 2 test was performed for assessment of aqueous tear production. The test involved measuring the amount of wetting of special (no.41 Whatmann) filter paper, 5 mm wide and 35 mm long. The test was performed as follows:
a – The eye was gently dried of excess tears. Topical anesthesia was applied and the excess was removed from the inferior fornix with filter paper or cotton piece.
b – The filter paper was folded 5 mm from one end and inserted at the junction of the middle and outer third of the lower eyelid.
c - The patient was asked to keep the eyes gently closed.
d – After 5 minutes the filter paper was removed and the amount of wetting from the fold measured.
The corneal fluorescein staining was performed by using test paper bar of fluorescein to contact the lower fornix of the eye. After 3 times of blinks, the subjects were asked to see straight forward without any blink. Under the wide blue cobalt light of the bimicroscope, the cornea was assessed. Staining in any part of the cornea was considered as abnormal.
Corneal staining of the area was graded:
- Grade 0: no punctuate staining.
- Grade 1: < 1/8 stained.
- Grade 2: > 1/8 to < 1/4 stained.
- Grade 3: >1/4 to 1/2 stained.
- Grade 4: Entire area stained.
Dry eye symptoms were characterized by burning, stinging, redness, sensation of a foreign body, photophobia and blurred vision and scored by the grades of 0, 0.5, 1 or 2.
- Grade 0: no dry eye symptoms.
- Grade 0.5: trace or seldom of dry eye symptoms.
- Grade 1: sometimes or mild dry eye symptoms.
- Grade 2: frequent or moderate dry eye symptoms.
All patients received pre operatively eye drops of 1% cyclopentolate and 1% tropicamide for mydriasis. Peribulbar anaesthesia was used for all patients.
A standard coaxial phacoemulsification technique was done with insertion of foldable PCIOL in the bag.
MSICS was done with insertion of PCIOL in the bag .
Post operatively, patients received topical 0.3% ofloxacin eye drops and 0.1% fluorometholone plus diclofenac sodium eye drops. Postoperatively to prevent infection and inflammation after the surgery. We didn't use strong steroid to decrease the effect of the drug on the tear secretion.
Dry eye symptoms were characterized by burning, stinging, redness, sensation of a foreign body, photophobia and blurred vision and scored by the grades of 0, 0.5, 1 or 2.
- Grade 0: no dry eye symptoms.
- Grade 0.5: trace or seldom of dry eye symptoms.
- Grade: 1: sometimes or mild dry eye symptoms.
- Grade 2: frequent or moderate dry eye symptoms.
All patients received pre operatively eye drops of 1% cyclopentolate and 1% tropicamide for mydriasis. Peribulbar anaesthesia was used for all patients.
A standard coaxial phacoemulsification technique was done with insertion of foldable PCIOL in the bag.
MSICS was done with insertion of PCIOL in the bag .
Post operatively, patients received topical 0.3% ofloxacin eye drops and 0.1% fluorometholone plus diclofenac sodium eye drops. postoperatively to prevent infection and inflammation after the surgery. We didn't use strong steroid to decrease the effect of the drug on the tear secretion.
Visit 1: At the second day of the operation.
Visit2: At the end of the first week.
Visit3: At the end of the fourth week.
Visit4: At the end of the third month.
In every visit-except the first-complete ophthalmic examination was done for every patient and dry eye tests as TF-BUT measurement, schirmer II test and corneal fluorescein staining were done. The dry eye symptoms were also recorded.
Statistical Analysis was conducted using Statistical Package for Social Science (SPSS) software, Version 16.0 in excel sheet 2007. Descriptive Analysis was used to describe different variables in terms of mean, Standard deviations, minimum, maximum and range values. This descriptive analysis was conducted to overview different variables, and test for sample normality and its representation to patient community. Statistical inference was conducted as follows:
Using T Test to compare means for dependent sample purposes, as the sample was considered as a pre and post intervention clinical trial. T test was considered statistically significant (i.e. there is a statistical difference between pre and post intervention measurements if the p value was < 0.05 as the confidence interval was assigned as 95 % for all applied tests. When p value was below 0.01 the test was considered and interpreted as highly significant. This procedure was applied to all numerical variables. In such case, a confidence interval of upper and lower limits was calculated.
Results
The aim of the present study was to evaluate tear film stability and tear secretion after phacoemulsification compared with changes of tear stability and tear secretion after manual incision cataract surgery. A total of 40 patients (40 eyes) with cataract were randomized into two groups: phacoemulsification group (Group A) included 20 patients (20 eyes) and group B (MSICS) that also included 20 patients (20 eyes).
There was no statistically significant difference between both groups regarding age with mean age 55.8 years in group A and 60.65 years in group B. Most of patients in group B were females (90%) versus 45% in group A with statistically significant difference (p-value < 0.05) as shown in table 1.
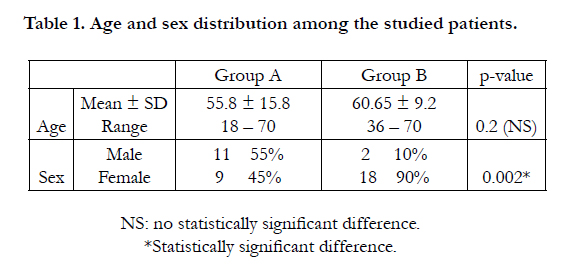

Table 1. Age and sex distribution among the studied patients.
Grade of DES has significantly increased 1 week after each procedure compared to preoperative data and remained increased after 4 weeks of surgery. After 3 months, the grade of DES has decreased again and returned to near baseline data. There was no statistically significant difference between both groups during any time point. Both phacoemulsification and MSICS patients had more severe DES on the first week postoperatively and slightly decreased after 4 weeks. Thereafter, the grades of DES returned to preoperative levels after 3 months as shown in table 2.
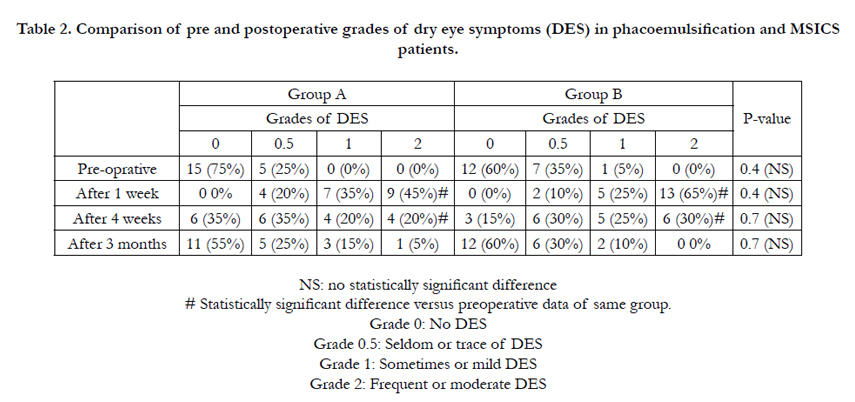
Table 2. Comparison of pre and postoperative grades of dry eye symptoms (DES) in phacoemulsification and MSICS patients.
There was no statistically significant difference between both groups regarding all symptoms at different time points except for presence of secretions 3 months after the operation as it was significantly higher among group A patients (phacoemulsification group). The pattern of change in prevalence of different symptoms in follow up period is almost the same in both groups. Heavy eyelid was absent in both groups prior to the operation then increased significantly up to 80 and 90% one week after surgery in group A and B respectively then decreased significantly till 3 months post-operative. Similar pattern of change was noted for foreign body sensation, redness, stinging and feeling of dryness as shown in table 3.
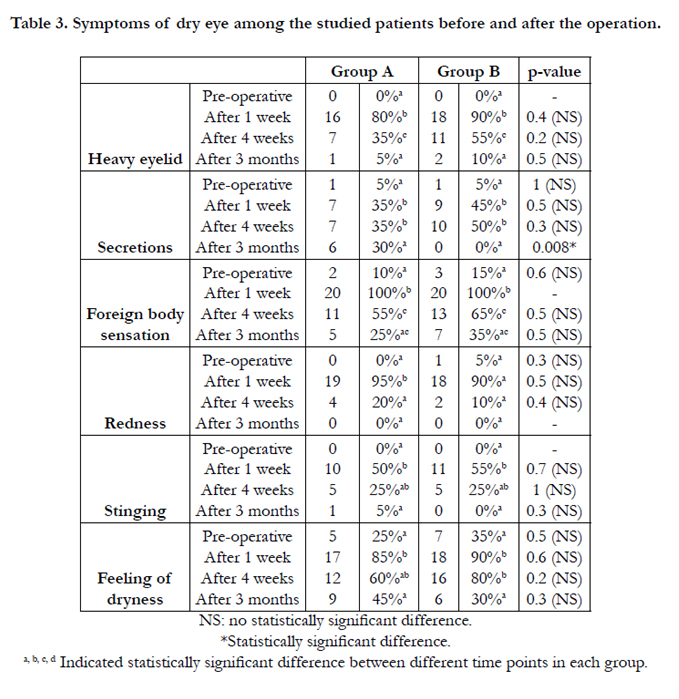
Table 3. Symptoms of dry eye among the studied patients before and after the operation.
There was no statistically significant difference between both groups regarding TF-BUT whether pre-operative or during the whole follow up period. Also there was no significant change over time among patients of each group. As shown in table 4.
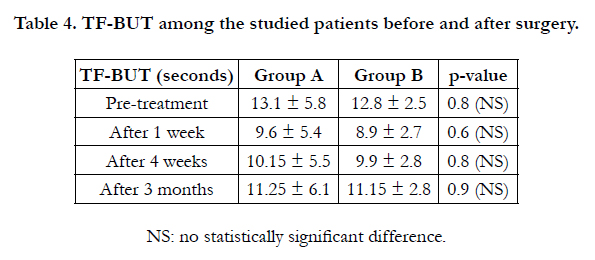
Table 4. TF-BUT among the studied patients before and after surgery.
No significant difference between the two groups regarding to TF-BUT during the whole follow up period. The TF-BUT was decreased one week after surgery and increased after 4 weeks to become near pre-operative data after 3 months as shown in figure 1.
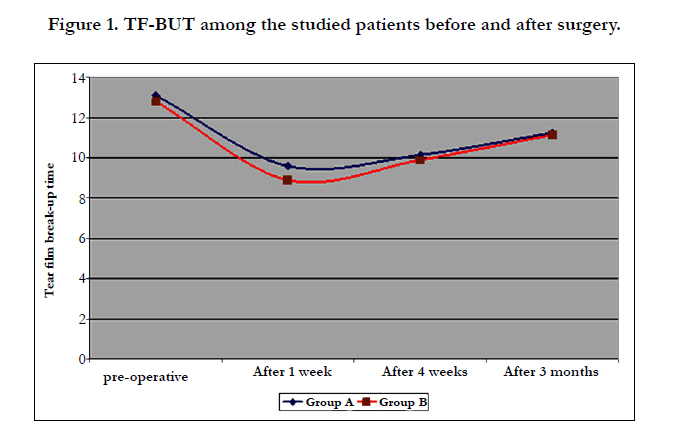
Figure 1. TF-BUT among the studied patients before and after surgery.
There was no statistically significant difference between both groups regarding corneal fluorescein staining grade whether pre-operative or during the whole follow up period. After 1 week of surgery most of eyes were stained grade 2 (55% and 45% in group A and B respectively) with statistically significant difference versus pre operative findings. After 3 months, there was no significant difference compared to pre-operative findings as shown in table 5.
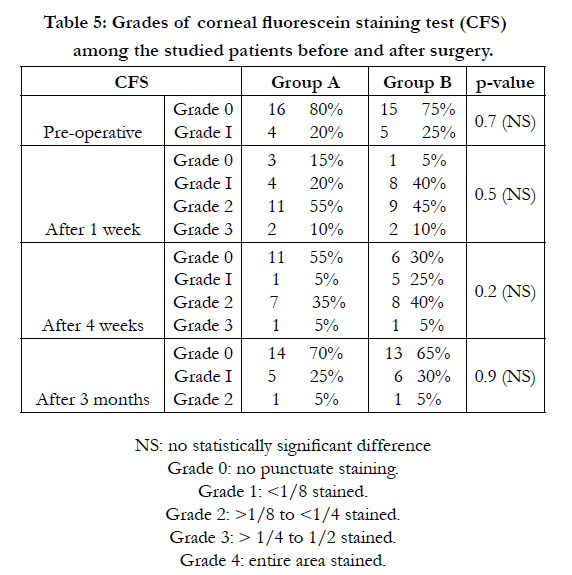
Table 5: Grades of corneal fluorescein staining test (CFS) among the studied patients before and after surgery.
There was no statistically significant difference between both groups regarding corneal fluorescein staining grade whether pre-operative or during the whole follow up period. With phacoemulsification, there was significant increase in number of eyes with positive corneal staining only after 1 week of surgery (from 20% to 85%) and returned to preoperative values after 4 weeks. However, with MSICS in group B there was significant increase in number of eyes with positive corneal staining that remained significantly increased even after 4 weeks of surgery but with no statistically significant difference versus group A as shown in table 6.
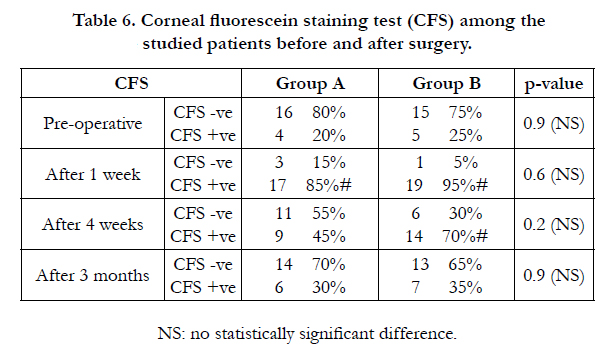
Table 6. Corneal fluorescein staining test (CFS) among the studied patients before and after surgery.
There was no statistically significant difference between both groups regarding Schirmer test whether pre-treatment or during the whole follow up period. With phacoemulsification there was significant decrease that was noted after 1 week and continued till end of follow up period compare to pre-operative period. With manual small incision cataract surgery, there was also significant decrease noted after 1 week of surgery but with end of follow up the test results were insignificantly different compared to preoperative findings shown in table 7.
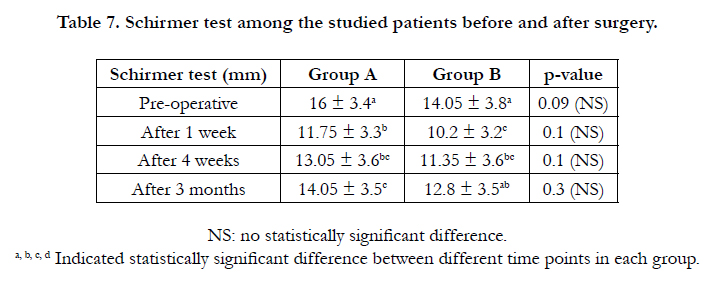
Table 7. Schirmer test among the studied patients before and after surgery.
By reviewing the previous tables and statistical results, we can easily conclude that:
Dry eye symptoms (burning sensation, stinging, redness, sensation of foreign body, photophobia, and blurred vision) were increased at one week postoperatively in the two groups, and started to improved after one month postoperatively and became nearly as preoperative after 3months in the two groups.
The TF-BUT test was decreased one week after surgery and increased after 4 weeks to become near pre-operative data after 3 months. No significant difference between the two groups regarding to TF-BUT test during the whole follow up period.
After 1 week of surgery most of eyes were stained grade 2 (55% and 45% in group A and B respectively) with statistically significant difference versus pre operative findings. After 3 months, there was no significant difference compared to pre-operative findings. There was no statistically significant difference between both groups regarding corneal fluorescein staining grades whether preoperative or during the whole follow up period.
There was no statistically significant difference between both groups regarding Schirmer test whether pre-treatment or during the whole follow up period. With phacoemulsification there was significant decrease that was noted after 1 week and continued till end of follow up period compare to pre-operative period. With manual small incision cataract surgery, there was also significant decrease noted after 1 week of surgery but with end of follow up the test results were insignificantly different compared to preoperative findings.
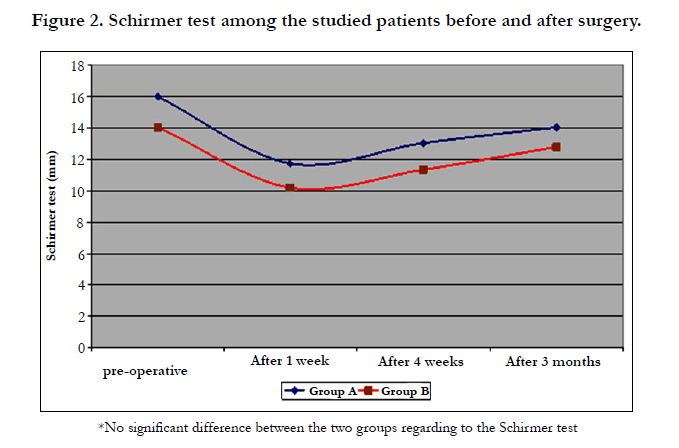
Figure 2. Schirmer test among the studied patients before and after surgery.
Discussion
To the best of our knowledge, few studies have been published comparing both techniques regarding their effect on tear film stability and tear secretion. Most of published studies were concerned of visual outcome after both surgeries. The few available studied concerned with the current outcome (tear film stability and tear film secretion) were conducted aftercertain patients' subgroups as diabetic patients or patients with preoperative dry eye.
When publication was sought for a British Medical Research Council (MRC) trial comparing phacoemulsification to extracapsular cataract extraction, peer reviewers initially recommended rejection because they regarded the case already made that phacoemulsification was safer and more effective. But it was, in fact, an important trial (and the study was eventually published) because it showed that despite the additional costs associated with the technology, phacoemulsification resulted in longer-term savings as a result of more rapid rehabilitation and fewer postoperative visits [5].
But this was only relevant to affluent health systems. For poorer countries, the capital and consumable costs of phacoemulsification remain a major issue. Cost is one of the most important barriers to cataract surgery, and it is in the poorer parts of the world where the huge backlog of avoidable cataract blindness exists. Pioneers of cataract techniques in India and Nepal soon found a way of reducing the incision size and eliminating the need for sutures in manual or nonmechanized techniques. This constituted the specific disadvantage of the traditional extracapsular technique: the need to have the sutures removed at three months, and the degree of postoperative astigmatism. Variations of the smallincision manual technique have rapidly developed, and last year, the first trials comparing phacoemulsification with MSICS and MSICS with extracapsular surgery were published [6-8]. These trials assessed visual outcome, vision-related quality of life, and cost. MSICS was found to be almost as good as phacoemulsification.
As regarding symptoms of dry eye, the present study has shown that there was significant increase in symptoms of dry eye 1 week after postoperative in both groups (phacoemulsification and MSICS) and returning for baseline preoperative prevalence after 3 months (120 day). This was applied for all symptoms including heavy eyelid, secretions, foreign body sensation, eye redness, stinging and feeling of dryness. No difference was noted between both groups.
Grade of dry eye symptoms (DES) has significantly increased 1 week after each procedure compared to preoperative data and remained increased after 4 weeks of surgery. After 3 months, the grade of DES has decreased again and returned to near baseline data. There was no statistically significant difference between both groups during any time point.
In the study of Liu and colleagues in 2008 [4] , grade of DES has increased for 7 days after phacoemulsification. The persistence of high grades of DES was for longer duration in the present study.
We have used three objective tests for assessment of tear film changes and tear film secretions following each of phacoemulsification and manual small incision cataract surgery. These tests are tear film break up time, cornea fluorescein staining test and schirmer test.
As concerning tear film break up time, the present study didn't report any significant change following each of surgical procedures whether one week or after 3 months and also there was no significant difference between both groups.
Unlike the current study, Liu et al., (2008) [4] have shown that phacoemulsification resulted in significant reduction of tear film break up only for time 1 day postoperatively.
Corneal fluorescein staining test has shown different results. Preoperative most of the studied patients (80% and 75% in group A and group B respectively) have shown no staining (grade 0). Only after 1 weeks of surgery the condition has turned out that most of patients has > 1/8 - < 1/4 corneal staining (grade II) and by this time 4 patients have even shown entire area staining (grade IV) (2 patients in each group). However, after three months most of patients has returned to preoperative state and showed no corneal staining.
There was no statistically significant difference between both groups regarding Cornea fluorescein staining grade whether pre-treatment or during the whole follow up period. With phacoemulsification, there was significant increase in number of eyes with positive corneal staining only after 1 week of surgery (from 20% to 85%) and returned to preoperative values after 4 weeks. However, with MSICS in group B there was significant increase in number of eyes with positive corneal staining that remained significantly increased even after 4 weeks of surgery but with no statistically significant difference versus group A.
Similar to the present study, Liu and colleagues (2008) [4] have shown that postoperatively, there is significant increase in number of patients showing corneal staining after phacoemulsification then it eventually reduced. However, in their study this increase was detected only 1 day after phacoemulsification while in the present study the corneal staining started to decrease after one month but still present at the third month.
As regarding schirmer test, in both groups it has been reduced 1 week following surgery and returned to baseline value after three months in group B (MSICS) while in group A (phacoemulsification) even after 3 months, it is still significantly lower than preoperative values. Liu et al., (2008) [4] have shown different results as it has reported that Schirmer test has increased significantly after phacoemulsification.
Prior studies have examined the effect of cataract surgery on tear film parameters and reported short-term disruptions in tear function. Consistently Ram et al. (2002) [9] and Li et al , (2007) [10] in 23 and 37 post cataract surgery patients respectively demonstrated decreased Schirmer scores and at various time points up to 2 months postoperative compared to preoperative values as same as the present study. As we have found that Schirmer test scores decreased significantly till 4 weeks postoperative.
However unlike the present study, Ram et al., (2002) [9] Li et al , (2007) [10] have shown significant decrease in tear break-up time (TBUT) while the present study have shown no significant change in tear break-up time (TBUT) till 3 months postoperative.
Also Venincasa and colleagues (2013) [11] have conducted a study to evaluate the differences in tear film parameters more than 3 months postsurgery in eyes with cataract surgery (surgical eyes) versus eyes without cataract surgery (nonsurgical eyes). They have found that after three months of surgery there was no statistically significant difference between surgical and nonsurgical eyes regarding corneal staining; tear break-up time and Schirmer’s test [11]. Their findings supported the current evidence as after three months we have found that all evaluated parameters have returned to preoperative values.
Kasetsuwan et al [12] concluded that the severity of dry eye peaked seven days post-phacoemulsification and was measured by OSDI questionnaire and three clinical tests. Within thirty days and 3 months post-surgery, both the symptoms and signs showed rapid and gradual improvements, respectively. However, dry eye post-phacoemulsification was not significantly associated with sex and systemic hypertension [12].
Another study that was conducted at 2010 [13] has compared phacoemulsification versus MSICS but regarding surgical complications, operative time, uncorrected (UDVA) and corrected (CDVA) distance visual acuities, and surgically induced astigmatism and hasn't addressed the issue of tear film stability and tear secretion. They have found that both techniques achieved excellent visual outcomes with low complication rates. Because SICS is significantly faster, less expensive, and less technology dependent than phacoemulsification, it may be a more appropriate technique in eyes with mature cataract in the developing world [13].
A problem with trials in which the same surgeon is randomized to both techniques under investigation is that the surgeons involved may not be equally skilled in both techniques. It makes it possible for experts who disagree with a trial’s findings to implicate the surgical skill of the trial surgeons. It is not the technique that is at fault, but the fact that the surgeons involved may have perfected one technique over another.
The cost of the surgery should have been questioned also, and it is important issue especially in developing countries like Egypt [14-18].
Trials of equivalence are also a problem. To confidently assert that one treatment is as good as another makes enormous demands on sample size. To detect small differences, a huge sample size is required. Another limitation of the present study was small sample size (20 eyes in each group). Also another limitation is that we had followed patients for short term (3 months) and didn't evaluate long term effects.
Conclusion
The present study has shown that MSICS is as effective as phacoemulsification with no difference between both techniques as regarding effect on tear film stability and tear secretion.
Phacoemulsification and SICS reduced the tear secretion in the studied patients so, it is necessary to use artificial tear preparations for managing corneal damage and dry eye symptoms.
References
- Garg A, Fry LL, Tabin G (2004) Clinical practice in small incision cataract surgery: Phaco Manual. (1st edtn), Jaypee Brothers Medical Publishers, India.
- Kanski JJ, Bowling B (2011) Clinical ophthalmology: A systematic approach. (7th edtn). Saunders/ Elsevier, New York.
- Kanski JJ, Bowling B (2011) Clinical ophthalmology: A systematic approach. Dry eye disorders (7th edtn), Elsevier/Saunders, New York. 4: 122.
- Liu X, Gu YS, Xu YS (2008) Changes of tear film and tear secretion after phacoemulsification in diabetic patients. J Zhejiang Univ Sci B 9(4): 324- 328.
- Minassian D, Rosen P, Dart J, Reidy A, Desai P, et al. (2001) Extracapsular cataract extraction compared with small incision surgery by phacoemulsification: a randomised trial. Br J Ophthalmol 85(7): 822-829.
- Gogate PM, Deshpande M, Wormald RP, Deshpande R, Kulkarni SR (2003) Extracapsular cataract surgery compared with manual small incision cataract surgery in community eye care setting in western India: a randomised controlled trial. Br J Ophthalmol 87(6): 667-672.
- Gogate PM, Deshpande M, Wormald RP (2003) Is manual small incision cataract surgery affordable in the developing countries? A cost comparison with extracapsular cataract extraction. Br J Ophthalmol 87(7): 843-846.
- Gogate PM, Kulkarni SR, Krishnaiah S, Deshpande RD, Joshi SA, et al. (2005) Safety and efficacy of phacoemulsification compared with manual small incision cataract surgery by a randomized controlled clinical trial: sixweek results. Ophthalmology 112(5): 869-874.
- Ram J, Gupta A, Brar GS, Kaushik S, Gupta A (2002) Outcomes of phacoemulsification in patients with dry eye. J Cataract Refract Surg 28(8): 1386- 1389.
- Li XM, Hu L, Hu J, Wang W (2007) Investigation of dry eye disease and analysis of the pathogenic factors in patients after cataract surgery. Cornea 26(9 Suppl 1): S16-S20.
- Venincasa VD, Galor A, Feuer W, Lee DJ, Florez H, et al. (2013) Longterm effects of cataract surgery on tear film parameters. The Scientific World Journal 2013: 1-4.
- Kasetsuwan N, Satitpitakul V, Changul T, Jariyakosol S (2013) Incidence and Pattern of Dry Eye after Cataract Surgery. PLoS One 8(11): e78657.
- Venkatesh R, Tan CS, Sengupta S, Ravindran RD, Krishnan KT, et al. (2010) Phacoemulsification versus manual small-incision cataract surgery for white cataract. J Cataract Refract Surg 36(11): 1849-1854.
- Amer SAK, Saif MYS, Abd El-Khalek MO, Tawfik A (2012) Prevalence of Dry Eye Syndrome in Beni-Suef Population. Cataract Cornea 18: 2-13.
- Abueleinen KG, El-Mekawey H, Saif MYS, Khafagy A, Rizk HI, et al. (2011) Sociodemographic factors responsible for blindness in diabetic Egyptian patients. Clin Ophthalmol 5: 1593-1598.
- Saif MYS, Saif ATS, Amer SK, Abueleinen KG (2012) Prevalence of Ophthalmic Disease in the Egyptian Oasis. Tanta Medical Sciences Journal 7(3): 21-28.
- Elsaftawy HS, Ahmed MH, Saif MY, Mousa R (2015) Sequential Intracorneal Ring Segment Implantation and Corneal Transepithelial Collagen Cross-Linking in Keratoconus. Cornea 34(11): 1420-1426.
- Said DG, Elalfy MS, Gatzioufas Z, El-Zakzouk ES, Hassan MA, et al. (2014) Collagen cross-linking with photoactivated riboflavin (PACK-CXL) for the treatment of advanced infectious keratitis with corneal melting. Ophthalmology 121(7): 1377-1382.





