The Relation between Scapular Dyskinesis and the Upper Quarter Y-Balance Test
Amasay T1*, Hall GA II2, Shapiro S1, Ludwig K1
1 Department of Sport & Exercise Sciences, School of Human Performance & Leisure Sciences, Barry Univesity, Miami Shores, FL USA.
2 Athletic Department, Eckerd College, St. Petersburg, FL, USA.
*Corresponding Author
Amasay Tal,
Department of Sport & Exercise Sciences,
School of Human Performance & Leisure Sciences, Barry Univesity,
Miami Shores, FL, USA.
E-mail: tamasay@barry.edu
Received: February 29, 2016; Accepted: March 16, 2016; Published: March 30, 2016
Citation: Amasay T, Hall GA II, Sue S, Kathy L (2016) The Relation between Scapular Dyskinesis and the Upper Quarter Y-Balance Test. Int J Anat Appl Physiol. 2(2), 20-25. doi: dx.doi.org/10.19070/2572-7451-160003
Copyright: Amasay T© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The shoulder is a complex mechanical system. Alterations in the position and/or orientation of its joints may interfere with optimal shoulder coordination. Scapular dyskinesis (SDK) is defined as mal-positioning or mal-movement of the scapula along the thoracic wall. It is not well established the role of scapular dyskinesis as the cause or the effect of shoulder pathologies. The Upper-Quarter Y-Balance test (UQYBT) has been suggested as a return-to-play tool for athletes with upper extremity injuries. The objective of this study was to quantify the relation between the UQYBT and SDK. Six males and five females participated in the study, age 18-30 years old. All participants’ shoulders were evaluated by a certified athletic trainer using Kibler Scapular Dyskinesis Test (SDT) as having dyskinesis or not. Each participant performed three of the SDT and three of the UQYBT. The outcomes of the UQYBT were the highest score for each direction Superior- Lateral Reach (SLR), Inferior-Lateral Reach (ILR), and Medial Reach (MR) and the Composite score. An independent t-test with unequal variances was performed to determine statistical differences between normal and SDK shoulders during the UQYBT. Results indicate significant differences between the normal and SDK shoulders in the Composite score (p=.048). No significance was found during the ILR, SLR, and MR. In conclusions, when the SDK shoulder was stabilizing during the UQYBT higher scores were seen in every direction compared to the normal shoulder. These suggest that SDK may affect the scores of UQYBT.
2.Introduction
3.Materials and Methods
3.1.Participants
3.2.Instrumentation
3.3.Procedures
3.4.Data Analysis
4.Results
5.Discussion
6.References
KeyWords
Shoulder Testing; Biomechanics; Scapular Dyskinesis; Functional Testing; Balance.
Introduction
The shoulder complex is a unique mechanical system in the human body consisting of three bones: the scapula, humerus and clavicle. These bones interact with each other through three joints (sternoclavicular, acromioclavicular, glenohumeral) and one articulation (scapulothoracic). The interaction between these bones produces smooth coordinated movements of the shoulder, such as reaching. Alterations in the position and/or orientation of any of these joints and articulation may interfere with optimal shoulder coordination. Abnormal shoulder kinematics has been found to be associated with musculoskeletal disorders such as rotator cuff impingement syndrome [1-3], unstable shoulder hypermobility [4], and frozen shoulder [5, 6].
Scapular dyskinesis is defined as mal-positioning or malmovement of the scapula along the thoracic wall during static glenohumeral position or dynamic movement. It is identified with increased protraction of the inferior angle and medial border of the scapula, and scapular dysrhythmia and or asymmetry bilaterally [7, 8]. It is believed that multiple factors may cause scapular dyskinesis such as bony, neurological and/or muscular sources. Some examples are clavicle fracture, long thoracic nerve palsy, and serratus anterior activation [8]. It is not well established the role of scapular dyskinesis as the cause or the effect of shoulder pathologies. On its own, scapular dyskinesis is neither an injury nor musculoskeletal disorder [8]. With current research on shoulder pathologies, there is a link between scapular dyskinesis and shoulder conditions such as rotator cuff pathologies, glenohumeral instability, acromioclavicular joint injuries, and adhesive capsulitis [7, 9, 10].
Currently, there are several tests to determine scapular dyskinesis, such as the Lateral Scapular Slide Test and the Scapular Dyskinesis Test (SDT). Reliability and validity of the Lateral Scapular Slide Test was relatively low [11]. On the other hand, the SDT, the most common visual test used, was found to have moderate reliability (k value, 0.4 - 0.6) [12, 13] as well as the validity [14]. The SDT was introduced by Ben Kibler (2002). The test incorporates glenohumeral flexion and abduction with resistance (3 lb or 5 lb depends on body weight) to determine the presence of scapular dyskinesis. Clinicians visually observe the movement of the scapula throughout the different range of motions and subjectively classify scapular motion patterns as having dyskinesis or not [12].
The Upper Quarter Y-Balance Test (UQYBT) was developed as a clinical upper extremity functional test. The UQYBT implements three dynamic movements while the participant is in the push-up position. During the test, the participant needs to stabilize his body in the push-up position while reaching in three different directions medial, superior-lateral, and inferior-lateral. The UQYBT can be used to compare between limb-to-limb movement limitations and asymmetries. There is a limited amount of research on the UQYBT. Westrick et al. (2012) examined the reliability and the effects of arm dominance on the UQYBT results. The test retest reliability proved excellent with an (ICC > 0.9) however, no significant difference was observed in performance score between dominant and non-dominant arms [15]. A different study by Gorman et al. (2012) demonstrated similar findings as Westrick et al. (2012) with no significant differences between dominant and non-dominant arms and reported good to high test re-test reliability (ICC > 0.8) and excellent inter-rater reliability (ICC = 1). Gorman et al. (2012) also examined gender differences during the UQYBT. No significant difference was found when comparing scores with respect to arm length [16].
The Upper-Quarter Y-Balance test has been suggested as a returnto- play tool for athletes with upper extremity injuries. However, to the best of the authors’ knowledge there are no known studies that have investigated the influence of scapular dyskinesis on UQYBT scores. The purpose of this study is to determine a relation between the UQYBT and the Scapular Dyskinesis Test. We hypothesized that a supporting arm with scapular dyskinesis would present a lower score than a supporting arm without dyskinesis on the UQYBT.
Materials and Methods
Eleven students from Barry University participated in this study, six males and five female, aged 18-30 years old. Exclusion criteria were shoulder surgery within the past year, acute or chronic subluxations/dislocations of either shoulder, or acute ligament injuries to their ulnar or elbow lateral collateral ligaments. The inclusion criteria included the ability to perform a 10 minutes warm-up on an upper extremity ergometer, lift 3 lb or 5 lb dumbbell weights in glenohumeral abduction and flexion, and perform at least five push-ups with correct form. This study was approved by the University’s IRB Committee.
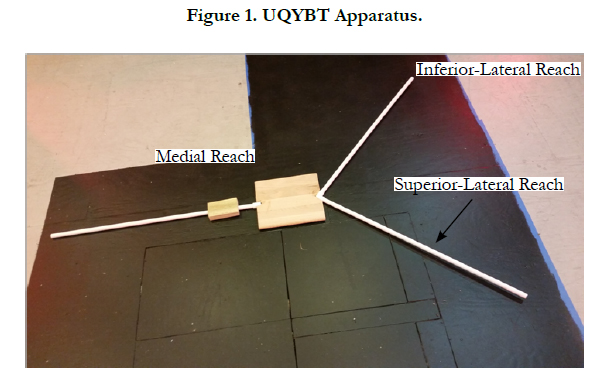
The UQYBT apparatus was designed based on the specifications of previous studies [16]. PVC pipes were connected to a wood block in the medial, inferior-lateral, and superior-lateral reach directions. Each pipe was 90 cm in length and was marked in 0.5 cm increments (Figure 1). The SDT was performed using a 3 lb or 5 lb dumbbell weights depending on the participant’s body weight.
Upon arrival to the Motion Analysis Center (MAC) Lab the participants were instruct to perform 10 minutes of warmup on the upper extremity ergometer. Once the participants finished the warm-up, they were instructed on the correct way to perform the SDT and the UQYBT. Based off previous literature those who weighed less than 150 lb used a 3 lb weight during the SDT and those who weighed 150 lb or more performed the SDT with a 5 lb [13, 14]. Participants performing the SDT stood feet shoulder width apart for both flexion and abduction. When performing shoulder flexion, their forearms were in neutral with thumbs pointing up. During abduction, their palms were facing down toward the floor. Both shoulder flexion and shoulder abduction were performed three times. Participants elevated and lowered their arms to a two-second count during both tests conditions. The participants were to pause for one second once they reached 90 degrees of either flexion or abduction before returning to the starting position. A rest interval of two minutes was taken between each trial to eliminate the affect of fatigue. Scapular dyskinesis was determined based on prominence of the inferior angle, medial border, early elevation of the acromion, or asymmetry of the scapulae during the lowering of the arms by a certified Athletic Trainer.
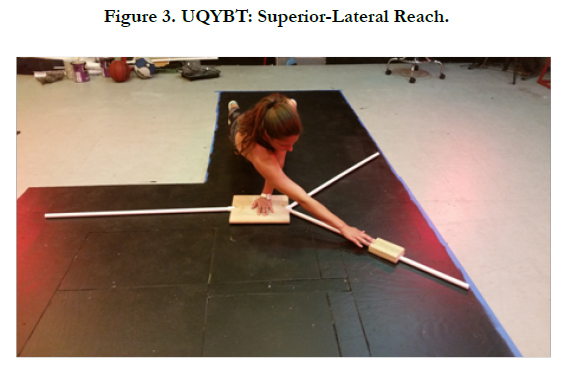
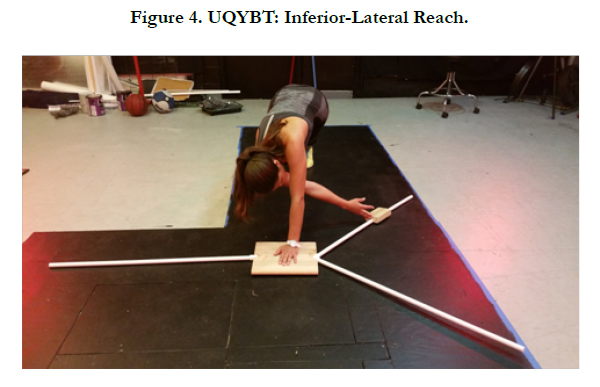
After performing the SDT, each participant performed three reaches in each of the three directions (medial, inferior-lateral, and superior-lateral) during the UQYBT (Figures 2-4). When performing the UQYBT participants were instructed to get in a push-up position with their feet shoulder width apart. The arm being tested would be supporting the body weight on the stationary plate, while the other arm moved the block. The reach distance was measured based on the final block position. The participant’s toe location was marked with tape to ensure that their feet remained in the same position throughout all testing trials. Participants were asked to keep their feet in these positions throughout each reaching trial. The medial reach required the individual to push the block with their arm straight to their side and fingertips at the edge of the block (Figure 2). The superiorlateral reach involved crossing over the stabilizing arm (Figure 3), whereas the inferior-lateral reach requires the individual to cross underneath the stabilizing arm to push the block (Figure 4). A rest period of one minute between each trial was given to eliminate the effect of fatigue. Three trials were performed in one direction before moving to next direction. If participant knees touched the ground, their body collapsed to the floor, failed to return to the starting position after moving the block, or the individual shoved the block without maintaining contact, he or she would repeat the trial. Upper extremity length was measure on the right side for each participant, from C7 to the tip of the middle finger, with the shoulder maintained at 90° of abduction.

Statistical analysis was performed on the data using SPSS version 21 (IBM Corp. Armonk, NY). Test-retest reliability, using intraclass correlation (ICC), was performed on the scores of each of the three different reaches. The highest score for each type of reach in the UQYBT was indentified for further analysis. In addition, the composite score was calculated for each group. The composite score is the average of the three different reaches. These scores were then normalized to the participant’s arm length. The means of the normalized scores were further analyzed using an independent t-test, assuming unequal variances, to identify significant differences in scores between normal shoulders and scapular dyskinesis shoulders (α=.05).
Results
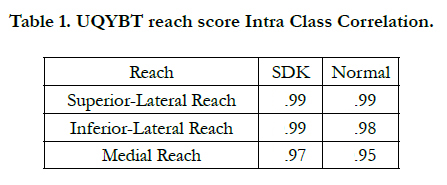
High reliability, ICC (3,1)>.95 was observed in every reach direction using the ICC (3,1) in the UQYBT for both normal (n=10) and scapular dyskinetic (SDK) (n = 12) groups (Table 1).

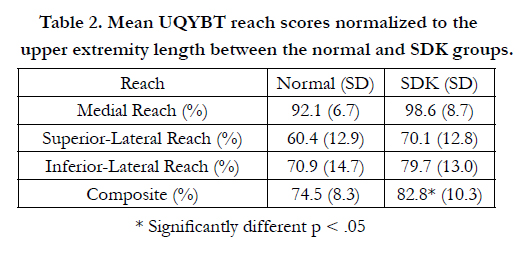
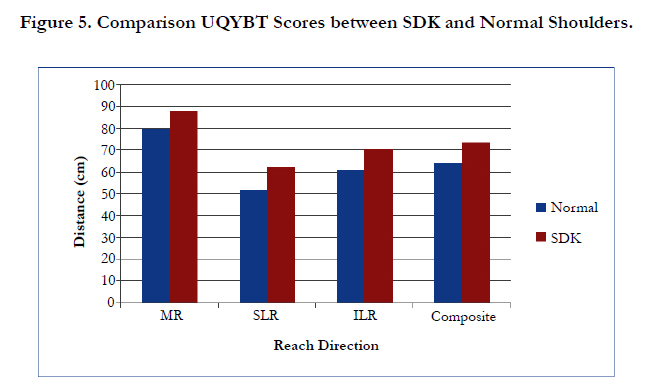
To identify differences between the two groups the highest scoring trials were used for each participant in each direction (Figure 5). Each reach score was then normalized to participant’s arm length for further analysis. The independent t-test with unequal variances identified significant differences in the Composite score (p-value = .048), where the SDK group had higher scores, on average, than the normal group. Although no significance differences were observed for the MR (p-value = .062) and SLR (p-value = .093) and ILR (p-value = .159), on average, the SDK group had the higher scores in all three directions (Table 2 and Figure 5).
Discussion
The Upper-Quarter Y-Balance test (UQYBT) has been suggested as a return-to-play tool for athletes with upper extremity injuries. In addition, difference in scores between sides or between pre and post testing, can indicate higher susceptibility for upper extremity injuries. The purpose of this study was to investigate the influence of scapular dyskinetic shoulders on the scores of the Upper Quarter Y-Balance Test (UQYBT). The assumption was that SDK shoulders would demonstrate lower scores during UQYBT in all directions. However, this study found that SDK shoulders had higher scores than normal shoulders, of which the Composite score was significantly different. Although not significant, on average MR, SLR, and ILR demonstrated higher scores in SDK shoulders too. It may be concluded that scapular dyskinesis can have an effect on the scores when stabilizing the body during the UQYBT, as well as when reaching.
An SDK shoulder is not necessarily a weak shoulder. In the case of UQYBT, the SDK shoulder was able to stabilize the body while the normal shoulder performed the reach. On the contrary, when the normal shoulder was stabilizing the SDK shoulder had a reduced mobility, which contributed to the lower reach score. On average, the SDK group scores were higher than the normal group by about 10 cm, in every direction, although only Composite score was significantly different. These observed differences might be related to the motions required the scapula to externally rotate around the thoracic wall, as well as upwardly rotate during the UQYBT. Previous studies have associated scapular dyskinesis with decreased in upward rotation, external rotation, and increased posterior tilting [8, 14]. This may explain the lower results while the SDK shoulder is reaching. In addition, a lack of mobility of the SDK shoulder while stabilizing may have been compensated by excessive trunk rotation, which we did not measure in the current study.
Comparing our study results to the other two studies measuring scores in the UQYBT our reach scores were in some cases lower than the results of the other studies, however the patterns were the same. On average, the participants achieved the highest scores during the MR, followed by the ILR, and the lowest scores during the SLR in both groups the SDK and normal shoulders. These differences can be attributed to the difference in study-pooled population. Our study had participants with scapular dyskinesis, whereas Gorman et al. (2012) had a large healthy and physically active population, and the population that was studied by Westrick et al. (2012) was from USA Military Academy of West Point [15, 16]. A more active population with no identified shoulder pathology may score higher on the UQYBT.
The UQYBT proved to have very high reliability in measuring normal and SDK groups during all reach directions, ICC (3,1) = .95 - .99. These results were similar to the ones observed by Gorman et al. (2012) and Westrick et al. (2012), ICC ranging from .80 to .99 [15, 16]. Gorman et al. (2012) indicated that the highest reliability were in the SLR (ICC = .920 - .990), and the lowest in the ILR (ICC = .800 - .960) [16]. Our study has found high reliability for all reach directions between trials using one rater. These findings might indicate that the UQYBT could be an excellent tool to compare between two sets of data collected in different times. For example, data collected pre and post season could be used to identify positive or negative changes in scores for the dominant and non-dominant arms to evaluate the quality of specific training program. On the other hand, UQYBT score pre and post injury could be used as another tool to assist in determining athlete return to play.
The UQYBT has been recommended as a measure of dynamic stability between limbs. It has been suggested that the nondominant shoulder can be used as a baseline measure when testing an injured extremity. Therefore, insinuating that the stabilizing shoulder with the higher distance reached is healthier shoulder. However, our study found that if the client has an SDK, it might influence the validity of the test. Dyskinesis does not necessarily mean that there is an injury; however, mal-movement of the scapula may cause the moving arm during the UQYBT to achieve lower scores compared to the normal shoulder. This information is critical for clinicians who administer this test, because if an individual has scapular dyskinesis there may be false findings during the UQYBT based on the assumption that the SDK shoulder would be associated with higher score reach when stabilizing. Clinicians should perform the SDT on their patients before implementing the UQYBT. This knowledge can allow the healthcare professional to incorporate rehabilitation or strengthening programs for the individual to the correct shoulder in order to prevent an injury from occurring.
References
- Adejuwon SA, Salawu OT, Eke CC, Femi-Akinlosotu W, Odaibo AB (2011) A craniometric study of adult humans skulls from Southwestern Nigeria. Asian Journal of Medical Sciences 3(1): 23-25.
- Ahmed AA, Mohammed HA, Hassan MA (2011) Sex determination from cranial measurements in recent northern Sudanese. Khartoum Medical Journal 4(1): 539-547.
- Ales Hrdlicka (1947) Hrdlicka's Practical Anthropometry. Wistar Institute of Anatomy and Biology, Philadelphia.109-197.
- Alex FR, Steven B, Timothy GL (1996) Human Body Composition. (4th edtn), Human Kinetics Publishers. 167-172.
- Cassidy PJ (1913) “Megaseme” Webster dictionary. answers.com (homepage on the internet),
Retrieved from http://www.answers.com/topic/megaseme - Dave MR, Gupta S, Vyas KK, Joshi HG (2013) A Study of Palatal Indices and Bony Prominences and Grooves in the Hard Palate of Adult Human Skulls. NJIRM 4(1): 7-11.
- Deshmukh AG, Devershi DB (2006) Comparison of Cranial Sex Determination by Univariate and Multivariate Analysis. J Anat Soc India 55(2): 48-51.
- Gopinathan K, Dhall U, Chhabra S (1998) Sutural bones in North Indian population. J Anat Soc India 47(2): 91-96.
- Ebeye OA, Otikpo O (2013) Orbital index in Urhobos of Nigeria. IOSR J Dental Med Sci 8(2): 51-53.
- Chaturvedi RP, Harneja NK (1963) A cephalometric study of human skulls. Journal of Anatomical Society of India 12: 93-96.
- Kranioti EF, Işcan MY, Michalodimitrakis M (2008) Craniometric analysis of the modern Cretan population. Forensic Sci Int 180(2-3): 110.e1–110.e5.
- Farkas LG, Munro IR (1987) Anthropometric facial proportions in medicine. Charles C Thomas Publisher, USA.
- Gosavi S (2014) A study of orbital morphometry in Indian dry skulls. Asian Journal of Biomedical and Pharmaceutical Sciences 4(29): 23-25.
- Kaur J, Yadav S, Singh Z (2012) Orbital dimensions - A direct measurement study using dry skulls. J Acad Indus Res 1(6): 293-295.
- Jaysingh P, Arora AK, Gupta CD, Dua S, Pandey DN (1979) Craniometric study of skulls of Uttar Pradesh. J Anat Soc India 28(3): 127-131.
- Kajanoja P (1966) Sex determination of Finnish crania by discriminant function analysis. Am J Phys Anthropol 24(1): 29-33.
- Kasai K, Richards LC, Brown T (1993) Comparative study of craniofacial morphology in Japanese and Australian aboriginal populations. Hum Biol 65(5): 821-834.
- Klepinger LL (2006) Fundamentals of Forensic Anthropology. John Wiley & Sons, USA.
- Krishan K (2008) Estimation of stature from cephalo-facial anthropometry in north Indian population. Forensic Sci Int 181(1-3): 52e1-52e6.
- Krogman WM, Iscan MY (1986) The Human Skeleton in Forensic Medicine. Charles C Thomas Publisher, USA.
- Lobo SW, Chandrashekar TS, Kumar S (2005) Cephalic Index of Gurung Community of Nepal - an Anthropometric study. Kathmandu Univ Med J 3(3): 263- 265.
- Martin R, Saller K (1957) Lehrbuch der Anthropologie. Gustav Fischer Verlag, Stuttgart.
- Steyn M, Işcan MY (1998) Sexual dimorphism in the crania and mandibles of South Africa whites. Forensic Sci Int 98(1-2): 9-16.
- Mcgraw Hill dictionary of scientific and technical terms “mesoconch” Mcgraw hill company Inc, answers. Com (homepage on the internet) 2003, Retrieved from http://www.answers.com/topic/mesoconch.
- Morant GM (1923) A first study of Tibetian skull. Biometrika 14(3-4): 193- 260.
- Rao NB, Padmini PM (2015) A Study of Orbital Index in dry Skulls of North Coastal Andhra Pradesh. International Journal of Basic and Applied Medical Sciences 5(2): 1-3.
- Novita M (2006) Facial, upper facial, and orbital index in Batak, Klaten, and Flores students of Jember University. Dent J (Maj Ked Gigi) 39(3): 116-119.
- Rooppakhun S, Chantarapanich N, Sitthiseripratip K (2011) Advanced Medical Imaging and Reverse Engineering Technologies in Craniometric Study. Forensic Medicine - From Old Problems to New Challenges 307-326.
- Shah GV, Jadhav HR (2004) The Study of Cephalic Index in Students of Gujarat. J Anat Soc India 53(1): 25-26.
- Sharma RN (2005) Criteria of racial classification. Physical Anthropology. Surjeet Publication. 226.
- Mahajan SA, Gandhi D (2011) Cephalometric study of adult human skulls of north indian origin. International Journal of Basic and Applied Medical Sciences 1(1): 81-83.
- Strouhal E (1973) Temporal and Spacial Analysis of Some Craniometric Features in Ancient Egyptians and Nubians. In Population Biology of the Ancient Egyptians. Academic Press, London. 121-142.
- Ukoha U, Egwu OA, Okafor IJ, Ogugua PC, Onwudinjo O, et al. (2011) Orbital dimensions of adult male Nigerians: a direct measurement study using dry skulls. Int J Biol Med Res 2(3): 688-690.
- Salve VM, Londhe PS (2012) A craniometric study of adult human skulls from Andhra Pradesh. National Journal of Integrated Research in Medicine 3(1): 63-66.
- Vidya CS, Prashantha B, Gangadhar MR (2012) Anthropometric Predictors for Sexual Dimorphism of Skulls of South Indian Origin. International Journal of Scientific and Research Publications 2(10): 1-3.
- Weaver AA, Loftis KL, Tan JC, Duma SM, Stitzel JD (2010) CT scan based three-dimensional measurement of orbit and eye anthropometry. Invest Ophthalmol Vis Sci 51(10): 4892-4897.
- Weiss RA, Haik BG, Saint-Louis LA, Ellsworth RM (1987) Advanced diagnostic imaging techniques in ophthalmology. Adv Ophthalmic Plastic Reconstr Surg 6: 207-263.





