Delirium - A Dysfunctional Circadian Rhythm
Eckle T
Associate Professor of Anesthesiology, Cardiology and Cell Biology, Department of Anesthesiology, University of Colorado Denver,Room 7121, USA.
*Corresponding Author
Tobias Eckle, M.D., Ph.D.
Associate Professor of Anesthesiology,
Cardiology and Cell Biology,
Department of Anesthesiology, University of Colorado Denver, 12700
E 19th Avenue, Mailstop B112, RC 2, Room 7121, Aurora, CO 80045,
USA.
Tel: +1-303-724 -2932/2947
Fax: +1-303-724-2852
E-mail: tobias.eckle@ucdenver.edu
Article Type: Editorial
Received: March 17, 2016; Published: March 30, 2016.
Citation: Tobias Eckle (2016) Delirium - A Dysfunctional Circadian Rhythm. Int J Anesth Res. 4(1e), 1-3. doi: 10.19070/2332-2780-160002e
Copyright: Tobias Eckle© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Critical care units are a major cause of a disrupted circadian rhythm in patients [1, 2]. Light, noise, treatments, sedatives and mechanical ventilation throughout a 24 h time period are the major offenders of circadian rhythm disruption in the intensive care unit [ICU] [2]. Interestingly, circadian disruption is frequently associated with the occurrence of delirium having a high impact on outcome and mortality in the critically ill [3-5]. Endogenous melatonin, a mirror of our circadian rhythm, seems to play an important role in the development of delirium in critical ill patients. Critically ill patients have been found to have abnormal melatonin levels indicating a disrupted circadian rhythm [6, 7]. Thus, results on melatonin expression in critical ill patients have generated a new interest in the use of exogenous melatonin and melatonin agonists to improve sleep, cognitive function or delirium. In fact, a very elegant randomized controlled trial recently demonstrated effectiveness in the use of a melatonin agonist (Ramelteon) versus placebo in the prevention of delirium [8].
Patients admitted to the ICU are at a very high risk of developing abnormal sleep. As such the effect of admission to the ICU on sleep was recognized by providers early in the history of intensive care, and ICU survivors consistently list insomnia and sleep disruption as among the most difficult aspects of their illness [3]. Furthermore, the effects of ICU admission and critical illness on sleep often persist beyond discharge. In one study, 44% of patients reported persistent difficulty sleeping three months after discharge [3]. One line of evidence in support of circadian dysrhythmias as a cause of delirium has been the observation that circadian disruption and sleep fragmentation often precede the development of delirium. In fact, these prodromal symptoms, including inattention, irritability, restlessness, and dysphoria are all common symptoms of a broad range of circadian rhythm disorders such as jet lag and shift-work sleep disorder. Dementia and age-related cognitive decline, themselves strong predictors of delirium risk, have also been linked with increased sleep fragmentation [3].
What is happening, however, at the cellular and molecular levels to cause delirium is only partially understood. In fact, mechanistic studies are lacking and a molecular mechanism is not identified yet. While the analysis of circadian rhythm proteins and their misalignment in humans seem difficult to assess, melatonin levels are an excellent surrogate for a circadian rhythm. As such sleep restriction has been shown to affect melatonin levels and circadian rhythms inhumans. On a molecular level, a mutation of the human circadian rhythm protein Period 2 leads to a sleep disorder that is known as ‘familial advanced sleepphase syndrome’. Interestingly, to identify somebody with this disease, early-morning serum melatonin levels are widely used andvalidated. Based on current literature it is very compelling that circadian rhythms with their impact on sleep might play an important role in the pathogenesis of delirium [9]. Further research on expression and function of circadian rhythm proteins such as Period 2 or melatonin in the setting of critical care and delirium could therefore help to understand mechanisms and find new therapeutics.
As light is an integral component of our circadian rhythm [2, 10], bright light therapy has been shown to have therapeutic effects for sleeping disorders and other disease such as depression, dementia or seasonal affective disorder [7]. Bright light therapy has also been useful for the prevention of delirium in post-operative patients, and is also a promising adjunctive therapy in patients with established delirium [11]. A study on postoperative patients found lower delirium scores and an earlier start of ambulation in the intervention group. Another elegant study performed by Barroso and Brinker using a mathematical model of circadian rhythms in critically ill patients hypothesized that with 6 hours of medium bright light, 10 hours of normal light (artificial light in a room) and 8 hours of darkness, patients could reach their maximal circadian rhythm amplitudes in three days [7]. In addition, they demonstrated that darkness was equally important as light for a functional circadian rhythm, since even a minimal intensity of light during the theoretical night-time considerably reduced the amplitude of melatonin secretion. They therefore concluded that a comfortable intensity of bright light during the morning and an assured dark period of night was a sufficient strategy for enhancing circadian rhythms in critically ill patients [7].
Only a few attempts have been made so far to minimize chrono-disruption in critical ill patients by enhancing the daynight contrast. This might be due to the fact that it still seems less important to most health care providers. From an evolutionary standpoint, however, it seems equally important as monitoring oxygen levels:
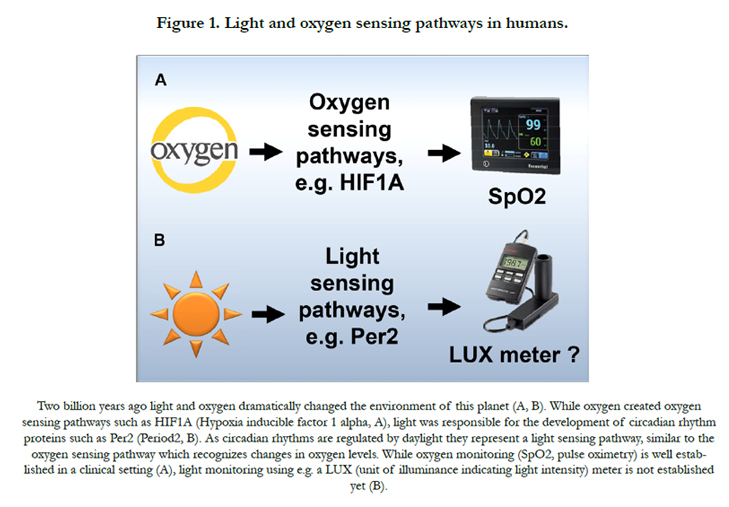
Two billion years ago, the appearance of light and oxygen dramatically changed the environment on our planet [4]. Oxygen led to the development of oxygen sensing pathways within organisms [12]. However, while oxygen sensing pathways are well established in the medical field, light sensing pathways are less known. It seems almost unknown that the appearance of sunlight created circadian rhythm proteins that represent a light sensing pathway in all humans. In fact, both pathways share several similarities as proteins in both groups belong to the same protein family that is believed to be able to sense oxygen, metabolism or light [2, 4, 10]. Nevertheless, monitoring of the light environment in a clinical setting such as the ICU is not fully appreciated yet and needs still to be established (Figure 1).
Other interventions than bright light to treat delirium include reducing the volume on telephones, earplugs, grouping patient care activities when possible, appropriate sedation, early mobilization and even ensuring patient orientation with respect to time [10]. However, if one single treatment will ever be the golden bullet needs to be proven yet. In fact, we have to realize that many common clinical scenarios can disrupt circadian rhythms, such as severe illness, stress, noise, surgery, sepsis, drugs, light at night and much more. Therefore, a single therapy might not be sufficient in restoring disrupted circadian rhythms in critical ill patients. More likely, a combination of melatonin agonists, daylight in the ICU during daytime, noise reduction at night, light reduction during the night together with optimized sedation and weaning protocols might help to restore disrupted circadian rhythms and eventually might improve mortality in critical illness [13].
In summary, monitoring of the ICU environment that could provide feedback to caregivers on common offenders (light, noise, temperature, etc.), in addition to systems that are capable to monitor circadian rhythms (actigraphy, melatonin course, etc.), could be important to minimize circadian disruption and consequently the development of delirium in the ICU. Finally, exploring the underlying molecular mechanism of delirium and its association with circadian rhythm proteins bears the potential for novel therapies, which are urgently needed as no specific therapy is available yet.
References
- Brainard J, Gobel M, Bartels K, Scott B, Koeppen M, et al. (2015) Circadian Rhythms in Anesthesia and Critical Care Medicine: Potential Importance of Circadian Disruptions. Semin Cardiothorac Vasc Anesth 19(1): 49-60.
- Brainard J, Gobel M, Scott B, Koeppen M, Eckle T (2015) Health Implications of Disrupted Circadian Rhythms and the Potential for Daylight as Therapy. Anesthesiology 122(5): 1170-1175.
- Scott BK (2015) Disruption of Circadian Rhythms and Sleep in Critical Illness and its Impact on the Development of Delirium. Curr Pharm Des 21(24): 3443-3452.
- Eckle T (2015) Editorial: Health Impact and Management of a Disrupted Circadian Rhythm and Sleep in Critical Illnesses. Curr Pharm Des 21(24): 3428-3430.
- Salluh JI, Wang H, Schneider EB, Nagaraja N, Yenokyan G, et al. (2015) Outcome of delirium in critically ill patients: systematic review and metaanalysis. BMJ 350: h2538.
- Bellapart J, Boots R (2012) Potential use of melatonin in sleep and delirium in the critically ill. Br J Anaesth 108(4): 572-580.
- Madrid-Navarro CJ, Sánchez-Gálvez R, Martinez-Nicolas A, Marina R, Garcia JA, et al. (2015) Disruption of circadian rhythms and delirium, sleep impairment and sepsis in critically ill patients. Potential therapeutic implications for increased light-dark contrast and melatonin therapy in an ICU environment. Curr Pham Des 21(24): 3453-3468.
- Hatta K, Kishi Y, Wada K, Takeuchi T, Odawara T, et al. (2014) Preventive effects of ramelteon on delirium: a randomized placebo-controlled trial. JAMA Psychiatry 71(4): 397-403.
- Fitzgerald JM, Adamis D, Trzepacz PT, O'Regan N, Timmons S, et al. (2013) Delirium: a disturbance of circadian integrity? Med Hypotheses 81(4): 568-576.
- Eckle T, Hartmann K, Bonney S, Reithel S, Mittelbronn M, et al. (2012) Adora2b-elicited Per2 stabilization promotes a HIF-dependent metabolic switch critical for myocardial adaptation to ischemia. Nat Med 18(5): 774-782.
- Yang J, Choi W, Ko YH, Joe SH, Han C, et al. (2012) Bright light therapy as an adjunctive treatment with risperidone in patients with delirium: a randomized, open, parallel group study. Gen Hosp Psychiatry 34(5): 546-551.
- Eltzschig HK, Carmeliet P (2011) Hypoxia and inflammation. N Engl J Med 364: 656-665.
- Scott B, Eckle T (2016) The impact of sedation protocols on outcomes in critical illness. Ann Transl Med 4(2): 33.





