Spinal Anesthesia for Transurethral Resection of Prostate: Levobupivacaine with or without Fentanyl
Maniyar F1*, Trishala Jain2, Praveen Kumar Ojha3
1 PG Resident, Sawai Man Singh Medical College, Jaipur, India.
2 Professor, Sawai Man Singh Medical College & hospitals, Jaipur, India.
3 PG resident, SMS medical college, Jaipur.
*Corresponding Author
Farooq Maniyar,
PG Resident, Sawai Man Singh Medical College, Jaipur, India.
Tel: 9462587809
Fax: 9549197320
E-mail: drfarooqmaniyar@gmail.com
Received: October 19, 2016; Accepted: November 29, 2016; Published: November 30, 2016
Citation: Maniyar F, Trishala Jain, Praveen Kumar Ojha (2016) Spinal Anesthesia for Transurethral Resection of Prostate: Levobupivacaine with or without Fentanyl. Int J Anesth Res. 4(11), 358-357. doi: dx.doi.org/10.19070/2332-2780-1600074
Copyright: Maniyar F© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The aim of the present study was to compare the characteristics of spinal blocks produced by low dose levobupivacaine (0.5%) and compare it when combined with fentanyl in transurethral resection of prostate.
Methods: With Institutional ethical committee clearance a prospective, randomized, double-blinded study conducted. After obtaining informed written consent a total of 140 patients scheduled for elective TURP were randomly allocated into one of the two groups of 70 patients each. Following a spinal tap, patients in Levobupivacaine Group(L) received 1.5 ml of 0.5% isobaric levobupivacaine and in Levobupivacaine - Fentanyl Group (LF) received 1 ml of 0.5% isobaric levobupivacaine with fentanyl 25 μg (0.5 ml) intrathecally. The characteristics of sensory and motor block, hemodynamic data, side effects, patient and surgeon satisfaction were recorded.
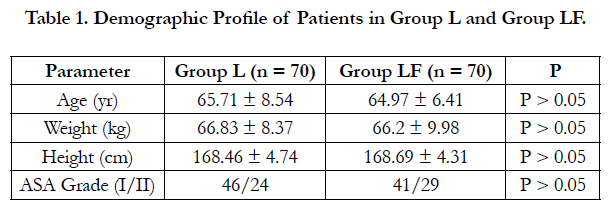
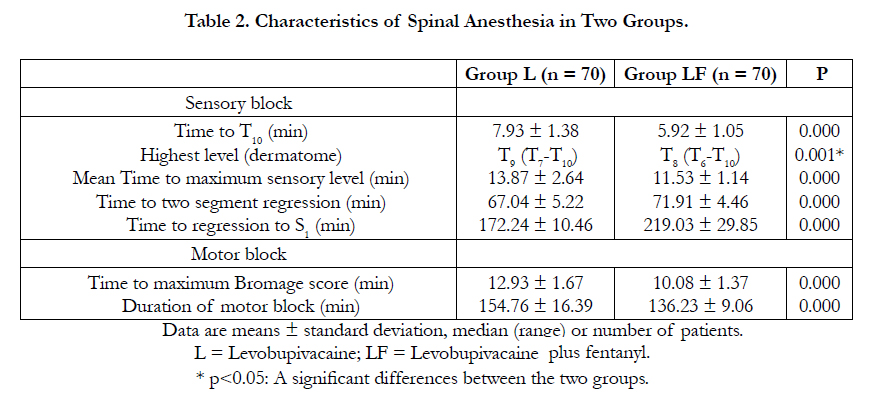
Results: There were no significant differences between the two groups for patient demographic, intraoperative hemodynamic parameters, side effects and satisfaction. The highest level of sensory block was T9 in the Group L, and T8 in the Group LF (p = 0.001). Duration of motor block was shorter in Group LF than in Group L (154.76±16.39 minutes in Group L; 136.23±9.06 minutes in Group LF) (p = 0.001).
Conclusion: Both regimes are effective, and the addition of fentanyl to levobupivacaine may offers prolong duration of sensory block and postoperative analgesia and the advantage of shorter duration of motor block, thus it may be used as an alternative to pure levobupivacaine solution in spinal anaesthesia, for transurethral resections.
2.Introduction
3.Materials and Methods
4.Statistical Analysis
5.Results
6.Discussion
7.Conclusion
8.References
Keywords
Anaesthetic Technique; Anaesthesia; Spinal; Anaesthetics; Local, levobupivacaine; Analgesics; Opioid; Fentanyl.
Introduction
Spinal anaesthesia is the most commonly used technique for infraumbilical surgeries because of its unmatchable reliability, cost effectiveness, effective analgesia, muscle relaxation and prolonged postoperative analgesia [1]. Recent advances in anaesthesia has allowed more surgeries to be performed on day case basis [2]. The properties of an anaesthetic agent used for day case surgeries in spinal anaesthesia should have decreased incidence of anaesthesia related complications, should provide adequate postoperative analgesia and allow early patient discharge [3]. Spinal anaesthesia is widely used for transurethral resections because it allows early recognition of symptoms caused by over hydration, transurethral resection of prostate (TURP) syndrome, and bladder perforation. Many patients undergoing TURP are elderly and have coexisting pulmonary or cardiac disease [4]. By reducing the dose of local anaesthetic used, side effect can be decreased. Levobupivacaine, a pure S(−) enantiomer of bupivacaine is a long acting amide local anaesthetic which produces differential neuraxial block, that is early onset and prolonged duration of sensory block with shorter duration of motor block and lower cardiac toxicity [5]. Levobupivacaine has been widely used in ambulatory surgeries after the development of low dose spinal anaesthesia technique [6,7]. To improve the block characteristics of intrathecally administered low dose local anaesthetics, addition of adjuvant is must. Intrathecal opioids enhance sensory block without prolonging motor and sympathetic block [8,9]. Among them, Fentanyl has rapid onset of action, binds strongly to plasma proteins and potentiates the afferent sensory blockade thus facilitates reduction in the dose of local anaesthetics [10,11]. Literature is available where spinal block characteristics of plain levobupivacaine were compared with fentanyl as an adjuvant to decreased doses of levobupivacaine given intrathecally [6,12,13,14]. The objective of the present study was double fold; to compare the characteristics of spinal blocks produced by 0.5% levobupivacaine with and without fentanyl and to test the hypothesis that, fentanyl added to levobupivacaine, may be used as an alternative to pure levobupivacaine solution, in a group of patients undergoing transurethral resection of prostate surgery under spinal anesthesia.
Materials and Methods
After obtaining the approval of the our Institutional Ethics Committee and patient's informed consent, 140 male patients, aged < 85 years, weight <100kg, height >145cm, ASA grade I and II patients scheduled for elective TURP operations were included in a prospective, randomized, double blind study. Patients with unwillingness for the procedure, coagulation or neurological disorders, septicaemia, deformity or previous surgery of spine, morbid obesity and allergy to the study drug were excluded from the study. Patients were randomly divided into two groups of 70 each using chit in box method.
A day before surgery detailed pre-anaesthetic check-up was done. General physical examination along with proper systemic examination, assessment of airway and local examination of lumbar spine was done. Relevant investigations were reviewed. Visual analogue scale (VAS) was explained to the patients to determine the level of analgesia in the postoperative period. Patients were asked to restrict solids and fluids by mouth at least 6 h before surgery.
None of the patients received any premedication. Patients were monitored non-invasively for systolic and diastolic blood pressure, peripheral oxygen saturation, respiratory rate, heart rate (HR), and electrocardiography evaluations. Patients were preloaded with 8 ml/kg sodium chloride solution over 15–20 min. Under all aseptic precautions, spinal anaesthesia was given in L3 and L4 space with 25 gauge Quincke spinal needle via midline approach in sitting position. On free flow of cerebrospinal fluid, study drug was injected intrathecally. In group L, 1.5 ml of 0.5% isobaric levobupivacaine and in group LF 1 ml of 0.5% isobaric levobupivacaine plus 0.5 ml fentanyl (25 μg) was injected. Study drug was prepared in similar syringes keeping the drug volume constant by an anaesthesiologist, who then handed over the syringe to another anaesthesiologist who performed the spinal block and also monitored all the patient variables. Patients were immediately turned to supine position and oxygen was given at the rate of 4 L/min by Venti-mask. Continuous monitoring of respiratory rate, HR, non-invasive SBP and DBP, SpO2 and ECG was done at 0 min, 3 min and 5 min, then at an interval of every 5 min up to 30 min and then every 10 min till the end of surgery. Hypotension, defined as a decrease of systolic blood pressure by more than 20% from baseline or a fall below 90 mmHg, was treated with incremental IV doses of IV mephentermine 5 mg and IV fluid titrated according to blood pressure. Bradycardia, defined as heart rate < 55 bpm, was treated with IV atropine 0.3-0.6 mg.
Sensory block was assessed by loss of sensation to pin prick in the midline every 2 min for first 15 min and then at an interval of 5 min till no change in level occurred. Onset of sensory block (when patient does not feel pin prick at T10 level), highest level of sensory block achieved, time to maximum sensory block, Time to two segment regression of sensory block and total duration of sensory block (regression to S1 dermatome) was noted. Motor block was assessed by using the modified Bromage scale15, every 2 min up to 20 min and then at an interval of 10 min till the completion of surgery. Maximum motor block achieved, time to maximum motor block and total duration of motor block (motor recovery to Bromage [0] was noted. All parameters were noted by taking the time of giving the study drug intrathecally as time 0. Surgery was allowed to start when sensory block to T10 dermatome was achieved. Otherwise, general anesthesia was applied.
In the postoperative period, patients were monitored for haemodynamic parameters and postoperative analgesia using VAS score, every 15 min for 120 min, then half hourly for 180 min, hourly for 12 h and thereafter every 3 hourly till 24 h of surgery in both groups. Rescue analgesia in the form of injection tramadol hydrochloride intramuscularly was given when VAS >3 in both groups. Time at which patient demanded first dose of rescue analgesia was taken as total duration of analgesia. Number of doses of rescue analgesia required in the postoperative period was also noted. Patients were monitored for any side effects or complications like hypotension, bradycardia, nausea, vomiting, sedation, urinary retention, pruritis, headache, backache and neurological changes for 24 hours. Nausea and vomiting were treated with Inj. Ondemsetron 4 mg iv. Volume of glycine used, duration of surgery and patient and surgeon satisfaction were recorded at the end of the operation. Patient satisfaction score was generated by general questioning of the patients regarding their experience of anesthesia during intra- and post-operative period. It was analyzed as: 5 – Very satisfied, 4 – satisfied, 3 – neutral, 2 – dissatisfied, 1 – very dissatisfied. Likewise, the surgeon was asked to estimate the operating conditions on a scale of excellent, good, fair and poor. Patients were observed until the level of sensory block was S1 and the Bromage score was 0.
The patients were discharged from the recovery room after the motor block was completely resolved, had stable vital signs, minimal nausea or vomiting and no severe pain or bleeding.
Statistical Analysis
Power analysis was done. Effective size/power of the study was determined by taking in to account the mean onset of sensory block, mean duration of sensory block and total duration of analgesia. The power was well above 90% by taking α error 0.05. The data from the present study was systematically collected, compiled and statistically analyzed using software IBM SPSS 17.0 (IBM Chicago SPSS Inc) to draw relevant conclusions. Data was expressed as mean and standard deviation, number and percentages. The patient characteristics (nonparametric data) was analysed using the “Chi-square tests” and the inter group comparison of the parametric data was done using the “unpaired t-test.” The P value was finally determined to evaluate the level of significance. P < 0.05 was considered as significant at 5% significance level; P < 0.01 was considered significant at 1% significance level and P < 0.001 was considered highly significant.
Results
In the present study, both groups were comparable with respect to demographic characteristics, baseline haemodynamic parameters and duration of surgery as shown in Table 1. After administering the study drug intrathecally, the mean time taken for onset of sensory block to T10 dermatome and the time to maximum sensory block in group L was more as compared to group LF and the difference was highly significant (P = 0.000). However the median maximum sensory level reached in group L was T9 dermatome and in group LF was T8 dermatome. Median maximum motor block achieved in both the groups was Bromage 2. But the mean time taken for achieving Bromage 2 motor block was more in group L as compared to group LF and the difference was highly significant (P = 0.000). The mean time to two segment regression taken in group L was 67.04 ± 5.22 minutes and in group LF was 71.97 ± 4.46 minutes. The difference in mean time to two segment regression was highly significant between the two groups (p value < 0.001). The mean time of total duration of sensory block (that is time to regression to S1 dermatome) in group L was 171.24 ± 10.46 minutes and in group LF was 219.03 ± 29.85 minutes. The difference was highly significant between group L and group LF (p value <0.001). The mean time of total duration of motor block in group L was 154.76 ± 16.39 minutes and in group LF was 136.23 ± 9.06 minutes. The difference in mean time of total duration of complete motor block was highly significant between group L and group LF (p value <0.001) as shown in Table 2.

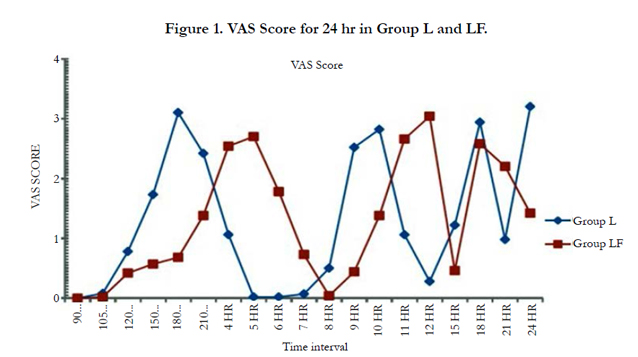
Visual analog scale score was used to monitor the patients for postoperative pain. VAS was 0 at 90 min of the study period then it started increasing in both the groups. VAS was on higher side in group L as compared to group LF as shown in Figure 1. Hence duration of analgesia was significantly prolonged in group LF (197.79 ± 29.71 min) as compared to group L (154.71 ± 10.89 min), (P = 0.000). The total number of doses of rescue analgesia required in 24 h was also significantly less in group LF as compared to group L (P = 0.000). Quality of surgical analgesia was excellent in both groups as none of the patient required supplementary analgesia intra-operatively.
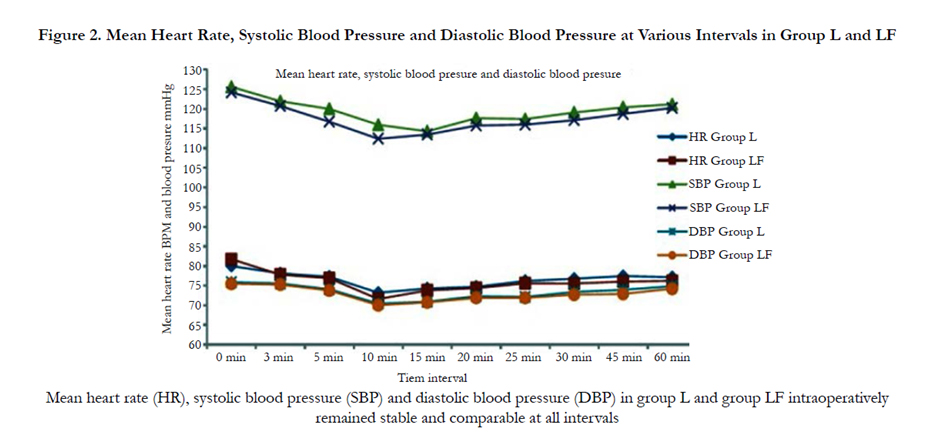
Patients were monitored for hemodynamic parameters at various time intervals starting from baseline till 24 h. There was no significant change in HR from baseline in both the groups throughout the study period. One patients (1.42%) in group LF and two patients (2.85%) in group L (P = 0.24) developed bradycardia during initial 10–15 min interval intraoperatively for which injection atropine sulphate was given. SBP and DBP also remained stable and comparable throughout the study as shown in Figure 2. In group L, 2 (2.85%) patients and in group LF, 1 (1.42%) patients (P = 0.50) had fall in SBP during 10–15 min interval intraoperatively and the percentage fall in SBP and DBP at 10 and 15 min was also comparable in both groups. Oxygen, additional IV fluids and injection mephentermine was given for treating hypotension. Respiratory rate and SpO2 was monitored and remained stable and comparable and none of the patient developed respiratory depression in both groups.
Patients were monitored for side effect and complications for 24 h. None of the patient had nausea and vomiting, headache or backache in the postoperative period. two (2.85%) patients in group LF had pruritis in the postoperative period whereas none of the patient in group L had pruritis. (P =0.04). At the end of the study, patient satisfaction score was comparable (in group L: 4.63 ± 0.67 and in group LF: 4.67 ± 0.66; P = 0.847) in both the groups as patients were satisfied with anaesthesia and analgesia in both groups.
Discussion
Spinal anaesthesia is a commonly used technique for infraumbilical surgeries, as it provides faster and effective onset of sensory and motor block and prolonged postoperative analgesia[1]. Levobupivacaine is a preferred local anaesthetic due to its longer sensory block, lower cardiac and central nervous system toxicity and shorter motor block. It produces localized anesthesia by blocking the transmission of action potential in sensory, motor and sympathetic nerve fibers, by inhibiting the passage of sodium ions through voltage sensitive ion channels in the neuronal membrane [5]. Intrathecal opioids as an adjuvant to low dose local anesthetics, produces a synergistic effect by acting directly on the opioid receptors in the spinal cord [16]. Fentanyl stimulates both μ1 and μ2 receptors and potentiates the afferent sensory blockade [11]. Studies reported that addition of 25 μg fentanyl to LA improves anesthesia quality and prolongs postoperative analgesia without prolonging the time to void [18].
The results of the present study demonstrated that addition of fentanyl to levobupivacaine improves the sensory and motor block characteristics, prolongs postoperative analgesia with decreased requirement of rescue analgesics in the postoperative period, without increasing the incidence of side effect and complications. In the present study, time to onset of sensory block and the time to achieve maximum sensory and motor block was more rapid, the duration of sensory block and postoperative analgesia was more prolonged in levobupivacaine and fentanyl group as compared to plain levobupivacaine group. Maximum sensory level in group L was T9 and in group LF was T8 dermatome but the maximum motor block was Bromage 2 in both groups. Requirement of postoperative rescue analgesics was also less in group LF.
Ozyilkan et al., [18], compared 2.2 ml of levobupivacaine plain with 10μg fentanyl or 2.5μg sufentanil as adjuvant in spinal anesthesia for caesarean section. Onset of sensory and motor block was achieved more rapidly in fentanyl and sufentanil group (P < 0.001). Duration of sensory and motor block and time for first analgesic requirement was longer in adjuvant groups as compared to plain group (P < 0.001) Akan et al., [13]. while using 10 mg plain levobupivacaine and comparing it with 7.5 mg levobupivacaine plus 25μg fentanyl and 7.5 mg levobupivacaine plus 2.5μg sufentanil in patients undergoing transurethral resection of the prostate under spinal anaesthesia concluded that combining lower doses of levobupivacaine with fentanyl and sufentanil provides faster onset of sensory block, lower frequency and shorter duration of motor block and prolonged analgesia time.
Cuvas et al., [12], also added 15 μg fentanyl to lower dose (2.3 ml) of levobupivacaine and compared it with 2.5 ml of plain levobupivacaine. The time to onset of sensory and motor block, regression of sensory block to S1 was similar in both groups. Duration of motor block was shorter in fentanyl group. Again the dose of levobupivacaine used was less in this group. Addition of fentanyl to levobupivacaine resulted in higher sensory level (T6) as compared to plain levobupivacaine (T9) which was almost similar to the findings of the present study (T8 in group LF and T9 in group L). The difference in the level of sensory block in both the groups can be explained by the difference in the bariacity of the injected solutions. Opioids are hypobaric and when added to hypobaric LA will make the mixture more hypobaric thus altering the density of resulting solution which effects the direction and extent of spread in spinal block.
Girgin et al., [6] while using 5 mg levobupivacaine plus 25 μg fentanyl and 7.5 mg levobupivacaine plain demonstrated that maximum sensory level was T7 and T6 respectively; however the maximum motor block achieved was Bromage 2 in both groups.
Heart rate and blood pressure remained stable and comparable in both the groups intraoperatively as well as postoperatively. Bradycardia was observed in 1 (1.42%) patients in group LF and 2 (2.85%) patients in group L and hypotension was seen in 2 (2.85%) patients in group L and 1 (1.42%) patients in group LF. Similar findings were reported by a previous study, where incidence of bradycardia was 15% when 10 mg of levobupivacaine was given intrathecally [14]. Chattopadhyay et al., [19] concluded that addition of fentanyl to levobupivacaine does not increase the incidence of bradycardia. Akan et al., [13] also concluded that there was no significant difference in the mean heart and blood pressure in plain levobupivacaine group and levobupivacaine plus fentanyl group. Similar results were reported by Cuvas et al., [12] and Lee et al., [20].
The most common side effect observed with intrathecal fentanyl was pruritis which was observed in 2 (2.85%) patients in group LF and none in group L (P = 0.004). Pruritis as a side effect of intrathecal fentanyl was reported by previous studies also [6, 18, 21]. No other side effect and complications were observed in both the groups. Patients were satisfied with the surgical analgesia and postoperative analgesia in both the groups. Similar patient satisfaction scores were reported by Lee et al., [20] and Cuvas et al., [12].
Conclusion
Both regimes were effective in providing surgical anaesthesia and haemodynamic stability, but group LF offered an advantage of rapid onset of sensory and motor block and prolonged duration of sensory block and postoperative analgesia, thus decreasing the doses of rescue analgesia in the postoperative period and shorter motor block.
References
- Casey WF (2000) Spinal anaesthesia - A practical guide. Update Anaesth.12: 1–7.
- Hadzic A, Karaca PE, Hobeika P, Unis G, Dermksian J, et al., (2005) Peripheral nerve blocks result in superior recovery profile compared with general anesthesia in outpatient knee arthroscopy. Anesth Analg. 100(4): 976–81.
- Redmond M, Florence B, Glass PS (2003) Effective analgesic modalities for ambulatory patients. Anesthesiol Clin North America. 21(2): 329–46.
- Mebust WK, Holtgrewe HL, Cockett ATK, Peters PC (2002) Transurethral prostatectomy: immediate and postoperative complications.Cooperative study of 13 participating institutions evaluating 3,885patients. J Urol. 167(1): 5-9.
- Foster RH, Markham A (2000) Levobupivacaine: A review of its pharmacology and use as a local anaesthetic. Drugs. 59(3): 551–79.
- Girgin NK, Gurbet A, Turker G, Bulut T, Demir S, et al., (2008) The combination of low-dose levobupivacaine and fentanyl for spinal anaesthesia in ambulatory inguinal herniorrhaphy. J Int Med Res. 36(6): 1287–92.
- Onur O, Sibel AM, Mustafa A, Mehmet Y (2010) Comparison of the effects of intrathecal different dosage of levobupivacaine in elective day-case arthroscopy of the knee. Middle East J Anaesthesiol. 20(5): 703–8.
- Wang C, Chakrabarti MK, Whitwam JG (1993) Specific enhancement by fentanyl of the effects of intrathecal bupivacaine on nociceptive afferent but not on sympathetic efferent pathways in dogs. Anesthesiology. 79(4): 766–73.
- Ben-David B, Solomon E, Levin H, Admoni H, Goldik Z (1997) Intrathecal fentanyl with small-dose dilute bupivacaine: Better anesthesia without prolonging recovery. Anesth Analg. 85(3): 560–5.
- Janicki PK, Parris WE (2003) Clinical pharmacology of opioids: Drugs for Pain. Hanley and Belfus, Philadelphia.97–118.
- Goel S, Bhardwaj N, Grover VK (2003) Intrathecal fentanyl added to intrathecal bupivacaine for day case surgery: A randomized study. Eur J Anaesthesiol. 20(4): 294–7.
- Cuvas O, Basar H, Yeygel A, Turkyilmaz E, Sunay MM (2010) Spinal anesthesia for transurethral resection operations: Levobupivacaine with or without fentanyl. Middle East J Anaesthesiol. 20(4): 547–52.
- Akan B, Yagan O, Bilal B, Erdem D, Gogus N (2013) Comparison of levobupivacaine alone and in combination with fentanyl and sufentanil in patients undergoing transurethral resection of the prostate. J Res Med Sci. 18(5): 378–82.
- Krobot R, Bacak I, Premuzic J (2005) Levobupivacaine-fentanyl spinal anaesthesia for transurethral urologic surgery. Eur J Anaesthesiol. 22: 899–903.
- Guler G, Cakir G, Ulgey A, Ugur F, Bicer C, et al., (2012) A comparison of spinal anaesthesia with levobupivacaine and hyperbaric bupivacaine for caesarian sections: A randomized trial. Open J Anesthesiol. 2: 84–9.
- Scott PV, Bowen FE, Cartwright P, Rao BC, Deeley D, et al., (1980) Intrathecal morphine as sole analgesic during labour. Br Med J. 281(6236): 351–3.
- Honca M, Dereli N, Kose EA, Honca T, Kutuk S, et al., (2014) Low-dose levobupivacaine plus fentanyl combination for spinal anesthesia in anorectal surgery. Rev Bras Anestesiol. 65(5): 461-465.
- Ozyilkan NB, Kocum A, Sener M, Caliskan E, Tarim E, et al., (2013) Comparison of intrathecal levobupivacaine combined with sufentanil, fentanyl or placebo for elective caesarian section: A Prospective, Randomized, Double- Blind, Controlled Study. Curr Ther Res Clin Exp. 75: 64–70.
- Chattopadhyay S, Halder B, Saha GC, Karmakar S (2013) Comparison of two concentrations of isobaric intrathecal levobupivacaine for vaginal hysterectomy. Indian J Pain. 27:154–8.
- Lee YY, Muchhal K, Chan CK, Cheung AS (2005) Levobupivacaine and fentanyl for spinal anaesthesia: A randomized trial. Eur J Anaesthesiol. 22: 899–903.
- Akcaboy EY, Akcaboy ZN, Gogus N (2011) Low dose levobupivacaine 0.5% with fentanyl in spinal anaesthesia for transurethral resection of prostate surgery. J Res Med Sci. 16(1): 68–73.





