Effectiveness Treatment ERP on Obsessive – Compulsive Disorder (OCD)
Maleki L1*, Derakhshi H2, Esmali Kooraneh A3
1 MA Cognitive Science, Department of Psychology, Azerbaijan Shahid Madani University, Iran.
2 MA Clinical Psychology‚ Islamic Azad University, Urmia of Science and Research Branch, Iran.
3 Assistant Professor, Department of Humanistic Science, Maragheh University, Iran.
*Corresponding Author
Leila Maleki,
MA Cognitive Science, Department of Psychology,
Azerbaijan Shahid Madani University, Iran.
Tel: 9333556131
E-mail: l.malakey@yahoo.com
Received: July 31, 2015; Accepted: October 16, 2015; Published: November 04, 2015
Citation: Maleki L, Derakhshi H, Esmali Kooraneh A (2015) Effectiveness Treatment ERP on obsessive – Compulsive Disorder (OCD). Int J Behav Res Psychol, 3(9), 163-167. doi: dx.doi.org/10.19070/2332-3000-1500029
Copyright: Maleki L© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This study is aimed to consider the effectiveness of exposure therapy and Exposure Response Prevention (ERP) on decrease of symptoms of obsessive - compulsive disorder is. The research method was quasi-experimental and its design was pre-test and post-test with control group. The statistical population of this study was all patients with obsessive-compulsive disorder (both male and female) referring to therapy centers of Maragheh city that a sample of 30 subjects was chosen by available sampling method and then they were replaced in experimental (therapy) group and control group randomly and answered to Maudsley Obsessive-Compulsive Inventory (MOCI). The findings indicated that the experimental group's average score in obsessive-compulsive symptoms was 14/46 in pre-test and 7/67 in post-test. As well as, in control group, the mean score of obsessive - compulsive symptoms in pre-test was 14/66 and 11/93 in post-test. Thus, it could be concluded that the reduction of scores in post-test of experimental group was accompanied with the decrease of symptoms of obsessive - compulsive disorder in experimental group.
2.Introduction
3.Methods
4.Participants and Data Selection
5.Instruments
6.Treatment
6.1.Steps exposure and response prevention therapy sessions
7.Results
8.Conclusion
9.References
Keywords
Obsessive – Compulsive; Treatment ERP; Maudsley Obsessive Compulsive Inventory.
Introduction
Obsessive-compulsive disorder is characterized by elevated anxiety caused by uncontrollable and intrusive thoughts called obsessions, and repetitive, ritualistic behaviors called compulsions. Children and adolescents with obsessive-compulsive disorder (OCD) cannot stop their worrying and anxiety. Obsession themes may include contamination, harming oneself or others, aggression, sexual misconduct, religiosity, forbidden thoughts, symmetry urges, and the need to tell, ask, or confess. Compulsions take the form of overt behavioral acts, rituals or covert mental acts (e.g. silently counting) [15]. The adult with OCD often recognizes that their behavior is abnormal and problematic. However, due to undeveloped cognitive abilities, children with OCD may not understand that their behaviors are unreasonable. Individuals with OCD experience distress when their compulsions cannot be completed. In children, this distress may manifest as tantrums or angry outbursts. Furthermore, children may not be able to specify the consequence of not engaging in their compulsions and may report a vague sense that “something bad might happen” if they are not able to complete the compulsion [16].
With an estimated lifetime prevalence of 2.5% in adults and 1 to 2% in children and adolescents, OCD is a fairly common psychiatric disorder. Onset is most frequently between six and 15 years of age in males and between 20 and 29 years of age for females [17]. The impairment caused by OCD is significant. Because compulsions serve as the primary coping mechanism, children and adolescents with OCD experience increasing levels of distress and will respond by increasing the intensity and/or magnitude of their compulsions. Thus, these youth may spend more and more time engaging in their rituals. The child’s dependence on their ineffective coping mechanism, in turn, interferes with school, work and social functioning. Accordingly, children with OCD may be reluctant to attend school for fear of embarrassment, and they often withdraw from social activities. Children and adolescents with OCD also possess a higher risk for comorbid anxiety disorders (e.g., social anxiety and panic disorder) and depression. While symptoms may fluctuate, the overall trend in symptom severity increases over the lifetime [26].
So far, various theories as theories of behavioral, cognitive and biological have been trying to explain and provide treatment paradigms to these problems. Biological research in explaining the cause of the disease using positron emission tomography increased glucose metabolism in the cerebral cortex of the socket (orbital frontal cortex) and the core tails have been reported [19]. Another model for explaining and treating obsessive-compulsive disorder, a behavioral pattern. According to this model, obsessive thoughts are conditioned stimuli. If the answer is relatively neutral stimuli through the process of learning and pairing with harmful and anxiety-provoking events that are naturally finds continuity with fear and anxiety. In this way, ideas and objects previously neutral stimulus becomes conditional, are able to provoke anxiety and discomfort. Compulsion is there but in a different way. The person finds that particular operation reduces anxiety is an obsession. Relieve and calm the anxiety that drives hidden acts as a result of Compulsion, the operation is enhanced. This will gradually reduce the usefulness of a painful secondary drives (anxiety) as a learned behavior pattern is fixed [24]. Behavioral therapists, several techniques such as systematic desensitization, paradoxical intention, saturation, aversion therapy, thought stopping, and imaginary concept in the treatment of obsessivecompulsive disorder have used. Several experiments have been able to be effective exposure and response prevention Obsessive prove their territory. The results so far show improvement in 65- 75% of patients using this way [20]. Recently cognitive techniques in the treatment of OCD considered that evidence of cognitive components involved in the disorder. Cognitive Theory of obsessive - compulsive suggests that the interpretation of catastrophic thoughts on the importance of the cause and the continuity of the opinion [21]. The most comprehensive cognitive analysis for OCD [23]. Suggests that intrusive obsessive thoughts, stimulating the launch of certain types of thoughts are automatic. Based on this theory, an intervention that led to chaos if people will have a personal belief system, that annoying assessment and thus unacceptable negative automatic thoughts to launch (for example, only bad guys, sexual thoughts banned have). Their sense of responsibility and shame, the main subject of obsessive thought is. Compensation in the form of cognitive or behavioral procedure, an attempt to reduce the sense of responsibility and avoid that feel ashamed. Accordingly, the identification and correction of negative evaluation thoughts, correct and prevent extremist attitudes of responsible disposal of this feeling, increase exposure and avoidance behaviors to be centered [14].
This approach is especially effective in patients who complete entry exposure and response prevention therapy are afraid or resistant to treatment, because rather than encourage people to stop compulsive behaviors, abuse targeted phrases acknowledge that the person forced to perform rituals and to stop these behaviors emphasize safety. Newer studies are generally of exposure and response prevention and cognitive approach to integration and the impact of cognitive-behavioral therapy in the treatment of the symptoms of this disorder are considered. The results of these studies [11, 12, 13, 25] Shows that this would expedite the immediate consequences of treatment, a significant reduction of symptoms and reduce the risk of recurrence.
Treatment generally obsessed with individual runs and using a team approach in the treatment of obsessive not common. Until a decade ago, a group approach only as a supplement to the treatment of individuals with OCD was raised, not as a substitute for individual treatment [27]. Using this method as an alternative method for the treatment of obsessive-compulsive disorder is a completely new approach which is considered a decade ago. In this way our patients not only a passive receiver of this approach is useful in creating pressure to break the resistance of patients to treatment.
[10] analyzed the results of a controlled study was eighteen, have reached the conclusion that after the implementation of exposure and response prevention of pathological symptoms disappeared in 51% of patients, and significant improvements have been the relative improvement was observed in 31% of cases and only in 10% of patients, this method is not effective. Many studies of the effects of cognitive behavior therapy in the treatment of obsessive- compulsive disorder have supported. The carefully controlled tests of cognitive behavior therapy in adults and children have reported success of 85% treatment [8, 9].
This description is natural to assess the efficacy of exposure therapy and response prevention is very important in reducing OCD symptoms and may increase our knowledge about this disease and to prevent planning for primary, secondary and treatment, is smooth. We hope that these new findings and additional research could take a small step in the diagnosis and treatment of obsessive-compulsive disorder.
Therefore, the present study aimed at investigating the effects of Exposure and response prevention therapy can reduce symptoms of obsessive – compulsive.
Methods
This study is a quasi-experimental one (pretrial, post trail, and control group). The participants in this study were selected available and were administered maudsley obsessive compulsive inventory afterwards, the clinical interview was performed based on DSM-IV-TR diagnostic criteria. They were randomly assigned into two groups, control and norm group, before considering the dependent variable. The norm group was taught of eight sessions (two sessions a week and a half hours).
Participants and Data Selection
The participants in this study were 30 Patients with Obsessive- Compulsive Disorder (both female and male) who in the second half the 2014 referred to health centers Maragheh.
Instruments
The Maudsley Obsessive-Compulsive Inventory (MOCI) is one of the most used tests in clinical psychology for assessing the obsessive and compulsive symptoms in psychiatric patients and as a screening tool in nonclinical population. One of the psychological tests most commonly used for assessing the obsessive and compulsive symptoms is the Maudsley Obsessive- Compulsive Inventory (MOCI) developed by Hodgson and Rachman (1977). The MOCI is a self-report questionnaire with true-false format developed for evaluating the type of obsessive-compulsive symptoms and discriminating obsessive patients from other neurotic patients and from nonclinical people. The test is composed of 30 dichotomous items, so that the total score for a subject will range between 0 (absence of symptoms) and 30 (maximum presence of symptoms). The original version has four subscales: Checking (9 items), Cleaning (11 items), Slowness (7 items), and Doubting (7 items). Note that the sum of the items for the four subscales is 34, not 30, because four items are included in two subscales [7]. The MOCI can be applied to adults as well as children and adolescents. In addition, it has been applied for assessing obsessive and compulsive symptoms not only in patients with OCD, but also for other patient populations (e.g., depressive patients), and as a screening tool for nonclinical populations [6]. The MOCI is also a very sensitive instrument to therapeutic change and, as a consequence, it has been applied very frequently in empirical studies evaluating the effectiveness of psychological and/or pharmacological treatments for patients with OCD [5].
Treatment
Experimental group For two months received exposure and response prevention. Eight treatment sessions, one hour weekly sessions were presented. The content of therapy sessions include communication, knowledge of treatment goals, principles and rules of sessions, explaining the nature and causes of the disorder and its treatment, explain behavioral therapy with emphasis on exposure and response prevention and logic treatment of the symptoms of subjects, providing practical exposure and how to prevent the responses over several sessions. Five sessions 8 sessions to provide practical treatment devoted.
First session: Presentation of the logic of cognitive behavior therapy with exposure and response prevention, identification and treatment sessions fixed rules and in particular rules of each week.
Sessions II and III: Provides a list of triggers symptoms of obsessive thoughts (internal and external), and avoidance behaviors are ceremonial and regulations practices and challenging these situations and behaviors.
Fourth, Fifth and Sixth sessions of practice and preparation tomeet the visual, offering homework, reviewing assignments at the beginning of each session and the contract to cooperation clients.
Seventh and Eighth sessions: Meeting (real or figurative) and inhibition of the response to stressful stimuli [2].
Results
After gathering the data, Mean and Standard Deviation (SD) for pretrial and post trail were measured. Based on the results, the average age of 28.9 years and a mean of control group 27.2 years.
Table 1 describes the statistical pre-test and post-test scores for symptoms of obsessive-compulsive and subscales are in control and experimental groups. The results of the experimental group decreased. Before beginning to examine the hypothesis of normal distribution of variables, non-parametric tests were used Kolmogorov - Smirnov results shows, distribution of pre-post test control group and test variables with Kolmogorov normal distribution is not significant. Kolmogorov- Smirnov test results in Table 2 are shown.
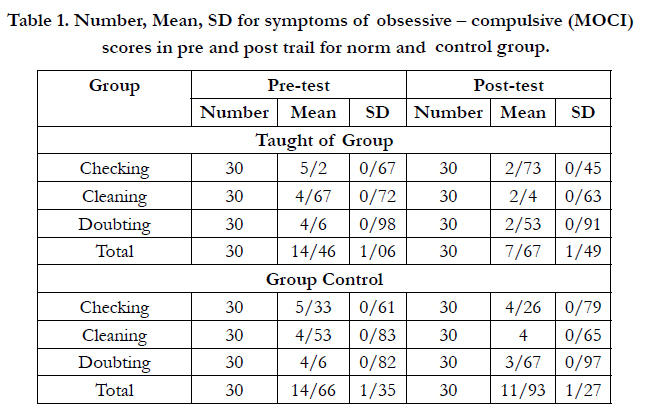

Table 1. Number, Mean, SD for symptoms of obsessive – compulsive (MOCI) scores in pre and post trail for norm and control group.
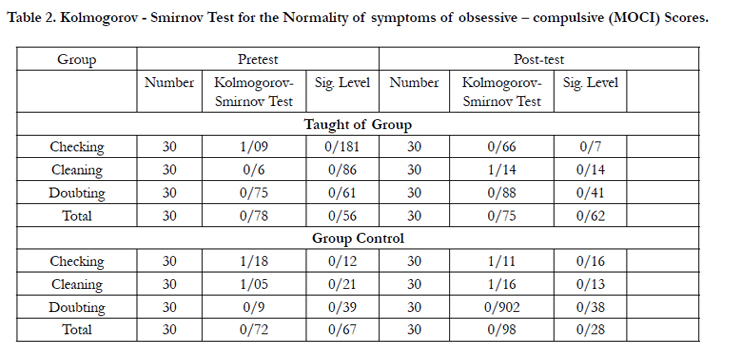
Table 2. Kolmogorov - Smirnov Test for the Normality of symptoms of obsessive – compulsive (MOCI) Scores.
According to the results (Table 3) (257/75, F=1 and 27 dF= 001/0 P =) is shown the effect of pre-test and post-test of the results of the groups elimination, the difference between groups in the there is a significant 95% confidence. Exposure and response prevention therapy can therefore be concluded (ERP) to reduce symptoms of obsessive - compulsive effective. Eta Square also indicates that 73 percent of test score changes in the variable group of obsessive-compulsive symptoms (difference between groups in the post-test) due to the implementation of the independent variables (exposure therapy and response prevention (ERP)).
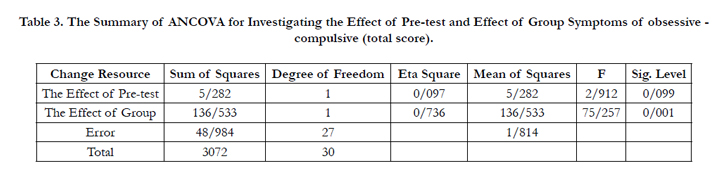
Table 3. The Summary of ANCOVA for Investigating the Effect of Pre-test and Effect of Group Symptoms of obsessive - compulsive (total score).
According to the results of Table (4) (42/39 F = 1 and 27, dF = 002/0 P =) is shown the effect of pre-test and post-test results for the group to be eliminated, the difference between groups was significant at the 95% confidence level is significant. Exposure and response prevention therapy can therefore be concluded (ERP) is effective in reducing the symptoms of obsessive-compulsive disorder checking. Eta Square also indicates that 59 percent of test score changes in the variable group, check the symptoms of obsessive-compulsive disorder (difference between groups in the post-test) due to the implementation of the independent variables (exposure therapy and response prevention (ERP)).
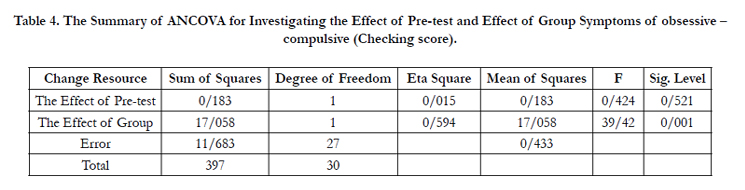
Table 4. The Summary of ANCOVA for Investigating the Effect of Pre-test and Effect of Group Symptoms of obsessive – compulsive (Checking score).
The results obtained (Table 5) (826/47, F=1 and 27 dF = 001/0 P=) is shown the effect of pre-test and post-test of the results of the groups eliminated, the difference between There is a significant level of 95% confidence. Thus, the null hypothesis is rejected and research scholars will be accepted. Exposure and response prevention therapy can therefore be concluded (ERP) reducing wash symptoms of obsessive - compulsive effective. Eta Square also indicates that 63 percent of test score changes in the variable group washing symptoms of obsessive - compulsive (difference between groups in the post-test) due to the implementation of the independent variables (exposure therapy and response prevention (ERP).
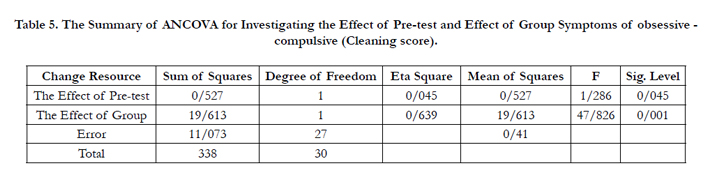
Table 5. The Summary of ANCOVA for Investigating the Effect of Pre-test and Effect of Group Symptoms of obsessive - compulsive (Cleaning score).
According to the results of Table (6) (637/12, F = 1 and 27 dF = 001/0 P =) is shown the effect of pre-test and post-test results for the group to be removed from the difference between groups is statistically significant at the 95% confidence level of significance. Thus, the null hypothesis is rejected and research scholars will be accepted. Exposure and response prevention therapy can therefore be concluded (ERP) to reduce the symptoms of OCD obsessive doubt effective. Eta Square also indicate that about 32% of test scores in variable symptoms of a compulsive OCD (difference between groups in the post-test) due to the implementation of the independent variables (exposure therapy and response prevention (ERP)).
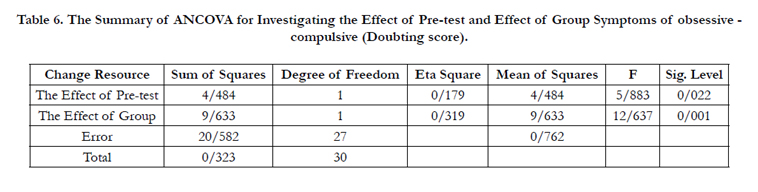
Table 6. The Summary of ANCOVA for Investigating the Effect of Pre-test and Effect of Group Symptoms of obsessive - compulsive (Doubting score).
Conclusion
Based on the results achieved by exposure therapy and response prevention (ERP) to reduce symptoms of obsessive - compulsive effective.
Occasionally men thought so, too many unintended and sometimes the passion that behave in a way that is embarrassing or even dangerous. But only a few people who are suffering from obsessive compulsive disorder. Obsessive compulsive disorder (OCD) is an anxiety disorder in which a person's mind is full of thoughts, uncontrollable and persistent and determined person would have to repeat this exercise is that it causes distress and disruption in daily functioning [4].
Emphasis on dealing with provocative situations obsessive thoughts and compulsive avoid giving answers rooted in the efforts to develop behavioral and cognitive therapy - behavior is obsessive. This approach believe that the obsessive thoughts in the form of conditioning, stress response, are linked. In such a case, if these thoughts, for a considerable time, continually conditioning are not usually conditioned response anxiety, gradually reduced and eventually shuts down. But because occurrence compulsive behaviors by patients with OCD, anxiety does not decrease, and still continues. In fact, compulsive behaviors, behaviors that are willing to deal with obsessive thoughts, their end and therefore can relieve anxiety or distress caused by obsessive thoughts. When compulsive behavior by reducing anxiety reinforces, its occurrences the likelihood of further. In addition, patients learn obsessive avoidance behaviors can be prevented obsessive thoughts, so as to deal with these thoughts, the more reduced. Therefore, exposure therapy and response prevention, the main goal of treatment is to put the person at the highest possible level of confrontation and at the same time, elimination is any kind of avoidance behavior. In this case, a conditional link between obsessive thoughts and anxiety responses, will be discrete and the person will be able to with their obsessive thoughts without being faced with high levels of anxiety [3]. Previous studies revealed that cognitive behavioral therapy is based on exposure and response prevention is effective in improving the symptoms of obsessive-compulsive disorder [1].
These findings explained that in this type of treatment in addition to identifying and correcting the negative assessments, thoughts interfering with the correct attitude of responsibility and prevent behaviors that neutralizing following a negative assessment by the sense of responsibility arises, Increased exposure and reduce avoidance behavior and So symptoms of OCD reduced.
References
- Whittal ML, Thordarson DS, McLean PD (2005) Treatment of obsessive– compulsive disorder: cognitive behavior therapy vs. exposure and response prevention. Behav Res Ther 43(12): 1559-1576.
- Baer L (2012) Getting control: Overcoming your obsessions and compulsions. Penguin.
- Hawton KE, Salkovskis PM, Kirk JE, Clark DM (1989) Cognitive behavior therapy for psychiatric problems: a practical guide. Oxford University Press, New York.
- Davison G, Neil, John, Kering N (2004) Psychopathology. Translated by Mehdi Dehestani, editing publications.
- Thordarson DS, Radomsky AS, Rachman S, Shafran R, Sawchuk CN, et al. (2004) The Vancouver Obsessional Compulsive Inventory (VOCI). Behav Res Ther 42(11): 1289-1314.
- Einstein DA, Menzies RG (2006) Magical thinking in obsessive-compulsive disorder, panic disorder and the general community. Behav Cogn Psychother 34(3): 351-357.
- Hodgson RJ, Rachman S (1977) Obsessional-compulsive complaints. Behav Res Ther 15(5): 389-395.
- Franklin ME, Foa EB (2007) Cognitive behavioral treatment of obsessive compulsive disorder. In: A guide to treatments that work. (3rd edtn), Oxford University Press, New York. 431-446.
- Barrett P, Healy-Farrell L, March JS (2004) Cognitive-behavioral family treatment of childhood obsessive compulsive disorder: A controlled trial. J Am Acad child Adolesc Psychiatry 43(1): 46-62.
- Foa EB, Steketee G, Grayson JB, Turner RM, Latimer PR (1984) Deliberate exposure and blocking of obsessive compulsive rituals: Immediate and longterm effects. Behav Ther 15(5): 450-472.
- O'Connor KP, Todorov C, Robillard S, Guay S, Pélissier MC, et al. (2006) Cognitive behavior therapy and medication in the treatment obsessive compulsive disorder. Acta Psychiatr Scand 113(5): 408-419.
- Van Balkom AJ, De Haan E, Van Oppen P, Spinhoven P, Hoogduin KA, et al. (1998) Cognitive and behavioral therapies alone versus in combination with fluvoxamine in the treatment of obsessive compulsive disorder. J Nerv Ment Dis 186(8): 492-499.
- Freeston MH, Ladouceur R, Gagnon F, Thibodeau N, Bujold A (1997) Cognitive behavioral treatment of obsessive thoughts: a controlled study. J Consult Clin Psychol 65(3): 405-413.
- Van-Noppen B, Steketee G, McCorkle BH, Pato M (1997) Group and multifamily behavioral treatment for obsessive-compulsive disorder: A pilot study. J Anxiety Disord 11(4): 431-446.
- March JS, Mulle K, Herbel B (1994) Behavioral psychotherapy for children and adolescents with obsessive-compulsive disorder: An open trial of a new protocol-driven treatment package. J Am Acad Child Adolesc Psychiatry 33(3): 333-341.
- Barrett PM, Farrell L, Pina AA, Peris TS, Piacentinit J (2008) Evidencebased psychosocial treatments for child and adolescent obsessive-compulsive disorder. J Clin Child Adolesc Psychol 37(1): 131-155.
- American Psychiatric Association (APA) (2000) Diagnostic and statistical manual of mental disorders. (4th edtn) (DSM-IV-TR), Washington, DC.
- American Psychiatric Association (APA) (2010) Diagnostic and statistical manual of mental disorders.
- Hollander E, De caria CM, Nitescu A, Gully R, Suckow RF, et al. (1992) Serotonergic function in Obsessive-compulsive disorder. Behavioral and neuroendocrine responses to oral m-chlorophenylpiperazine and fenfluramine in patients and healthy volunteers. Arch Gen Psychiatry 49(1): 21-28.
- Liebowitz MR, Foa EB, Kozak MJ, Davies S, Campeas R, et al. (2005) Randomized placebo controlled trial of exposure and ritual prevention, clomipramine and their combination in the treatment of obsessive-compulsive disorder. Am J Psychiatry 162(1): 151-161.
- Shafran R, Somers J (1998) Treating adolescent obsessive-compulsive disorder: Applications of the cognitive theory. Behav Res Ther 36(1): 93-97.
- Clark DA (2004) Cognitive behavioral therapy for OCD. Guilford Press, New York.
- Salkovskis PM (1989) Congnitive behavioural Factors and the Persistence of intrusive thoughts in obsessional Problems. Behav Res Ther 27(6): 677-682.
- Benjamin J. Sadock, Virginia A. Sadock (2012) Kaplan and Sadock's Concise Textbook of Clinical Psychiatry. (3rd edtn), Lippincott Williams & Wilkins, Philadelphia.
- Bux DA, Zoellner LA, Franklin ME, Abramowitz JS, Feeny NC (2002) Cognitive-behavioral therapy with and without medication in the treatment of obsessive compulsive disorder. Professional Psychology Research and Practice 33(2): 162-168.
- American Psychiatric Association (2005) DSM-IV-TR.152-153.
- Abramowitz JS, Foa EB, Franklin ME (2002) Empirical status of cognitivebehavior therapy for obsessive compulsive disorder: A meta-analytic review. Romania Journal of Cognitive Behavioral Psychotherapies 2(2): 89-104.





