Injected Versus Oral Deep Vein Thrombosis Prophylactic Therapy: A Patient Satisfaction Study
Banaszek D1,2, Pickell M1,2, Wood GC1,2, Campbell A1,2*
1 Human Mobility Research Center, Kingston, ON.
2 Department of Surgery, Kingston General Hospital, Kingston, ON.
*Corresponding Author
Aaron Campbell, M.D., FRCSC.
Department of Surgery, Division of Orthopaedic Surgery,
Kingston General Hospital, Victory 3-310, Kingston, ON K7L 2V7.
Tel: 613.549.6666 x. 6802
Fax: 613.548.7884
E-mail: campbea2@KGH.KARI.net
Received: March 21, 2016; Accepted: April 11, 2016; Published: April 16, 2016
Citation:Banaszek D, Pickell M, Wood GC, Campbell A (2016) Injected Versus Oral Deep Vein Thrombosis Prophylactic Therapy: A Patient Satisfaction Study. Int J Bone Rheumatol Res. 3(2), 28-32.DOI : dx.doi.org/10.19070/2470-4520-160007
Copyright: Campbell A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Deep vein thrombosis (DVT) is a serious complication of total knee replacement (TKA). While the need for post op prophylaxis is accepted, controversy exists as to which regimen(s) to use. ASA use has seen resurgence due to its efficacy, safety profile, and easy administration. To date no study has evaluated patient satisfaction and compliance with ASA chemoprophylaxis after TKA.
Ninety-six TKA patients were surveyed after randomization to receive either oral ASA or injected low molecular weight heparin. Satisfaction was significantly greater in the ASA group. Confidence in treatment was equivalent between the groups.
Patient satisfaction withanticoagulation after TKA should not be overlooked. We have demonstrated increased satisfaction with ASA treatment without affecting perceptions of efficacy. Our findings should be considered when prescribing postoperative prophylaxis
2.Introduction
3.Methods
3.1 Subjects and Treatment Course
3.2 Satisfaction Survey
3.3 Ethics and Statistical Analysis
4.Results
5.Discussion
6.References
Keywords
Aspirin; DVT Prophylaxis; Thromboembolism; Arthroplasty; Patient-Reported Outcomes; Arthroplasty.
Introduction
Venous thromboembolism (VTE) is one of the most common, and potentially devastating post-operative complications following total joint arthroplasty (TJA). Rates of pulmonary embolism (PE) without prophylaxis have been reported as high as 20% in total hip arthroplasty, and 8% in total knee arthroplasty (TKA) [1,2,3]. This is in contrast to rates of fatal PE with DVT prophylaxis, which are consistently reported at 0.1-0.2% regardless of which chemoprophylaxis is employed.4-8 As such, the use of postoperative DVT prophylaxis has become standard of care in patients undergoing these procedures. Currently accepted methods to help prevent VTE after TKA include the use of regional anesthesia, early postoperative mobilization, mechanical compression devices, and chemoprophylaxis. Despite the availability of multiple anticoagulant medications, no single chemoprophylaxis is currently deemed superior to any other [4,5,6,8].
Both the American Academy of Orthopedic Surgeons (AAOS) and the American College of Chest Physicians (ACCP) view Aspirin as a safe and effective preventative agent for VTE after TKA in low risk patients [9,10,11]. Furthermore, ASA been used as secondary preventative measure against heart attacks and strokes [12,13]. Numerous studies comparing aspirin to other chemo-prophylactic agents have demonstrated the efficacy of Aspirin [15,-18]. While some have reported an increased risk of symptomatic DVT and PE with ASA use14, other studies have demonstrated a decreased rate of hematoma formation (Figure 1), fewer issues with wound healing, and reduced serious bleeding complications [19,-24]. Additional benefits of ASA include ease of delivery, no requirement for blood monitoring, a proven longterm safety profile, and cost of treatment.
Despite much information on different chemoprophylaxis regimens, there remains a paucity of literature with respect to risk stratification and appropriate patient selection for the appropriate chemoprophylactic choice [22]. In choosing a post-op regimen one must balance the need to prevent clot formation (determined by anticoagulant potency and patient risk factors) with the risk of anticoagulant side effects, including bleeding and hematoma formation in the wound. Additionally, treatment cost and patient compliance also should be considered.
Trends in clinical research have increasingly emphasized patient reported outcome measures (PROMS) as crucial in the implementation of new treatment strategies. Informed decisionmaking is now an integral part of patient-centered medical and surgical care. In 2004, the National Institutes of Health [26] created a mandate dedicated to high-quality PROMS research. Validated PROMS questionnaires have been developed looking at multiple patient populations, including disability as it relates to mental health [27], chronic disease [28], chronic pain [29], and arthritis [30]. To date, however, the literature remains sparse with regards to patient-perceived medical treatment. Prins et al. compared oral Rivaroxaban versus standard injectable VTE prophylaxis in patients on active DVT/PE treatment as part of the EINSTEIN-PE trial [24]. This group reported significantly improved satisfaction rates in the oral medication (Rivaroxaban) cohort [24]. No studies have directly compared patient satisfaction with oral aspirin versus injected low-molecular weight heparin after total joint replacement.
We hypothesize that injectable anticoagulants create a negative experience for patients to the point that despite the additional mechanical prophylaxis, and a prolonged treatment course, patients would be significantly more satisfied with oral aspirin prophylaxis. Using a questionnaire we examined patient preference for aspirin versus injected low molecular weight heparin for DVT prophylaxis after TKA, as well as compliance, patient perceptions of efficacy and patient reported complications.
Methods
Subjects and Treatment Course
A total of 96 patients at a single academic surgical center met inclusion criteria for this prospective cohort study. All patient signed a consent form prior to study enrollment. Patient demographics were collected prior to study participation. All patients who received a unilateral primary knee replacement were considered for the study. Patients were excluded based on the limitations set forth by our institutions short stay TJA program (Figure 2) designed for the low-risk arthroplasty patient. On average, patients in this stream, have a length of stay of less than 48 hours. Additionally, patients on long-term anticoagulation for chronic conditions prior to surgery were excluded. Subjects were randomly assigned to receive either injected low molecular weight heparin (Dalteparin 5000U subcutaneous injection once daily) x 2 weeks or aspirin (ASA 162mg oral, once daily) and TED stockings x 6 weeks. In the ASA group, pneumatic compression devices (PCD) were also used immediately post-op until patients mobilized with physiotherapy.


Figure 1. Clinical Photo of a post-operative hematoma in a patient having undergone total knee arthroplasty.
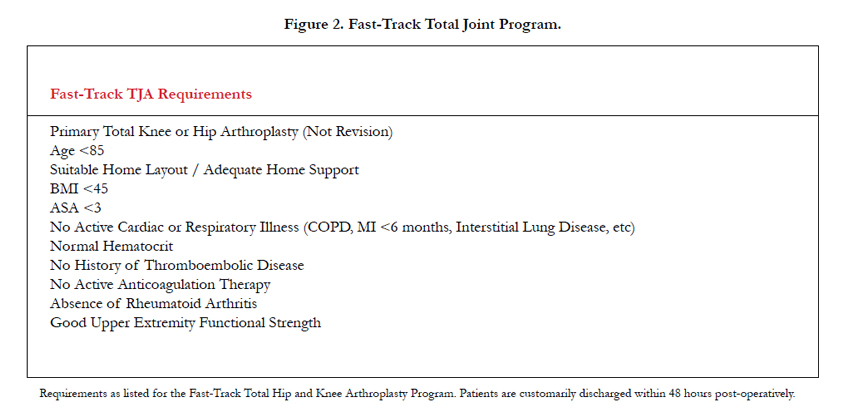
Figure 2. Fast-Track Total Joint Program.
Satisfaction Survey
All eligible consenting patients were seen postoperatively at six weeks and given the patient satisfaction survey (Figure 3). A 10-point Likert Scale was used to address patient satisfaction with treatment and confidence in efficacy of treatment to prevent blood clots. Number of doses missed or skipped was reported. Other parameters evaluated included complications associated with treatment and whether the patient experienced a blood clot. All patients enrolled in the study completed the required followup.
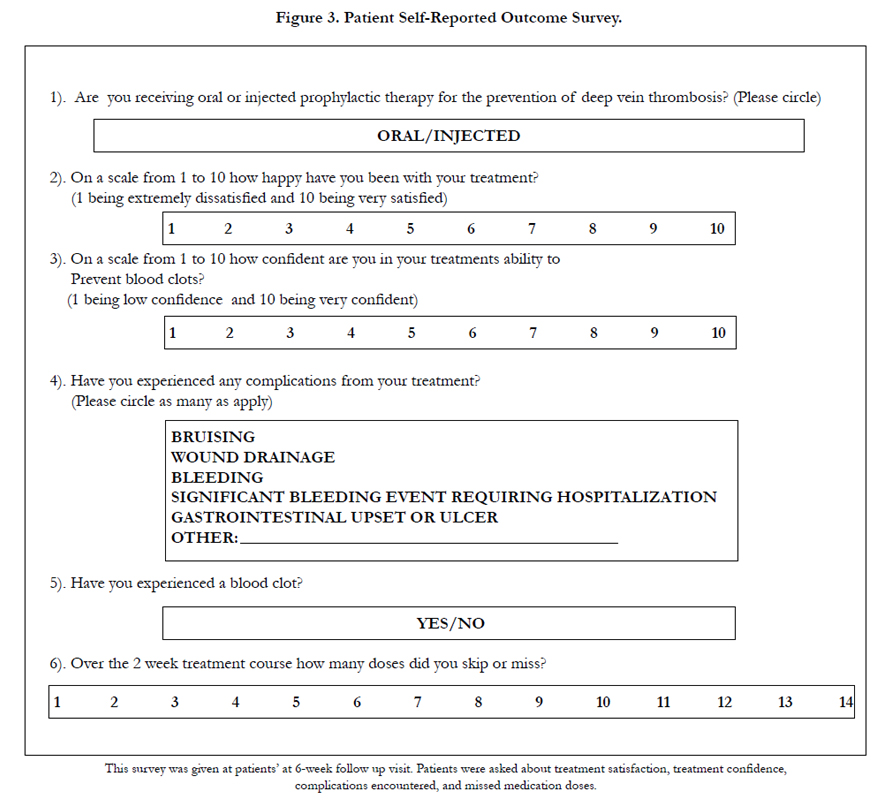
Figure 3. Patient Self-Reported Outcome Survey.
Ethics and Statistical Analysis
Ethics approval for our study was obtained through our institutions internal Institutional Review Board (IRB). Descriptive statistics were used to summarize variables. Non-parametric Mann- Whitney and Chi-square tests were used to determine if significant differences existed between the oral and injected groups on studyvariables. An alpha value of less than .05 was considered statistically significant.
Results
Ninety six patients completed the survey; 48 in each group. Patient satisfaction was significantly greater in the patients treated with oral DVT prophylaxis (p<0.01). The reported mean satisfaction rate with oral aspirin was 9.4/10 compared with 7.3/10 for subcutaneous injected treatment. There was no statistical difference in patient confidence in the efficacy of prophylaxis between the 2 treatment groups (p>0.05) (Table 1).
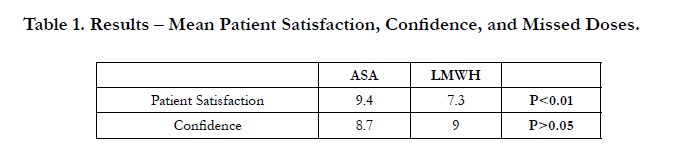

Table 1. Results – Mean Patient Satisfaction, Confidence, and Missed Doses.
Ten subjects overall reported missing a dose. In the injected group patients in the reported missing a total of 25 doses for a dose compliancy rate of 96.2% (647 of 672 doses administered correctly). Comparatively 2 patients in the oral ASA group missed a total of 7 doses for a dose compliancy rate of 99.8% (4025 of 4032 doses administered correctly).
More complications were experienced in the Injected LMWH group than the ASA group (60% vs. 31%, p=.01) (Table 2). The most common complication was bruising which occurred significantly more frequently in the injected group (52%) versus in the oral group (19%) (p<0.01). No patients experienced a blood clot in either treatment group.
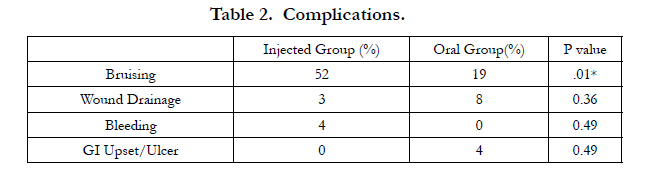
Table 2. Complications.
Discussion
The benefits of VTE prophylaxis after total joint replacement surgery have rendered this treatment standard of care among postoperative arthroplasty patients. Cordell-Smith et al. reported that proximal thrombi were found in 11.0% of TKRs and in 14.8% of THRs in patients not receiving routine VTE prophylaxis [3]. There is, however, currently no universally accepted medication regimen for this patient population. The lack of adequate high quality research has called into question the routine use of injected low molecular weight heparin as standard chemoprophylaxis. Furthermore, recent ACCP and AAOS guidelines have advocated for ASA use as an effective and safe alternative [9-11]. In a recent study, Nam et al. concluded that the addition of oral aspirin to mechanical prophylaxis was a safe alternative to warfarin therapy in patients after bilateral TKR, traditionally viewed as a high-risk group [23]. As such, surgeons must consider individual patients needs and the overall benefits and risks prior to determining and post op regimen TKA.
Our findings indicate that in an eligible, low-risk population, knee arthroplasty patients prefer oral aspirin to injectable VTE prophylaxis. These are consistent with a study conducted by Prins et al., in which oral rivaroxaban was compared to standard injectable VTE prophylaxis in patients on active DVT/PE treatment in the EINSTEIN-PE trial. They reported significantly improved satisfaction rates in the oral medication cohort [24]. Although this study’s population and medications differ from our own, the basic premise of increased satisfaction with oral versus injected treatment holds. Furthermore, higher patient satisfaction is likely to lead to increased treatment compliance, as reported by the authors of the EINSTEIN-PE trial. This is in keeping with our data. Despite the increased treatment course, only 2/48 (4.2%) patients in the oral aspirin group reported missing a medication dose, for a total of 7/4023 (0.17%) of doses. This is in comparison to 8/48 (16.7%) patients in the injected cohort, for a total of 25/762 (3.72%) of doses.
We acknowledge the inherent limitations to our investigation. The most apparent of these is the nature of a self-reported questionnaire- based design. Recall bias may exist with regard to the perceived satisfaction or efficacy of treatment, as well as compliance to treatment in terms of missed medication doses. Furthermore, our limited 6-week follow up may not be reflective of true shortterm efficacy or complication rates with anticoagulant treatment. Complication rates and treatment efficacy, however, were not the focus of this study. Nonetheless, in a study of post-operative total joint patients on active warfarin therapy, Parvizi et al. determined that out of 283 documented symptomatic PE cases, 81% occurred within three postoperative days, 89% within one postoperative week, and 94% within two postoperative weeks [25]. Active VTE prophylaxis is therefore most crucial during the first two weeks post-operatively, although the timing of other complications is less well studied. Lastly, our study reflects the opinions and practices of patients and senior surgeons of a single institution, which may not be in conjunction with those of a larger multi- centered population. Specific patient profiles and conditions, laboratory data, and transfusion requirements were not addressed in this study and may be areas of additional research.
There is much controversy regarding chemoprophylaxis after TKA. There is increasing evidence in the literature of the effectiveness and safety of aspirin-based treatment of DVT and PE in post-operative TKA patients. Our study addresses patient reported outcomes with regards to the use of aspirin, as compared to injectable chemoprophylaxis. We have demonstrated increased satisfaction and compliance with our oral aspirin regimen, as compared to traditional injected low-molecular weight heparin. We thereby conclude that aspirin prophylaxis should be strongly considered in the low-risk post-operative total joint patient. Further research is necessary to address long-term satisfaction outcomes in our study population.
References
- Comp PC, Spiro TE, Friedman RJ, Whitsett TL, Johnson GJ, et al. (2001) Prolonged enoxaparin therapy to prevent venous thromboembolism after primary hip or knee replacement. Enoxaparin Clinical Trial Group. J Bone Joint Surg Am 83(3): 336-345.
- Cusick LA, Beverland DE (2009) The incidence of fatal pulmonary embolism after primary hip and knee replacement in a consecutive series of 4253 patients. J Bone Joint Surg Br 91(5): 645-648.
- Cordell-Smith JA, Williams SC, Harper WM, Gregg PJ (2004) Lower limb arthroplasty complicated by deep venous thrombosis. Prevalence and subjective outcome. J Bone Joint Surg Br 86(1): 99-101.
- Bookenthal KR, Freedman KB, Lotke PA, Fitzgerald RH, Lonner JH (2001) A meta-analysis of thromboembolic prophylaxis in total knee arthroplasty. J Arthroplasty 16(3): 293-300.
- Douketis JD, Eikelboom JW, Quinlan DJ, Willan AR, Crowther MA (2002) Short duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of prospective studies investigating symptomatic outcomes. Arch Intern Med 162(13): 1465-1471.
- Freedman KB, Brookenthal KR, Fitzgerald RH Jr, Williams S, Lonner JH (2000) A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 82(7): 929-938.
- Larson CM, MacMillan DP, Lachiewicz PF (2001) Thromboembolism after total knee arthroplasty: intermittent pneumatic compression and aspirin prophylaxis. J South Orthop Assoc 10(3): 155-163.
- Sharrock NE, Gonzalez Della Valle A, Go G, Lyman S, Salvati EA (2008) Potent anticoagulants are associated with a higher all cause mortality after hip and knee arthroplasty. Clin Orthop Relat Res 466(3): 714-721.
- Johanson NA, Lachiewicz PF, Lieberman JR, Lotke PA, Parvizi J, et al. (2009) American Academy of Orthopaedic Surgeons clinical practice guideline on prevention of symptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. J Bone Joint Surg Am 91(7): 1756-1757.
- Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, et al. (2012) Prevention of VTE in Orthopedic Surgery Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141(2 suppl):e278S-e325S.
- Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, et al. (2008) Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 133(6 suppl): 381S-453S.
- Catella-Lawson F, Reilly MP, Kapoor SC, Cucchiara AJ, DeMarco S, et al. (2001) Cyclooxygenase inhibitors and the antiplatelet effects of aspirin. N Engl J Med 345(25): 1809-1817.
- Patrono C, Coller B, FitzGerald GA, Hirsh J, Roth G (2004) Platelet-active drugs: the relationships among dose, effectiveness, and side effects: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 126(3 suppl): 234S-264S.
- Bozic KJ, Vail TP, Pekow PS, Maselli JH, Lindenauer PK (2010) Does aspirin have a role in venous thromboembolism prophylaxis in total knee arthroplasty patients? J Arthroplasty 25(7): 1053-1060.
- Jameson SS, Baker PN, Charman SC, Deehan DJ, Reed MR, et al. (2012) The effect of aspirin and low molecular weight heparin on venous thromboembolism after knee replacement: a non-randomized comparison using national joint registry data. J Bone Joint Surg Br 94(7): 914-918.
- Lotke PA, Lonner JH (2005) Deep venous thrombosis prophylaxis: better living through chemistry – in opposition. J Arthroplasty 20(4 Suppl 2): 15- 17.
- Lotke PA, Palevsky H, Keenan AM, Meranze S, Steinberg ME, et al. (1996) Aspirin and warfarin for thromboembolic disease after total joint arthroplasty. Clin Orthop Relat Res (324): 251-258.
- Raphael I, Tischler E, Huang R, Rothman R, Hozack W, et al. (2014) Aspirin: An Alternative for Pulmonary Embolism Prophylaxis After Arthroplasty? Clin Orthop Relat Res 472(2): 482-488.
- Vulcano E, Gesell M, Esposito A, Ma Y, Memtsoudis SG, et al. (2012) Aspirin for elective hip and knee arthroplasty: a multimodal thromboprophylaxis protocol. Int Orthop 36(10): 1995-2002.
- Berend KR, Lombardi AV Jr. (2006) Multimodal venous thromboembolic disease prevention for patients undergoing primary or revision total joint arthroplasty: the role of aspirin. Am J Orthop 35(1): 24-29.
- White RH, Meehan JP, Romano PS (2010) Re: Does aspirin have a role in venous thromboembolism prophylaxis in total knee arthroplasty patients? J Arthroplasty 25(4): 667.
- Pellegrini VD Jr, Sharrock NE, Paiement GD, Morris R, Warwick DJ (2008) Venous thromboembolic disease after total hip and knee arthroplasty: current perspectives in a regulated environment. Instr Course Lect 57: 637-661.
- Nam D, Nunley RM, Johnson SR, Keeney JA, Barrack RL (2015) Mobile Compression Devices and Aspirin for VTE Prophylaxis Following Simultaneous Bilateral Total Knee Arthroplasty. J Arthroplasty 30(3): 447-450.
- Prins MH, Bamber L, Cano SJ, Wang MY, Erkens P, et al. (2015) Patientreported treatment satisfaction with oral rivaroxaban versus standard therapy in the treatment of pulmonary embolism; results from the EINSTEIN PE trial. Thromb Res 135(2): 281-288.
- Parvizi J, Huang R, Raphael IJ, Maltenfort MG, Arnold WV, et al. (2015) Timing of Symptomatic Pulmonary Embolism with Warfarin Following Arthroplasty. J Arthroplasty 30(6): 1050-1053.
- www.nihpromis.org
- Hays RD, Bjorner JB, Revicki RA, Spritzer KL, Cella D (2009) Development of physical and mental health summary scores from the Patient Reported Outcomes Measurement Information System (PROMIS) global items. Qual Life Res 18(7): 873-880.
- Rothrock NE, Hays RD, Spritzer K, Yount SE, Riley W, et al. (2010) Relative to the general US population, chronic diseases are associated with poorer health-related quality of life as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS). J Clin Epidemiol 63(11): 1195-1204.
- Chung H, Kim J, Cook KF, Askew RL, Revicki DA, et al. (2014) Testing measurement invariance of the Patient-Reported Outcomes Measurement Information System pain behaviors score between the US general population sample and a sample of individuals with chronic pain. Qual Life Res 23(1): 239-244.
- Broderick JE, Schneider S, Junghaenel DU, Schwartz JE, Stone AA (2013) Validity and reliability of Patient-Reported Outcomes Measurement Information System instruments in osteoarthritis. Arthritis Care Res 65(10):1625-1633.





