Multifocal Dermatofibrosarcoma Protuberans
Weinstock M1, Berman R2, Sanfilippo N3, Myssiorek D1*
1 Department of Otolaryngology - Head and Neck Surgery.
2 Department of Surgical Oncology.
3 Department of Radiation Oncology, the Laura and Isaac Perlmutter Cancer Center of the NYU Langone Medical Center, New York, NY 10016, USA .
*Corresponding Author
David Myssiorek, MD, FACS,
NYU Clinical Cancer Center, 160 E34th Street, 7th Floor,
New York, NY 10016, USA.
Tel: (212) 731-6085
Fax: (212) 731-5520
E-mail: myss@optonline.net
Received: March 06, 2016; Accepted: March 23, 2016; Published: March 31, 2016
Citation: Weinstock M, Berman R, Sanfilippo N, Myssiorek D (2016) Multifocal Dermatofibrosarcoma Protuberans. Int J Clin Exp Otolaryngol. 2(1), 19-22. doi: dx.doi.org/10.19070/2572-732X-160003
Copyright: Myssiorek D© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Dermatofibrosarcoma Protuberans (DFSP) is an exceptionally rare soft tissue tumor that spreads locally with rare metastasis limited to brain, lung, and liver. Immunocompetent patients presenting with more than one DFSP are rare.
Methods and Results: A 47 year old man presented with metachronous lesions of the left mastoid skin and right supraclavicular fossa skin. Biopsies revealed DFSP in both locations. CT scans never showed bony invasion in either location. Multiple excisions and radiation therapy have resulted in no recurrence at the supraclavicular site and recurrence in the mastoid site.
Conclusions: DFSP can recur despite wide and deep excision combined with radiation therapy. The treatment algorithm for DFSP in the Head and Neck region is included in our review of the literature. Long term follow up is mandatory in these patients.
2.Introduction
3.Case History
4.Discussion
5.Conclusion
6.References
Keywords
Dermatofibrosarcoma Protuberans; Multifocal; Surgery; Radiation; Non Immunocompromised.
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a superficial sarcoma stemming from fibroblastic and myofibroblastic differentiation within the dermis and underlying soft tissue. It is a very rare tumor with less than 4.5 cases per million persons per year in the US [1]. Between 16 and 20% of the cases of DFSP may be associated with previous traumatic events ranging from mild ulcerations to bayonet stabbing [2]. Most cases of DFSP (47%) occur in the trunk region, however roughly 10% of cases can be found in the head and neck region and 8% in the shoulder region [3]. Metastasis is a rare occurrence, with a rate of roughly 2% over ten years, and usually occurs in the lung, brain, or bone.4 DFSP has the propensity to recur locally especially within the head and neck region where wide local excision is difficult to obtain without significant morbidity. Given the high risk of local recurrence adjuvant therapy in the form of radiation has grown in practice.
Cases of multicentric DFSP are exceptionally rare, with only a few case reports available in the literature. The following case report describes a patient who had concurrent lesions of DFSP of a multifocal nature, one possibly precipitated by trauma and the other with no apparent causative injury.
Case History
A 47 year old patient presented with simultaneous lesions of the left mastoid region and right shoulder. These lesions were subcutaneous and not tender. Roughly 20 years prior to presentation, he was struck in the back of the head with a baseball bat and subsequently developed a firm swelling over his left mastoid bone posteriorly. The lesion was removed 18 years after it initially appeared. The pathology of this specific lesion was reportedly benign. Surgical excision and pathological investigation were conducted at an outside hospital and no records were able to be obtained. In 2007, the patient was again struck in the back of the left skull during an altercation. A short time later he noted a 2 x 2 cm lesion immediately medial to the scar from the prior surgical resection of the original lesion. This lesion was resected at another hospital and found to be DFSP with multiple positive margins.
The patient was did not seek any intervention for the next two years. He then presented with a vertical scar over the occipital region of his left skull, lateral to which there was a circular quarter size depression (Figure 1). Lateral to this depression there was a ridge of firm tissue. The patient underwent another resection and DFSP was found. The margins were considered negative but close in March, 2009. The patient returned for a re-excision of the tumor this time with margins negative for disease in June, 2009.
The patient then presented for the evaluation of an unrelated mass located in his right supraclavicular subcutaneous space. He stated that he had been aware of the supraclavicular mass for roughly seven years but had never had it evaluated. The patient underwent a biopsy of the lesion in the office that confirmed the supraclavicular lesion to be DFSP as well. CT scan showed no bony invasion or local extension. The patient underwent excision of the mass located in the right supraclavicular fossa that had been confirmed as DFSP in November, 2011 (Figure 1 and 2). All margins were negative.
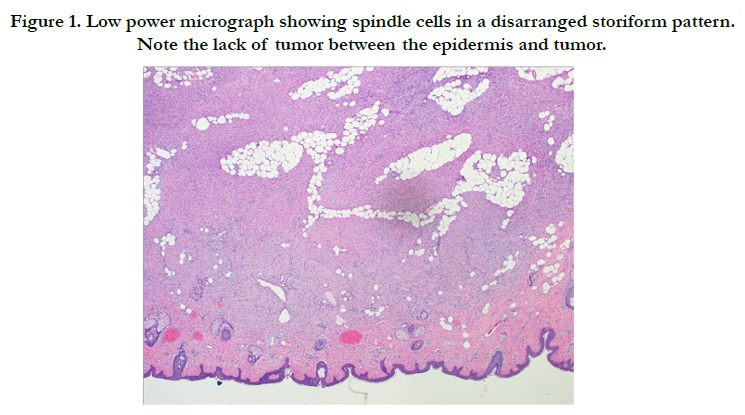
Figure 1. Low power micrograph showing spindle cells in a disarranged storiform pattern. Note the lack of tumor between the epidermis and tumor.
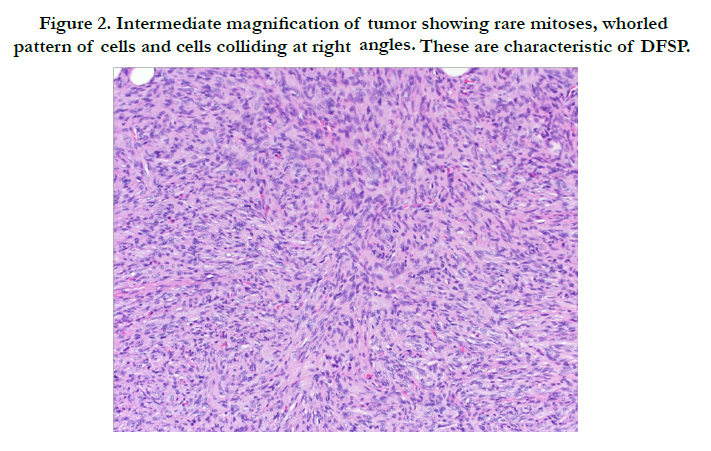
Figure 2. Intermediate magnification of tumor showing rare mitoses, whorled pattern of cells and cells colliding at right angles. These are characteristic of DFSP.
The distance between the mass in the right supraclavicular fossa and the left occipital region of the skull was at least 10 cm; given the negative margins and lack of gross tumor in between these two pathologically confirmed DFSP tumors, it was inferred that these two tumors were concurrently growing and originated from different foci.
The patient subsequently underwent external beam radiation to both sites from 1/5/12 through 2/27/12. He received a total of 5940 cGy to both regions. The patient once again presented with a 0.5 x 0.5 cm pink raised area just lateral to the distal/ inferior edge of the supraclavicular wound. MRI showed a region of iso-intensity on T1 and T2 with an enhancing signal within subcutaneous tissue along the anterior margin of the trapezius just proximal to its clavicular insertion measuring approximately 3.5 x 0.9 x 0.3 cm. This mass was excised shortly thereafter and found to be recurrent DFSP with wide local margins of 2 to 3 cm negative for disease. At the time of excision the patient noted some firm changes to the scar on the back of his left neck. An excision and biopsy were taken two months later; this was found to be traumatic neuroma and not DFSP.
Three months later the patient presented with right sided headache. The right occipital scalp revealed a nondiscreet mass, not fixed to the skull that was flat and 25mm by 25mm. It was nontender but associated with pain. The left excision site had no masses. The right shoulder was free of subdermal masses. FNA confirmed this mass to be of a benign nature. At one year since the last treatment, the patient remains without evidence of recurrence at the shoulder site. 3 years following completion of radiation at the left mastoid site, a recurrence was noted and resected to negative margins. At no time have distant metastasis been detected.
Discussion
A literature search revealed four cases of multicentric DFSP in immunocompetent patients. One case involved a 59 year old man with a 6 year history of concurrently growing dermal lesions, one located in his left abdomen and the other on his right mandible. These lesions were confirmed to be DFSP on biopsy. No evidence of metastatic disease was seen in the lungs or brain.
A second case of multifocal DFSP was reported by Rademaker et al and was seen in a 35 year old patient with a previous scalp lesion of DFSP since the age of 10, status post 15 excisions and two courses of radiation who presented with a 10 x 7 cm plaque like thickening that had two nodules, found to be multi-centric DFSP. Eight years later he had a wedge resection of the middle lobe of his right lung for metastasis of DFSP, and was recurrence free at 18 months follow up [5]. It is somewhat unclear whether these two nodules represent discrete masses or were from the same original tumor.
The last two cases of multifocal DFSP were reported by Pack et al. One patient was reported to have DFSP with a second nodule 13 cm away, however a lack of excision or biopsy of the second nodule leaves the authenticity of the multifocal nature of this occurrence in question. The final patient had multiple lesions within 10 cm of each other; however the skin between these lesions was not biopsied so it is unclear whether it could be from local migration or of multicentric origin [6].
A number of patients with Adenosine Deaminase–Deficient Severe Combined Immunodeficiency (ADA-SCID) were found to have DFSP of multicentric origins. In a study looking at 12 patients with ADA-SCID, seven were found to have multifocal DFSP; the patients ranged in age from 2-22 years old. A combined pathogenesis explaining the concurrence of these two rare diseases has not been fully illuminated, but is not likely secondary to viral infection from the Herpes virus or other viral etiologies [7].
A recent analysis of the SEER database by Kurlander et al., revealed an increased risk of subsequent primary malignancy (SPM) in patients with primary DFSP [8]. Male patients with DFSP were found to have a 25% increased risk of developing an SPM, with a 21-fold increased risk of non epithelial skin cancers, many of which were DFSP. Female patients were found to be at an increased risk of melanoma (2.58 fold increased risk) and breast cancer (1.44 fold increased risk). Patients of both sexes are also at an increased risk developing soft tissue sarcomas (5 fold increase), of which DFSP is also classified. Our male patient should undergo thorough dermatologic screening for de novo DFSP lesions every three to six months as his risk of developing a third malignancy is increased. Female patients can consider increased screening for breast malignancies, melanoma, and soft tissue, although the data is less conclusive for this recommendation [8].
A common finding in DFSP is the presence of supernumerary ring chromosomes or a translocation between chromosomes 17 and 22 (t 17;22) (22;q13): over 90% of DFSP tumors possess this characteristic, resulting in a hyperexpression of collagen type 1 alpha 1 (COL1A1) gene on chromosome 17 with platelet-derived growth factor B–Chain gene (PDFGB), a growth factor for connective tissue cells. PDGFB production results in constant generation and proliferation of tumor cells [9]. PDGFB has been implicated in malignancies for which patients with a primary diagnosis of DFSP are at a high risk of developing subsequent to their initial diagnosis, such as melanoma [10, 11], breast cancer [12], and soft tissue cancer [13].
The locally aggressive nature of DFSP has led many to suggest wide local excision with between 2.5 and 3.5 cm as the mainstay of therapy. Local recurrence rates have dropped to reports of 0-5% with wide local excision [14, 4] compared to an average of 39.7% with undefined or conservative surgical margins [15]. Radiation therapy has become more popular as a form of adjuvant therapy for DFSP especially when the tumor is located in the head and neck region where wide local excision with 3 cm margins may be impossible without significant morbidity. Local control rates for secondary recurrence after surgery vs. surgery with radiation therapy was 28% vs. 80%, respectively [16]. In a retrospective analysis of 53 patients treated with surgery and either preoperative or postoperative radiation therapy, Castle et al found local control of 98% and 93% at 5 and 10 years respectively when using radiation doses of roughly 50 Gy preoperatively or 60 Gy postoperatively [17]. The recommended dose of radiation therapy ranges from 50 Gy (palliative), to 60 Gy (microscopic tumor) and 70 Gy (macroscopic tumor) in conventional fractions [18]. Radiation therapy should be considered in patients with DFSP of the head and neck where wide local excision may not be attainable.
Conclusion
Dermatofibrosarcoma protuberans is a rare sarcoma of skin and underlying soft tissue. It is rarer to have two lesions occurring in one individual. The lesions should be treated as one would treat a single occurrence. Radiation therapy given postoperatively improves the outcome of these patients but long term follow up for recurrence is mandatory. Patient self-reporting is valuable with this disease.
- Multifocal DFSP is rare.
- When present, it is more likely to be found in immunocompromised hosts.
- Reverse transcriptase polymerase chain reaction (RT-PCR) and fluorescence in situ hybridization (FISH) should be used as screening tools for the presence of the COL1A1-PDGFB fusion gene.
- Treatment should include wide surgical excision with at least two cm margins.
- DFSP is a radioresponsive tumor.
- Common indications for adjuvant radiation are microscopically close or positive margins or after resection of recurrent tumors.
- Total radiation doses of approximately 60 Gy over 6-7 weeks should be prescribed for microscopic disease.
- While surgery is the primary treatment, conservative resection and postoperative radiation should be considered for situations where wide excision alone would result in major cosmetic or functional deficit.
- Imatinib (Gleevec) has shown promise in patients with this fusion gene and may be initiated as adjuvant therapy.
- DFSP tumors lacking the classic t (17, 22) translocation mutation seem to respond poorly to imatinib.
References
- Rouhani P, Fletcher CD, Devesa SS, Toro JR (2008) Cutaneous soft tissue sarcoma incidence patterns in the U.S.: An analysis of 12,114 cases. Cancer 113(3): 616-627.
- Taylor HB, Helwig EB (1962) Dermatofibrosarcoma protuberans. A study of 115 cases. Cancer 15: 717-725.
- Gloster HM Jr (1996) Dermatofibrosarcoma protuberans. J Am Acad Dermatol 35(3 Pt 1): 355-376.
- Fiore M, Miceli R, Mussi C, Lo Vullo S, Mariani L, et al. (2005) Dermatofibrosarcoma protuberans treated at a single institution: a surgical disease with a high cure rate. J Clin Oncol 23(30): 7669-7675.
- Rademaker B, Angelillo M, Reiman HM, Jackson IT (1990) Dermatofibrosarcoma protuberans: a review of 73 cases. Eur J Plast Surg 13: 251-255.
- Pack GT, Tabah EJ (1951) Dermatofibrosarcoma protuberans: A report of thirty-nine cases. AMA Arch Surg 62(3): 391-411.
- Kesserwan C, Sokolic R, Cowen EW, Garabedian E, Heselmeyer-Haddad K, et al. (2012) Multicentric dermatofibrosarcoma protuberans in patientswith adenosine deaminase–deficient severe combined immune deficiency. JAllergy Clin Immunol 129(3): 762-769.
- Kurlander DE, Martires KJ, Chen Y, Barnholtz-Sloan JS, Bordeaux JS (2013) Risk of subsequent primary malignancies after dermatofibrosarcoma protuberans diagnosis: A national study. J Am Acad Dermatol 68(5): 790-796.
- Patel KU, Szabo SS, Hernandez VS, Preito VG, Abruzzo LV, et al. (2008) Dermatofibrosarcoma protuberans COL1A1-PDGFB fusion is identified in virtually all dermatofibrosarcoma protuberans cases when investigated by newly developed multiplex reverse transcription polymerase chain reaction and fluorescence in situ hybridization assays. Hum Pathol 39(2): 184-193.
- Wu NL, Chiang KYC, Huang CC, Fang JY, Chen DF, et al. (2010) Zeaxanthin inhibits PDGF-BB-induced migration in human dermal fibroblasts.Exp Dermatol 19(8): e173-181.
- Furuhashi M, Sjoblom T, Abramsson A, Ellingsen J, Micke P, Li H, et al. (2004) Platelet-derived growth factor production by B16 melanoma cells leads to increased pericyte abundance in tumors and an associated increase in tumor growth rate. Cancer Res 64(8): 2725-2733.
- Yokoyama Y, Mori S, Hamada Y, Hieda M, Kawaguchi N, et al. (2011) Platelet derived growth factor regulates breast cancer progression via β-Catenin expression. Pathobiology 78(5): 253-260.
- Palman C, Bowen-Pope DF, Brooks JJ (1992) Platelet-derived growth factor receptor (beta-subunit) immunoreactivity in soft tissue tumors. Lab Invest66(1): 108-115.
- Popov P, Bohling T, Asko-Seljavaara S, Tukiainen E (2007) Microscopic margins and results of surgery for dermatofibrosarcoma protuberans. Plast Reconstr Surg 119(6): 1779-1784.
- Lemm D, Mügge LO, Mentzel T, Höffken K (2009) Current treatment options in dermatofibrosarcoma protuberans. J Cancer Res Clin Oncol 135(5):653-665.
- Sun LM, Wang CJ, Huang CC, Leung SW, Chen HC, et al. (2000) Dermatofibrosarcoma protuberans: Treatment results in 35 cases. Radiother Oncol 57(2): 175-181.
- Castle KO, Guadagnolo BA, Tsai CJ, Feig BW, Zagars GK (2013) Dermatofibrosarcoma Protuberans: Long-term outcomes of 53 patients treated with conservative surgery and radiation therapy. Int J Radiat Oncol Biol Phys 86(3): 585-590.
- Ugurel S, Kortmann RD, Mohr P, Mentzel T, Garbe C, et al. (2008) Short German guidelines: dermatofibrosarcoma protuberans. J Dtsch Dermatol Ges 6(Suppl 1): S17-18.





