Multiple Myeloma: Concise Review of the Literature and A Case Report of Mandibular Involvement
Hong K1, Lim A1, Wong R1, Chan EH2, Islam I3*
1 Discipline of Oral and Maxillofacial Surgery, University Dental Cluster, National University Health System, Singapore.
2 Department of Haematology-Oncology, National University Cancer Institute, Singapore.
3 Discipline of Oral and Maxillofacial Surgery, Faculty of Dentistry, National University of Singapore, Singapore.
*Corresponding Author
Intekhab Islam,
Assistant Professor, Oral and Maxillofacial Surgery, National University of Singapore,
11 lower Kent Ridge Road, Singapore 119083.
Tel: +6567726748
Fax: +6567732600
E-mail: denii@nus.edu.sg
Received: July 05, 2016; Accepted: August 20, 2016; Published: August 23, 2016
Citation: Hong K, Lim A, Wong R, Chan EH, Islam I (2016) Multiple Myeloma: Concise Review of the Literature and A Case Report of Mandibular Involvement. Int J Dentistry Oral Sci. 3(8), 309-314.DOI : dx.doi.org/10.19070/2377-8075-1600062
Copyright: Islam I© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Multiple myeloma is an uncommon hematologic malignancy which is characterized by monoclonal proliferation of malignant plasma cells. The most common locations include the spine, skull, pelvis, ribs, humerus, femur and jaws. Jaw involvement usually present as secondary lesions. The prevalence of jaw involvement is up to 30%, more commonly involving the mandible. Diagnostic techniques used to evaluate patients with suspected multiple myeloma include bone marrow biopsy, blood tests, urinalysis and radiographic evaluation. For most patients, the preferred treatment option is for induction chemotherapy followed by autologous stem cell transplantation. Bisphosphonates are commonly used in the treatment of multiple myeloma as they inhibit bone resorption and exert anti-tumor activity. Patients are usually referred to the dental service for clearance prior to commencement of intravenous bisphosphonate therapy.
We present a case report which describes the incidental finding and subsequent management of a secondary lesion at the left mandible in a patient diagnosed with multiple myeloma during a routine dental examination. The necessity for dental clearance prior to bisphosphonate therapy makes it necessary to treat jaw lesions for Multiple Myelomas which were previously monitored and treated medically along with the Myeloma.
2.Introduction
3.Diagnosis of Multiple Myeloma
4.Prevalence and Clinical Presentation in the Jaw
5.Role of Bisphosphonates
6.Dental Clearance Prior To Intravenous Bisphosphonate
7.Case Report
8.Discussion
9.Ethics Declaration
10.References
Keywords
Multiple Myeloma; Medical Management; Mandible; Bisphosphonates.
Introduction
Multiple myeloma is an uncommon hematologic malignancy which makes up 1% of all cancers and slightly over 10% of all hematologic malignancies [1]. It occurs in adults and is rarely diagnosed before 40 years old [2]. The median age is 66 years [3]. It is characterized by the monoclonal proliferation of malignant plasma cells which produce excessive amounts of abnormal monoclonal immunoglobulins leading on to end organ damage or more commonly known as the CRAB features [3].
Although many etiologic factors have been described, including infectious agents like human herpes virus 8 (HSV-8), exposure to chronic low-dose ionizing radiation and industrial exposure to insecticides, there is no clear etiology for multiple myeloma [2].
The malignant plasma cell proliferation in the bone marrow results in reduced normal trilineage haematopoiesis, which in turn results in anemia and increased fatigue. Although severe thrombocytopenia and neutropenia are not common at first presentation, thrombocytopenia if present increases the risk of bleeding, while neutropenia with co-exisiting immune paresis result in an increased risk of serious infections [4].
Bone involvement is the most common complication in multiple myeloma and is seen in up to 90% of cases. Pain is most commonly reported in the chest or back and is caused by lytic bone lesions [3]. The bone loss and erosions also cause osteopenia or osteoporosis which can lead to pathological fracture in bones such as the vertebrae, ribs and pelvis. Hypercalcemia usually occurs in active disease and results from the destruction of bone by lytic lesions and subsequent release of calcium into the bloodstream. This is seen in approximately 15-30% of myeloma patients [5].
Diagnosis of Multiple Myeloma
Diagnostic techniques used to evaluate patients with suspected multiple myeloma include bone marrow biopsy, blood tests, urinalysis and radiographic evaluation. The criteria used to diagnose multiple myeloma have just recently been updated by the International Myeloma Working Group [5].
A bone marrow biopsy would show interstitial clusters, focal nodules or diffuse sheets of abnormal myeloma plasma cells. As the disease progresses, diffuse involvement of the expansive areas of the bone marrow occur with consequent suppression of haematopoiesis. Bone marrow aspirates typically have a pleomorphic appearance with normal, immature and plasmablastic myeloma plasma cells [6].
Due to the deposits of the malignant plasma cells, radiolucent lesions are present within bone. These lytic lesions may present as well-defined ‘punched out’ radiolucencies or ragged ill-defined radiolucencies.
The most common locations are namely: spine (50%), skull (35%), pelvis (34%), ribs (33%), humerus (22%), femur (13%) and mandible (10%). Witt et al., (1997) [7] found that 46.7% of patients presented with skull lesions, similar to a study by Ludwig et al. (1982) [8] which found 45% prevalence for skull involvement. Scutellari et al., (1993) noted that in 30% of patients, skeletal radiographic abnormalities may not be seen in the early stage of the disease [9].
Additional forms of imaging such as CT, MRI, PET-CT may be useful for patients without abnormality on plain radiographs, patients with unknown extent of disease, patients with bone pain and patients with neurological deficit with suspicion of spinal cord compression [5].
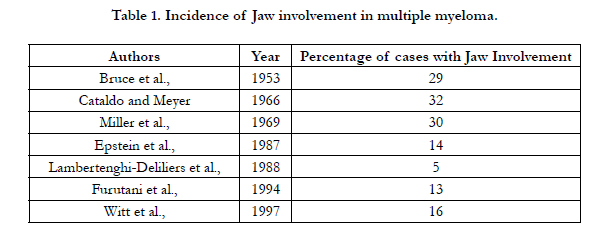

Table 1. Incidence of Jaw involvement in multiple myeloma.
Prevalence and Clinical Presentation in the Jaw
Multiple bone involvement in multiple myelomas are common and the most common clinical signs are swelling and pain. Radiographically they may present as generalized osteoporosis as well as multiple punched out lesions involving multiple bones [10]. Jaw involvement may be present in patients with multiple myeloma, usually as secondary lesions. Prevalence of jaw involvement is up to 30% in the literature.
Bruce et al., (1953) examined 59 patients with multiple myeloma and found jaw involvement in 17 patients [11]. Among the 17 patients with jaw involvement, the mandible was involved in 16 patients and maxilla was only involved in 4 patients while both jaws were involved in three patients. Cataldo and Meyer reported 32% of 44 patients had oral signs or symptoms [12]. Similarly, Miller et al., (1969) reported that prevalence of jaw involvement was 30%, with the mandible more commonly involved [13].
Epstein et al., (1984) reported a mean prevalence of 14% after evaluating 783 patients in the literature Mandibular lesions were commonly observed whereas maxillary lesions were rare. They summarized that the most commonly noted oral symptoms are pain, soft tissue swelling, mobility of teeth, amyloid deposition and radiolucent bony lesions. Oral signs and symptoms may be the initial presentation [14].
In a study by Lambertenghi-Deliliers et al., (1988), 10 out of 193 patients who were diagnosed with multiple myeloma developed osteolytic alterations of the mandible [15]. In all 10 patients with mandibular involvement, the maxilla was not involved. Prevalence of mandibular involvement was 5% the study.
Furutani et al., (1994) reported jaw involvement in 5 out of 38 patients with multiple myeloma, giving rise to prevalence of 13% [16]. Similar to the study by Lambertenghi-Deliliers et al., (1988), there was no maxillary involvement [15].
Witt et al., (1997) found a prevalence of 16% of mandibular involvement in a group of 77 patients with multiple myeloma [7]. Varying degrees of bone destruction were present. According to the study, radiographic lesions at the mandible were classified into 3 categories: 1) multilocular radiolucency; 2) unilocular radiolucency with a cyst like appearance; 3) ill-defined lesion with destructive bone resorption. Witt et al., (1997) found that the most common presentation was that of multiple lytic radiolucent lesions occurring at the posterior mandible [7]. All patients who presented with mandibular lesions also presented with skull lesions. Primary involvement of the mandible was not seen for all 77 cases.
Bruce et al., (1953) reported that multiple myeloma lesions usually present as multiple rounded radiolucent lesions with hazy, ill-defined margins with little osteosclerosis [11]. Other authors reported radiographic presentation as ‘punched out’ osteolytic lesions which may be single or multiple [14-16]. Root resorption may sometimes be observed [14].
Clinical presentation of multiple myeloma in the oral cavity may be varied (Table 2) and sometimes resemble dental or oral infection. It can range from small gingival masses to maxillary or mandibular cortical expansion with facial asymmetry. Although rare, patients may present with paraesthesia in cases of nerve compression. Paraesthesia of the lower lip and chin may be due to involvement of the inferior alveolar nerve [14, 17, 18].
Other forms of oral presentation may be due to light-chain associated amyloidosis, which is a complication of multiple myeloma. The oral lesion may present as a papule/nodule on the oral mucosa or even macroglossia due to deposition of amyloid [19].
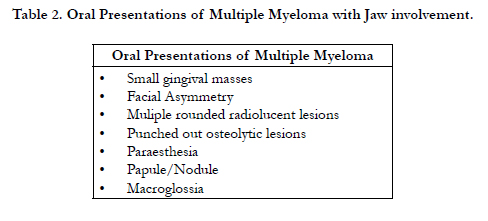
Table 2. Oral Presentations of Multiple Myeloma with Jaw involvement.
Role of Bisphosphonates
Bisphosphonates are synthetic analogues to inorganic pyrophosphates found within bone. They cannot be hydrolyzed by blood phosphatases. They inhibit osteoclastic activity and reduce bone resorption. The actions of bisphosphonates are long lasting and are thought to remain in bone for at least 10 years [20].
Besides inhibiting bone resorption, bisphosphonates may affect the microenvironment in which tumor cells grow and exert antitumor activity [21]. The UK Medical Research Council Myeloma IX trial randomized patients to zoledronic acid or clodronate and reported an increase in overall survival, reduction in skeletal related events and an improvement in progression free survival for patients who were given zoledronic acid. Thus, intravenous bisphosphonates is currently recommended for all multiple myeloma patients with active disease requiring therapy [22].
Dental Clearance Prior To Intravenous Bisphosphonate
In view of risk of bisphosphonate related osteonecrosis of the jaw, it is recommended by the American Association of Oral and Maxillofacial Surgeons that prior to treatment with intravenous bisphosphonates, the patient should have a thorough oral examination. A proper examination should include both detailed clinical and radiographic examination. Any unsalvageable teeth should be removed, all invasive dental procedures should be completed and optimal periodontal health should be achieved before the start of bisphosphonate therapy [23].
At present, patients are usually referred to the dental service for clearance prior to commencement of intravenous bisphosphonate therapy. The following case report describes the incidental finding of a secondary lesion at the left mandible during a routine oral examination in a patient diagnosed with multiple myeloma.
Case Report
Patient was a 60 year old Chinese male who was referred by the hematologist for dental clearance prior to use of intravenous zoledronic acid. (Zometa, Novartis Pharmaceuticals Corporation, USA).
Patient had recently undergone a bone marrow biopsy and was diagnosed with multiple myeloma (IgG type). Staging was done using the International Staging System [24] and was classified as Stage II. Genetic tests using fluorescence in situ hybridization (FISH) did not detect any abnormalities.
Bony metastasis was present at time of diagnosis of the disease. A full radiographic skeletal survey showed multiple bony lesions at the ribs, skull, humerus, femur and pubic rami. CT thorax showed extensive destructive bony lesions at the ribs and clavicle. Pathological fracture of the left clavicle was reported. MRI which was done for the spine reported tumor involvement of the entire spine and right hemisacrum. Other co-morbidities included type II diabetes mellitus, hypertension, hyperlipidemia and Hepatitis C. Patient was first seen by a general dentist for consult. He presented with a periodontally stable dentition. There was an incidental finding of a fluctuant mucosal colored swelling at the left posterior mandible in the region distal to tooth #34. The lower border of mandible was intact on palpation. No lower lip or chin paresthesia was present. A panoramic radiograph indicated a radiolucent lesion which was associated with impacted tooth #35 and a separate radiolucent lesion distal to it. The root of #35 appears resorbed in the dental panoramic radiograph (Figure 1).
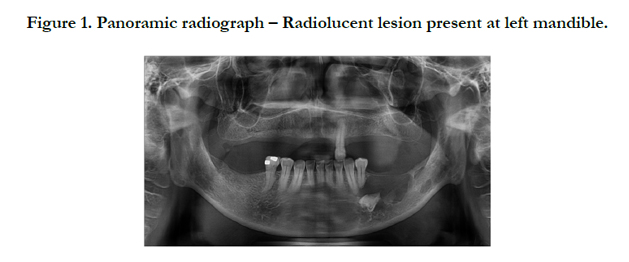
Figure 1. Panoramic radiograph – Radiolucent lesion present at left mandible.
The patient was subsequent referred by the general dentist to the oral and maxillofacial surgery service for further management. A cone beam CT was taken and indicated a radiolucent lesion present at the left posterior mandible with no distinct bony separation between the anterior and posterior lesion (Figure 2). The radiolucent lesion had a thin sclerotic border and was associated with impacted #35. The lingual plate in the region of the lesion was intact, but buccal plate was perforated.
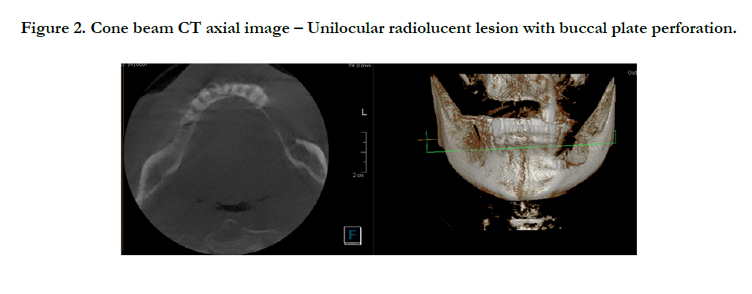
Figure 2. Cone beam CT axial image – Unilocular radiolucent lesion with buccal plate perforation.
Differential diagnoses included odontogenic cyst, odontogenic tumor and multiple myeloma. As the patient was not keen on incisional biopsy or any general anaesthesia procedures, the patient opted for local anaesthetic enucleation (excisional biopsy) of the lesion with removal of associated impacted tooth #35.
The patient’s fitness for surgery was verified with the referring hematologist prior to surgery. The local anaesthetic enucleation of the lesion with excision of impacted tooth #35 was performed 2 weeks after the initial dental consult. The patient was counselled on risks of infection and excessive blood loss in view of existing hematologic irregularities. The patient was also warned of risk of pathological fracture of the mandible in view of existing osteoporotic state.
A crevicular trapezoidal mucoperiosteal flap was raised at the left posterior mandible to expose the lesion. Perforation of the buccal plate was noted. On inspection, the lesion appeared fibrous and lobulated. No obvious aspirate was noted. The inferior alveolar nerve passed through the centre of the lesion. It was dissected free and preserved intact (Figure 3). The lesion was enucleated in whole together with excision of associated impacted tooth #35.
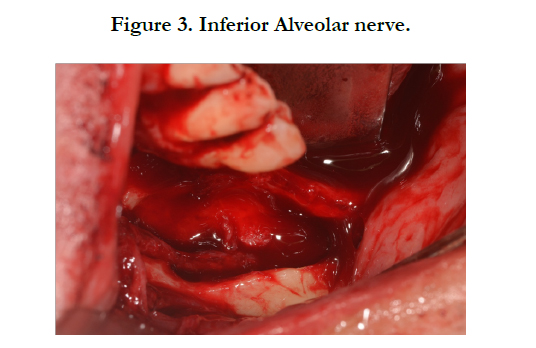
Figure 3. Inferior Alveolar nerve.
The lesion was sent for histopathological study. A small 4mm perforation of the lingual plate was noted after enucleation of the lesion. The periosteum of the mucoperiosteal flap which corresponded with the area of buccal bone perforation was excised. Peripheral bone ostectomy and chemical cauterization with Carnoy solution was done to reduce risk of recurrence in view of possibility of odontogenic cyst or tumor [25].
Any active bleeding was arrested with electrocautery before wound closure. BIPP (Bismuth Iodoform Paraffin Paste) pack was placed in the bony cavity to reduce risk of infection. Closure was done with resorbable 4/0 polyglactin sutures (Vicryl, Ethicon Inc, USA) and the BIPP pack was secured to the adjacent tooth #34 with 4/0 black silk sutures (Mersilk, Ethicon Inc, USA).
The patient tolerated the procedure well and vital signs of the patient were monitored in the clinic’s recovery room post operatively. The patient was discharged well on the same day of the surgery. The patient was kept on oral Augmentin (GlaxoSmithKline, UK) 625mg twice daily for 2 weeks. Analgesics and antibacterial mouthwash were also prescribed. The patient was advised to keep to soft diet for 4 weeks to reduce risk of pathological fracture.
The histological sample was examined by an oral maxillofacial pathologist and confirmed diagnosis of multiple myeloma. The recovery of the bony cavity was uneventful and patient was kept on regular reviews for replacement of BIPP pack every 2 weeks until the bony cavity shrank in size. Use of BIPP pack was discontinued 8 weeks after surgery. The patient was taught on selfcare of the bony cavity through use of an irrigation syringe. In the immediate post-operative period, patient reported moderate paraesthesia of his lower left lip and chin. At the 8week review, the cavity was filled with mucosa and only mild paraesthesia was reported (Figure 4).

Figure 4. Bony cavity healed, completely covered by mucosa.
Chemotherapy was started by the medical oncologist 3 weeks after the surgical enucleation of the mandibular lesion. The 4 cycle VCD regimen was used, which included use of Bortezomib (Velcade), Cyclophosphamide and Dexamethasone. Radiotherapy was not indicated. The first dose of intravenous zoledronic acid (Zometa, Novartis Pharmaceuticals Corporation, USA) was also given 12 weeks after the start of the VCD. The patient is currently planned for mobilization chemotherapy and subsequent autologous stem cell transplant (ASCT).
Discussion
Bisphosphonates are also commonly used for prevention of new bony lesions and are recommended for multiple myeloma patients who present with lytic lesions on radiographs or patients with osteopenia or osteoporosis as a result of the disease process [26]. The use of bisphosphonates leads to reduced complications such as skeletal fractures and bone pain [27]. Most patients are now referred for dental clearance prior to initiation of intravenous bisphosphonates.
The patient was first referred to the dental service for dental clearance prior to initiation of intravenous zoledronic acid. (Zo-meta, Novartis Pharmaceuticals Corporation, USA). The patient presented with incidental finding of a fluctuant mucosal colored swelling at the left posterior mandible in the region distal to tooth #34. The panoramic radiograph indicated a radiolucent lesion which was associated with impacted tooth #35 with a separate radiolucent lesion distal to it. A subsequent cone beam CT scan taken indicated a uni-locular radiolucent lesion with a thin sclerotic margin.
A full radiographic skeletal survey done pre-operatively showed multiple bony lesions at the ribs, skull, humerus, femur and pubic rami. CT scan of the thorax showed extensive destructive bony lesions at the ribs and clavicle. Pathological fracture of the left clavicle was also reported. The findings are consistent with the literature where multiple sites of bony involvement are present [9]. Pathological fracture of the left clavicle was likely due to an osteoporotic state as a result of the disease process.
Differential diagnoses for the jaw lesion included primary odontogenic cyst/tumor such as keratocystic odontogenic tumour or ameloblastoma. Another possible differential diagnosis was multiple myeloma. As there were no prior radiographs for comparison, it was impossible to know if the lesion was a primary lesion or a secondary lesion of the mandible. If the lesion was a multiple myeloma lesion, it was most likely due to secondary involvement of the mandible [7, 15, 16].
An incisional biopsy for the patient would have been beneficial to diagnose the lesion, but the patient was only keen on one surgical procedure. Fine needle aspiration biopsy could have been used, but may not be fully conclusive as well [17]. The lesion was closely associated with impacted tooth #35, causing root resorption. In view of possibility of the lesion being odontogenic in nature, we elected on enucleation of the lesion with peripheral ostectomy and chemical cauterization with Carnoy solution in accordance with protocol by [25]. The surgery was done under local anaesthesia and not general anaesthesia in view of multiple pre-existing co-morbidities.
The patient was counselled on the risks of pathological fracture that may occur post-operatively in view of the osteoporotic state as exemplified by the existing pathological fracture at the left clavicle. Intra-operatively, it was noted that there was still sufficient mandibular bone inferior to the lesion and no inter-maxillary fixation was deemed necessary. Post-operatively, the patient was advised to keep to soft diet for 4 weeks to reduce risk of pathological fracture. A two week course of oral antibiotics (Augmentin, GlaxoSmithKline, UK) was given to reduce risk of post-operative infection.
There is currently no consensus in the literature for management of multiple myeloma lesions in the jaw. If it is a solitary primary lesion of the jaw without systemic involvement, surgical excision and/or radiotherapy could be an option [17]. The adverse effects of radiotherapy must however be considered.
With the advent of bisphosphonate use in the treatment of multiple myeloma, it is crucial to manage any jaw lesion prior to initiation of intravenous bisphosphonate.
Multiple myeloma is generally considered incurable and is characterized by frequent relapses. Long term detailed surveillance of the oral cavity is advisable in view of risks of metastasis of the tumor and possible oral complications arising from use of bisphosphonates [23].
Mandibular lesions are different from other bony lesions of the body as the mandible is constantly subjected to tensile and compressive stresses caused by mastication and/or para-functional habits. Surgical procedures done in patients with intravenous bisphosphonate use would pose risk of osteonecrosis of the jaw [23].
If it is a secondary multiple myeloma jaw lesion in the presence of multiple metastatic bony lesions, the authors propose surgical excision of the jaw lesion followed by medical therapy (chemotherapy, autologous hematopoietic cell transplantation and intravenous bisphosphonate).
There is currently no consensus in the literature for management of multiple myeloma lesions in the jaw. If it is a solitary primary lesion of the jaw without systemic involvement, surgical excision and/or radiotherapy could be an option [17]. The adverse effects of radiotherapy must however be considered.
The necessity for dental clearance prior to bisphosphonate therapy makes it necessary to treat jaw lesions for Multiple Myelomas which were previously monitored and treated medically along with the Myeloma and tighter protocols need to be formulated for the same.
Ethics Declaration
The authors confirm that this study has been conducted in full accordance with the World Medical Association Declaration of Helsinki and written consent was obtained from the patient for documentation and reporting of this case. As this was a retrospective case report, an Institutional Review Board approval was not required.
References
- Siegel, R.,Ma J, Zou Z, et al., (2014) Cancer statistics . CA Cancer J Clin. 64(1): 9-29.
- Neville BW,Damm DD,Allen CM,Bouquot JE (2009) Hematologic disorders: Oral and maxillofacial pathology. (3rd edn), Saunders-Elsevier, Philadelphia. 592-598.
- Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, et al., (2003) Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 78(1): 21-33.
- Stoopler ET, DT Vogl, and EA Stadtmauer (2007) Medical management update: multiple myeloma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 103(5): 599-609.
- Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, et al., (2014) International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 15(12): 538-48.
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, et al., (2008) WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. (4th edn), IARC Press, Lyon, France.439.
- Witt C, Borges AC, Klein K, et al., (1997) Radiographic manifestations of multiple myeloma in the mandible: a retrospective study of 77 patients. JOral Maxillofac Surg,. 55(5): 450-3. discussion 454-5.
- Ludwig H (1982) Multiples Myeloma : Diagnose, Klinik und Therapie. Springer Verlag NY, New York.
- Scutellari PN and C Orzincolo (1993) Bone disease in multiple myeloma. Analysis of 253 controlled cases, with reappraisal of diagnostic criteria and current imaging techniques. Radiol Med. 85(3): 235-46.
- Lee SH, Huang JJ, Pan WL, et al., (1996) Gingival mass as the primary manifestation of multiple myeloma: report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 82(1): 75-9.
- Bruce KW and RQ Royer (1953) Multiple myeloma occurring in the jaws; a study of 17 cases. Oral Surg Oral Med Oral Pathol. 6(6): 729-44.
- Cataldo E, and I Meyer (1966) Solitary and multiple plasma-cell tumors of the jaws and oral cavity. Oral Surg Oral Med Oral Pathol. 22(5): 628-39.
- Miller CD, RR Goltry and JH Shenasky (1969) Multiple myeloma involving the mandible. Report of a case. Oral Surg Oral Med Oral Pathol. 28(4): 603-9.
- Epstein JB, NJ Voss and P Stevenson-Moore (1984) Maxillofacial manifestations of multiple myeloma. An unusual case and review of the literature. Oral Surg Oral Med Oral Pathol 57(3): 267-71.
- Lambertenghi-Deliliers, G Bruno E, Cortelezzi A, et al., (1988) Incidence of jaw lesions in 193 patients with multiple myeloma. Oral Surg Oral Med Oral Pathol. 65(5): 533-7.
- Furutani M, M Ohnishi, and Y Tanaka (1994) Mandibular involvement in patients with multiple myeloma. J Oral Maxillofac Surg. 52(1): 23-5.
- Cardoso RC1, Gerngross PJ, Hofstede TM, Weber DM, Chambers MS (2014) The multiple oral presentations of multiple myeloma. Support Care Cancer. 22(1): 259-67.
- Baykul T, U Aydin, and OC MK (2004) Unusual combination of presenting features in multiple myeloma. Dentomaxillofac Radiol. 33(6): 413-9.
- Stoopler ET, TP Sollecito, and SY Chen (2003) Amyloid deposition in the oral cavity: a retrospective study and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 95(6): 674-80.
- Kimmel DB (2007) Mechanism of action, pharmacokinetic and pharmacodynamic profile, and clinical applications of nitrogen-containing bisphosphonates. J Dent Res, 86(11): 1022-33.
- Mundy GR and T Yoneda (1998) Bisphosphonates as anticancer drugs. N Engl J Med. 339(6): 398-400.
- Morgan GJ, Davies FE, Gregory WM, Cocks K, Bell SE, et al., (2010) First-line treatment with zoledronic acid as compared with clodronic acid in multiple myeloma (MRC Myeloma IX): a randomised controlled trial.Lancet. 376(9757): 1989-99.
- Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, et al., (2014) American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J Oral Maxillofac Surg. 72(10):1938-56.
- Greipp PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, et al., (2005) International staging system for multiple myeloma. J Clin Oncol.23(15):3412-20.
- Stoelinga PJ (2012) The management of aggressive cysts of the jaws. J Maxillofac Oral Surg. 11(1): 2-12.
- Berenson JR, Rosen LS, Howell A, Porter L, Coleman RE, et al., (2001) Zoledronic acid reduces skeletal-related events in patients with osteolytic metastases. Cancer. 91(7): 1191-200.
- Mhaskar R, Redzepovic J, Wheatley K, Clark OA, Miladinovic B, et al., (2012) Bisphosphonates in multiple myeloma: a network meta-analysis. Cochrane Database Syst Rev, 16(5): CD003188.





