Evaluating Dentine Hypersensitivity Severity in Nigerians using Cumulative Hypersensitivity Index
Dosumu EB1*, Bamishe CT2, Dosumu OO3, Ogunsuji OO4
1 Faculty of Dentistry, Department of Periodontology & Community Dentistry, College of Medicine, University of Ibadan, Nigeria.
2 Faculty of Dentistry, Department of Restorative Dentistry, College of Health Sciences, Obafemi Awolowo University, Nigeria.
3 Faculty of Dentistry, Department of Restorative Dentistry, College of Medicine, University of Ibadan, Nigeria.
4 Faculty of Dentistry, Department of Periodontology and Community Dentistry, College of Medicine, University of Ibadan, Nigeria.
*Corresponding Author
Elizabeth Bosede DOSUMU,
Faculty of Dentistry, Department of Periodontology & Community Dentistry,
College of Medicine, University of Ibadan, Nigeria.
E-mail: edosumu18jj@mail.com
Received: November 23, 2018; Accepted: January 09, 2019; Published: January 11, 2019
Citation:Dosumu EB, Bamishe CT, Dosumu OO, Ogunsuji OO. Evaluating Dentine Hypersensitivity Severity in Nigerians using Cumulative Hypersensitivity Index. Int J Dentistry Oral Sci. 2019;6(1):671-675. doi: dx.doi.org/10.19070/2377-8075-19000132
Copyright: Dosumu EB©2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim: This national survey aimed to evaluate the cumulative severity of dentine hypersensitivity (DH) in Nigerians.
Method: 1349 urban and rural Nigerian dwellers aged 18-35 years were studied within a six-month period. Self-administered questionnaire evaluated subject’s demography, settlement, and brushing technique. Schiff index Scores were collected and percentages calculated. Gingival recession (GR) was measured, Cumulative Hypersensitivity Index (CHI) Score and the highest Schiff Index Score were recorded per subject. Spearman correlation Coefficients (P-value) were used to assess the relationship between CHI Scores, Schiff Index percentages, and Schiff Index highest per subject.
Results: There was statistical significance between CHI, gender, tooth brushing technique and GR (P<0.001). Percentage highest CHI was 18.8% and Schiff score was 35.4%. 26.5% of the respondents had GR greater than 1mm and the overall mean GR was 1.00 ± 1.32. The overall mean Schiff score was 0.54 ± 0.88 while the overall mean CHI was 1.51 ± 2.95.
Conclusion: DH is severe in Nigerians and the relationship between this severity, gender and tooth brushing technique is strong. There is a need for the prevention and management of DH in Nigeria.
2.Abbreviations
3.Introduction
4.Materials and Methods
5.Result
6.Discussion
7.Clinical Relevance
7.1 Scientific rational for study
7.2 Principal Findings
7.3 Practical Implications
8.Conclusion
9.References
Keywords
Dentine Hypersensitivity; Cumulative Hypersensitivity Index.
Abbreviations
DH: Dentine Hypersensitivity; GR: Gingival Recession; CHI: Cumulative Hypersensitivity Index.
Introduction
Dentine hypersensitivity (DH) has initial symptoms of sharp pain of rapid onset which disappears once the stimulus is removed. The initiation and progression of dentine hypersensitivity are reported to be influenced by the characteristics of the teeth and periodontium with the oral environment and external influences [13]. The aggravating stimuli are tactile, thermal and chemical or osmotic [1, 10, 13, 18]. The pain of DH although uncomfortable, it is most often a temporary and sustainable problem (Fardal et al., 2002) [7] and occasionally the pain may become chronic persisting for months or years.
DH is currently defined as a condition that is characterized by short sharp pain arising from exposed denture in response to stimuli typically thermal, evaporative, tactile, osmotic or chemical and which cannot be ascribed to any other form of defect or disease [5]. A more recently internationally and widely used definition is that DH is characterized by distinctive short, sharp pain arising from exposed denture in response to various external stimuli which are typically thermal, evaporative, tactile, electrical, osmotic, or chemical which cannot be related to any other form of dental pathology, defect or disease [2, 5, 8]. DH is the major and most significant symptom of gingival recession which is predisposed by some tooth/teeth anatomical, (root prominence, frenal pull, dehiscence & fenestrations), iatrogenic (surgical & non-surgical periodontal therapy) and behavioral (excessive oral hygiene and plaque control habits) factors [6].
DH is reported to be of particular concern to patients and sub-sequently affect health related quality of life [9]. This makes the accurate diagnosis and measurement of the severity of DH very important for appropriate corresponding management. A large number of indices and methods for reporting DH are available (Holland et al., 1997) [11] and reports from most studies are not comparable [14].
The Cumulative Hypersensitivity Index (CHI) for dentine hypersensitivity severity was validated by Olley et al., 2013 [14] to indicate DH severity per subject which may help to investigate the prevalence, aetiology and management of this condition. Olley et al., used the existing diagnostic criteria of Schiff index (Schiff et al., 1994) [16] by combining the results from the teeth into an overall subject sextant score.
The CHI was used in this study to investigate the severity of DH in Nigerian subjects with a view to proposing the need for its prevention and or management.
Materials and Methods
Two examiners for each of the eight states from the six geopolitical regions of Nigeria were trained and calibrated in the use of the Schiff Index at designated dental centers in these states. Institutional ethical approval for the study was obtained and all participating subjects provided written consents prior to enrolling in the study. A total of 1,349 urban and rural dwellers were recruited into the study, they were consecutive adult patients aged 18-35years that presented for routine dental treatments at these designated dental centers.
The inclusion criteria are dentate 18-35 years old subjects in good general health that presented at the designated urban and rural dental centers for routine dental care and consented to participate in the study. The exclusion criteria are subjects that have oral pathology or who wear orthodontic appliances or had used topical analgesic in the preceding 24 hours or were on antibiotics and those who do not consent to participate in the study.
Self administered questionnaire was used to evaluate subjects’ demography, settlement and tooth brushing techniques. The degree of gingival recession was measured using a CPITN periodontal probe at the mid-buccal and mid-oral of each tooth.
0 ‘subject does not respond to air stimuli’
1 ‘subject responds to air stimuli but does not request discontinuation of stimuli’
2 ‘subject responds to air stimuli and requests discontinuation or moves from stimuli’
3 ‘subject responds to the air stimulis, considers stimulis to be painful and requests discontinuation or moves from stimulus’
Schiff Index scoring criteria (Schiff et al., 1994)[16].
The teeth were dried with compressed air and all teeth surface examined under normal dental surgery conditions with good lighting. Teeth surfaces that had been restored, traumatized or carious and third molars were excluded from the study. DH was assessed using evaporative stimuli by compressed air from a three in one tip of a dental syringe at 900 to the tooth surface at 1cm distance for 1 sec [12, 14-16]. The gloved finger was used to shield the adjacent tooth surfaces. The response to DH was recorded on every teeth surface using the Schiff Index scoring criteria.
The CHI score was calculated for each subject as the summation of the highest Schiff Index recorded on a tooth surface in each of the six oral sextants. A percentage score was also calculated as a proportion of all tooth surface (buccal, occlusal/ incisal and oral) for Schiff Index 1, 1 and above, 2, 2 and above and 3 per subject. The highest Schiff Index score was also obtained per subject for all tooth surfaces (buccal, occlusal, incisal and oral).
The overall data were recorded and descriptive analyses was done using the spearman correlation coefficient (P-Value) to assess the relationship between CHI Scores, Schiff Index percentages and Schiff Index highest score per subject.
Result
A total of 1,349 consecutive adult subjects aged 18-35 years were recruited from sixteen (one rural and one urban) dental centers located in eight states from the six geopolitical regions of Nigeria within a period of six months. The urban dwellers were 51.9% of the respondents while 48.1% were rural dwellers. A total of 43.9% (n=592) were male while 54.6% (n=737) were females and there was statistically significant association between gender and CHI. Four hundred and three (29.9%) used various motion of brushing technique, 24.8% (n=334) used the horizontal motion, 38.3% (n=517) used the vertical motion, 3.9% (n=53) used the circular motion while 1.6% (n=22) do not know their brushing technique.
There was statistically significant association between CHI and tooth brushing technique. The type of hand used in tooth brushing does not have statistically significant association with CHI, while 91.9% (n=1,240) right handed, 6-3% (n=85) were left – handed.
Three hundred and twenty-six (24.2%) of the subjects had gingival recession (GR) greater than 1mm, 28.5% (n=385) had GR of 1mm while 47.3% (n=638) had GR of 0mm and the overall mean GR was 1.00=1.32. There was statistically significant association between CHI and gingival recession. The overall mean Schiff Index score was 0.54+ 0.88 while the overall mean CHI score was 1.51 ± 2.95. All the result shown in Tables 1,2,3, & 4.
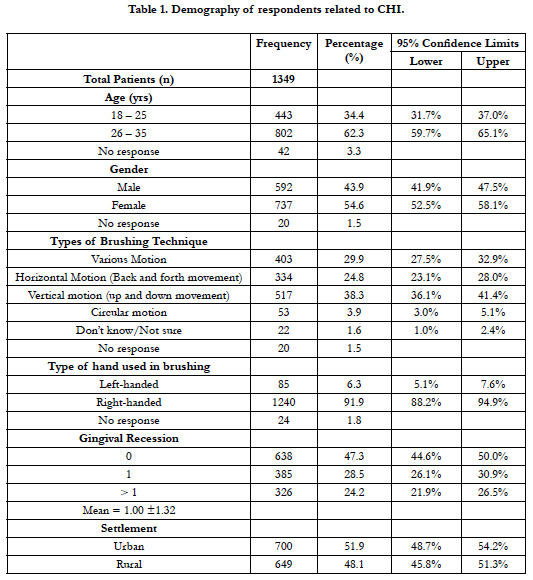

Table 1. Demography of respondents related to CHI.
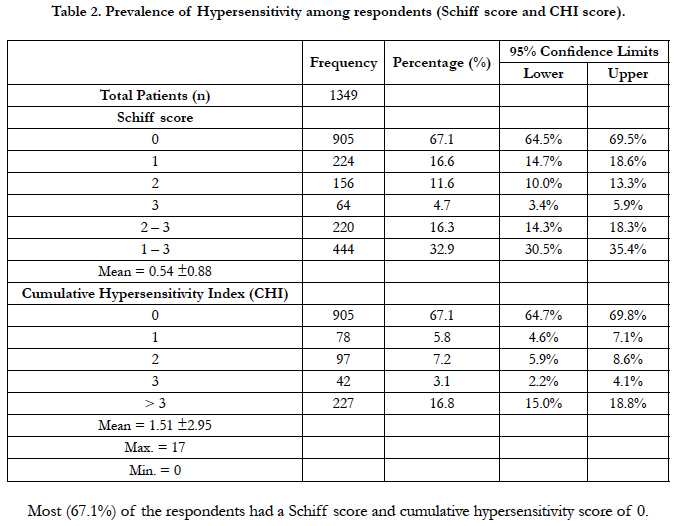
Table 2. Prevalence of Hypersensitivity among respondents (Schiff score and CHI score).
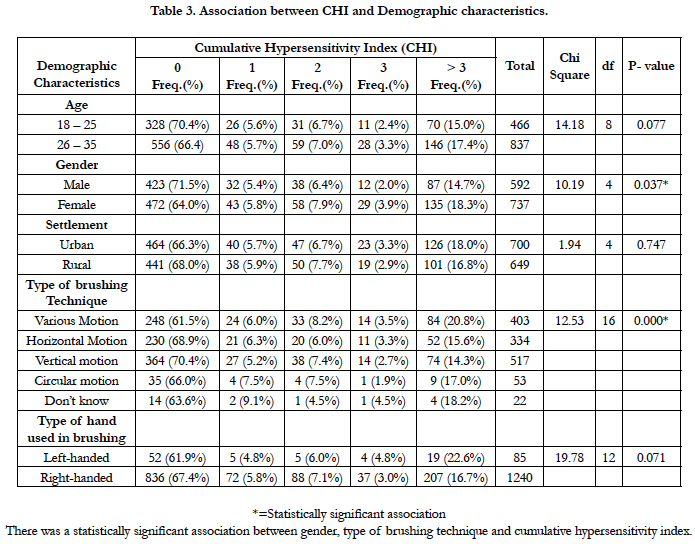
Table 3. Association between CHI and Demographic characteristics.
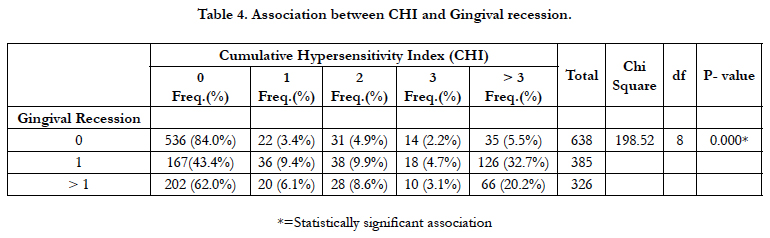
Table 4. Association between CHI and Gingival recession.
Discussion
This is a national survey which used the Schiff Index recorded as a cumulative sextant score per subject (or CHI Score) to assess the severity of denture hypersensitivity (DH) in Nigeria subjects. CHI score is reported to be a useful screening tool for the description of DH per subject. Although Olley et al., reported no significant association between CHI and gender, our finding in this study is contrary to this but it is in keeping with the findings of previous studies [5]. The difference in the study size may attribute for this variance in the findings.
This study showed a significant association between CHI and gingival recession (GR) which supports the report that a higher CHI score also indicated a higher risk of more gingival recession [14]. This study found 52.7% of the subjects to have varying degree of gingival recession which is just slightly higher than subjects who do not have GR and it is in keeping with other findings (Susin et al., 2004; Addy & West, 1994) [3, 17] although not as high.
In this study, there was a significant association between CHI and tooth brushing technique which may be consequent to gingival recession that is a sequel to improper tooth brushing technique with eventual dentine exposure and DH.
The overall mean CHI score was found to be 1.51+ 2.95 which is high indicating that DH is severe in this study subject. Since the study population spreads over all the six geopolitical regions of Nigeria, it may therefore imply that DH is severe in adult Nigerians.
On the contrary, the overall Schiff index score was 0.54 + 0.88 which is low and it may be because this index uses a semi-subjective judgment of a subject’s pain related behavior which is caused by an external stimulus and recorded by an observer.
The CHI score provides an indication of DH severity as well as providing possible guidance to clinical management.
Scientific rational for study
Dentine hypersensitivity is a clinical condition that leads to severe pain which affects the subject’s quality of life and it is a common finding in the Nigerian population. The Cumulative Hypersensitivity Index (CHI) for dentine hypersensitivity severity was used to indicate DH severity per subject which may help to investigate the prevalence, aetiology and management of this condition.
Principal Findings
There was statistical significance between CHI, gender, tooth brushing technique and GR (P<0.001).
Practical Implications
There is a need for the prevention and management of DH in Nigeria.
Conclusion
This national survey used a validated novel CHI score to indicate the severity of DH per subject in Nigerian adults. DH was found to be severe in Nigerians and the relationship between this severity, gender and tooth brushing technique is strong. There is therefore a dare need for the prevention and management of DH in Nigeria.
References
- Addy M. Tooth brushing, tooth wear and dentine hypersensitivity - are they associated?. Int Dent J. 2005;55(4 Suppl 1):261-7. PubMed PMID: 16167604.
- Addy M, Smith SR. Dentine hypersensitivity: an overview on which to base tubule occlusion as a management concept. J Clin Dent. 2010;21(2):25-30. PubMed PMID: 20669812.
- Addy M, West N. Etiology, mechanisms and management of dentine hypersensitivity. Curr Opin Periodontol. 1994:71-7. PubMed PMID: 8032468.
- Canadian Advisory Board on Dentine Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentine hypersensitivity. J Can Dent Assoc. 2003 Apr;69(4):221-6. PubMed PMID: 12662460.
- Addy M, Dummer PM, Hunter ML, Kingdon A, Shaw WC. The effect of toothbrushing frequency, toothbrushing hand, sex and social class on the incidence of plaque, gingivitis and pocketing in adolescents: a longitudinal cohort study. Community Dent Health. 1990 Sep;7(3):237-47. PubMed PMID: 2076500.
- Drisko C. Oral hygiene and periodontal considerations in preventing and managing dentine hypersensitivity. Int Dent J. 2007 Dec;57(S6):399-410.
- Fardal O, Johannessen AC, Linden GJ. Patient perceptions of periodontal therapy completed in a periodontal practice. J Periodontol. 2002 Sep;73(9):1060-6. PubMed PMID: 12296592.
- Gernhardt CR. How valid and applicable are current diagnostic criteria and assessment methods for dentin hypersensitivity? An overview. Clin Oral Investig. 2013 Mar;17 Suppl 1:S31-40. doi: 10.1007/s00784-012-0891-1. PubMed PMID: 23224044.
- Gibson B, Boiko OV, Baker S, Robinson PG, Barlow A, Player T, Locker D. The everyday impact of dentine sensitivity: personal and functional aspects. Soc Sci Dent . 2010;1(1):11-20.
- Gillam DG, Orchardson R. Advances in the treatment of root dentine sensitivity: mechanisms and treatment principles. Endod Topics. 2006 Mar;13(1):13-33.
- Holland G, Narhi MN, Addy M, Gangarosa L, Orchardson R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontol. 1997 Nov;24(11):808-13. PubMed PMID: 9402502.
- Mason S, Hughes N, Sufi F, Bannon L, Maggio B, North M, et al. A comparative clinical study investigating the efficacy of a dentifrice containing 8% strontium acetate and 1040 ppm fluoride in a silica base and a control dentifrice containing 1450 ppm fluoride in a silica base to provide immediate relief of dentin hypersensitivity. J Clin Dent. 2010;21(2):42-8. PubMed PMID: 20669815.
- West NX, Sanz M, Lussi A, Bartlett D, Bouchard P, Bourgeois D. Prevalence of dentine hypersensitivity and study of associated factors: a European population- based cross-sectional study. J Dent. 2013 Oct;41(10):841-51. doi: 10.1016/j.jdent.2013.07.017. PubMed PMID: 23911597.
- Olley RC, Wilson R, Moazzez R, Bartlett D. Validation of a Cumulative Hypersensitivity Index (CHI) for dentine hypersensitivity severity. J Clin Periodontol. 2013 Oct;40(10):942-7. doi: 10.1111/jcpe.12144. PubMed PMID: 23998374.
- Pashley DH. Mechanisms of dentine hypersensitivity. Dent Clin North Am. 1990 Jul;34(3):449-73. PubMed PMID: 2197121.
- Schiff T, Dotson M, Cohen S, De WV, McCool J, Volpe A. Efficacy of a dentifrice containing potassium nitrate, soluble pyrophosphate, PVM/MA copolymer, and sodium fluoride on dentinal hypersensitivity: a twelve-week clinical study. The J Clin Dent. 1994;5 Spec No:87-92. PubMed PMID: 8534380.
- Susin C, Haas AN, Oppermann RV, Haugejorden O, Albandar JM. Gingival recession: epidemiology and risk indicators in a representative urban Brazilian population. J Periodontol. 2004 Oct;75(10):1377-86. PubMed PMID: 15562916.
- Tammaro S, Wennström JL, Bergenholtz G. Root‐dentin sensitivity following non‐surgical periodontal treatment. J Clin Periodontol. 2000 Sep;27(9):690-7. PubMed PMID: 10983603.





