Troponin T as a Diagnostic Marker in the Detection of Acute Myocardial Infarction at Autopsy
Kathleen Han*, Richard Flavin
Department of Pathology, University Hospital Galway, Ireland.
*Corresponding Author
Kathleen Han,
Department of Pathology,
The National Maternity Hospital,
Holles Street, Dublin 2, Ireland.
Tel: +353 87 9389 400.
E-mail: kathleen.han@lycos.com
Article Type: Short Report.
Received: April 23, 2014; Accepted: May 20, 2014; Published: May 21, 2014
Citation: Han K, Flavin R (2014) Troponin T as a Diagnostic Marker in the Detection of Acute Myocardial Infarction at Autopsy. Int J Forensic Sci Pathol. 2(4), 28-29. doi: dx.doi.org/10.19070/2332-287X-140009
Copyright: Han K© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Sudden adult cardiac death accounts for a significant proportion of autopsies performed. In the clinical setting, electrocardiography and cardiac Troponin are the gold standard in detecting acute myocardial infarction. The use of cardiac Troponin T at autopsy is less clear. This study evaluates the sensitivity and specificity of cardiac Troponin in the detection of acute myocardial infarction at autopsy. A retrospective study was performed, identifying autopsy cases where serum Troponin was requested. In these cases, cause of death was identified from autopsy reports, the histology reviewed and Troponin T levels were recorded. Acute myocardial infarction was confirmed as a cause of death in 72 out of the 196 cases with 66 cases having an elevated Troponin T. (Sensitivity: 92%; Specificity: 5%). The results of this study suggest that while Troponin T is sensitive marker, it is not specific as a diagnostic tool in the detection of acute myocardial infarction at autopsy. Histology remains the gold standard.
2.Introduction
3.Materials and Method
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Troponin; Autopsy; Acute Myocardial Infarction.
Introduction
Sudden cardiac death due to an acute myocardial infarction (AMI) comprises a significant proportion of autopsy cases. In clinical practice, AMI is diagnosed with the aid of the electrocardiogram and serum biochemical markers specific in the detection of myocardial damage [1-3]. Troponin T and Troponin I in particular have been extensively studied and proof of sensitivity and specificity in detecting AMI is well established [3-6]. Troponin is a complex of three regulatory proteins (Troponin C, I and T) that is integral to muscle contraction in skeletal and cardiac muscle [7]. It is a component of thin filaments along with actin and tropomyosin and is the protein to which calcium binds to accomplish regulation of contraction and relaxation of the cardiac muscle. During myocardial injury, as seen in AMI, Troponin is released from the injured myocyte into the circulation which can be detected biochemically. The potential role however of Troponin in the diagnosis of AMI at post-mortem is less well known [8-10]. In this study, we evaluate the sensitivity and specificity of Troponin T as a diagnostic tool in the detection of AMI at autopsy.
Materials and Method
We conducted a retrospective study of post mortem examinations that were performed in the Department of Pathology, University Hospital Galway, Ireland between 2007 and 2010. All cases where Troponin T analysis was performed at the time of autopsy were included in the study. Blood samples were drawn from the femoral vessels of the deceased and analysed at the Department of Biochemistry, University Hospital Galway using the Roche Elecsys Diagnostics™ System. An elevated Troponin T level was defined as being greater than 0.03mg/L. All demographic data, autopsy findings (including cause of death, serum Troponin T levels and histology) were reviewed by the two authors. The cause of death was classified into eight distinct categories. Atheroscerotic coronary artery disease was defined as evidence of atherosclerosis occupying more than 75% of vessel lumen. Statistical analysis was performed using Analyse-IT® from Microsoft Excel. The chi-squared test was used to perform two by two comparisons. Ethical approval for the study was granted by the Galway University Hospital Ethics Committee (Reference no C.A. 660).
Results
A total of 1493 post mortem examinations were carried out between 2007 and 2010. There were 207 cases where serum Troponin T was analysed (14% of all autopsy cases). 1 of the 207 cases (5%) were excluded, due to severe haemolysis of sample rendering interpretation impossible. The cause of death, presence or absence of AMI and Troponin T levels are outlined in Table 1. Ante mortem blood troponin levels were not available in the majority of cases and were not included in this study. AMI was established as a cause of death in 72 of the 196 cases (36.7%) and confirmed on histological examination. Of the 72 cases of AMI, 66 (92%) showed an elevated Troponin T level [> 0.03mg/L]. There were 117 cases where the Troponin T levels were elevated but the cause of death was due to alternate causes other than an AMI. This yielded a sensitivity of 92% and a specificity of 5% (p=0.62; chi-squared test) for Troponin T in predicting an AMI at autopsy. Correspondingly, the positive and negative predictive value of Troponin T was 36% and 57% respectively.
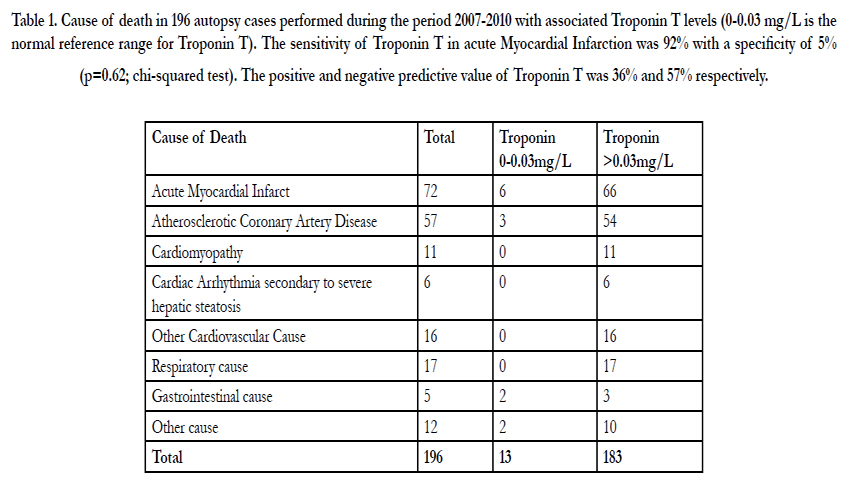

Table 1. Cause of death in 196 autopsy cases performed during the period 2007-2010 with associated Troponin T levels (0-0.03 mg/L is the normal reference range for Troponin T). The sensitivity of Troponin T in acute Myocardial Infarction was 92% with a specificity of 5% (p=0.62; chi-squared test). The positive and negative predictive value of Troponin T was 36% and 57% respectively.
Discussion
In clinical practice, Troponin T has been extensively investigated and found to be a sensitive marker of myocardial necrosis. While our study confirms that Troponin T is sensitive at detecting AMI, it is unfortunately not specific to this disease process.
In our study, there were 117 cases where Troponin T levels were elevated without an established diagnosis of AMI. Interestingly, in all of these cases, there was histological evidence of ischaemic heart disease represented by either myocardial fibrosis,early coronary artery disease (where occlusion of the vessel was less than 75%) or a combination of both. In the cases where AMI was present, the age of the infarct did not correlate with the rise in troponin T levels.
Macroscopic changes of AMI become apparent only after 2-3 days from onset of symptoms making identification of early myocardial damage challenging to the pathologist. Without macroscopic change, methodical sampling of myocardium cannot guarantee detecting microscopic evidence of AMI. This could possible explain the rise in Troponin levels in some of our cases, where microscopic diagnosis of AMI is not seen. In addition, in cases where death is immediate, histologic changes will not be established and so even extensive sampling may not provide a histological diagnosis of AMI. However, elevated levels of Troponin T may be useful as an adjunct test especially if the deceased has established coronary artery atherosclerosis (with or without thrombosis).
In our study, we observed that 63.3% of deaths were not due to AMI. Cause of death included bronchopneumonia, multi-organ failure and cerebrovascular haemorrhage where the Troponin T levels were elevated. In such cases, systemic hypovolaemia or agonal global hypoxia could result in coronary ischaemia leading to an increased Troponin levels. In addition, cardiopulmonary resuscitation may have contributed to cardiac injury resulting in an elevation of Troponin T levels.
This study was limited by factors including variance in post mortem interval from time of death; post mortem refrigeration time and blood sample haemolysis. Under routine conditions, most bodies presenting for autopsy will demonstrate some degree of autolysis. This process is dependent on a number of key factors including duration of death prior to post mortem examination,interval between death and refrigeration and seasonal variance.
The time interval from death to autopsy in this study varied from 2-30 hours (data not shown) and all cases showed a degree of haemolysis in the blood retrieved for analysis. There was no correlation between the troponin levels and duration of death prior to femoral blood testing.
Conclusion
The findings from our study confirm that while Troponin T is a sensitive marker in the detection of AMI at autopsy it is not specific and therefore cannot be used as a diagnostic tool at autopsy. There are multiple factors that can attribute to an elevated Troponin T result following death. Histological evaluation for the diagnosis of AMI remains the gold standard.
References
- Jaffe AS, Babuin L, Apple FS (2006). Biomarkers in acute cardiac disease: the present and the future. Journal of American College of Cardiology; 48(1):1–11.
- Kavsak PA, MacRae AR, Lustig V, Bhargava R, Vandersluis R, et al.(2006) The impact of the ESC/ACC redefinition of myocardial infarction and new sensitive Troponin assays on the frequency of acute myocardial infarction. American Heart Journal; 152(1):118–25.
- Batalis NI, Marcus, BJ, Papadea CN, Collins KA(2010). The role of Post mortem Cardiac Markers in the Diagnosis of Acute Myocardial Infarction J Forensic Science July, Vol 55, No 4.
- Katus HA, Remppis A, Neumann FJ, Scheffold T, Diederich KW, et al. (1991) Diagnostic efficiency of troponon T measurements in acute myocardial infarction. Circulation.; 83; 902-912.
- Osuna E, Perez-Carceles MD, Alvarez MV, Noguera J, Luna A(1998). Cardiac Troponin I and the post mortem diagnosis of myocardial infarction International Journal of Legal medicine.;111(4);173-1761
- Adams JE, Bodor GS, Davila-Roman VG, Delmez JA, Apple FS, et al.(1993) Cardiac troponin I. A marker with high specificity for cardiac injury. Circulation; 88:101-106
- Ross G, Bever F, Uddin ZI, Hockman EM (2000). Troponin I sensitivity and specificity for the diagnosis of acute myocardial infarction. Journal of American Osteopathic Association January Vol 100 No 1;29-32
- Vargas S, Grudzien C, Tanasijevic MJ(2008). Postmortem cardiac Troponin I levels predict intramyocardial damage at autopsy. J Thromb Thrombolysis. Oct;26(2):132-7.
- Zhu BL, Ishikawa T, Michiue T, Li DR, Zhao D, et al.(2006) Post mortem cardiac troponin T levels in the blood and pericardial fluid. Part 1. Analysis with special regard to traumatic causes of death. Legal medicine (Tokyo): 8(2):86-93
- Zhu BL, Ishikawa T, Michiue T, Li DR, Zhao D, et al.(2006) Postmortem cardiac Troponin T levels in the blood and pericardial fluid. Part 2: analysis for application in the diagnosis of sudden cardiac death with regard to pathology. Legal Medicine (Tokyo); 8(2):94-101.





