Suicide among Adolescents in Center Tunisia: An 18-Year Autopsy Study
Jedidi M1*, Mlayeh S2, Hamila I1, Masmoudi T1, Ben Dhiab M1, Zemni M1, Souguir M K1
1 Department of Legal Medicine, Farhat Hached University Hospital Sousse, Tunisia.
2 Department of Legal Medicine, Ibn Jazzar University Hospital, Kairouan, Tunisia.
*Corresponding Author
Maher Jedidi
Department of Legal Medicine, Farhat Hached University Hospital Sousse, Tunisia.
Tel: +216 98 536 440
Fax: + 216 73 226 702
Email : jedidimaher@yahoo.fr
Received: August 24, 2016; Accepted: September 29, 2016; Published: September 30, 2016
Citation: Jedidi M, Mlayeh S, Hamila I, Masmoudi T, Ben Dhiab M, et al., (2016) Suicide among Adolescents in Center Tunisia: An 18-Year Autopsy Study. Int J Forensic Sci Pathol.4(9), 271-275.
doi:dx.doi.org/10.19070/2332-287X-1600064
Copyright: Jedidi M© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Suicide and suicide attempts are more common among adolescents. Many factors are known to influence suicide in particular: region and culture. Adolescent suicide has been widely studied in many countries, but there are, currently, no data relating to adolescent suicide in Tunisia.
Aim: The aims of this study were to describe epidemiological aspects of death related to adolescent suicide in Sousse, a city in central Tunisia.
Methods: Data of forensic autopsies from 1998 to 2015 related to suicide of adolescents were retrospectively examined considering age, gender, method of death, year and risk factor.
Results: 70 cases were reported with female predominance (62, 8%). The age range was from 10 to 19 and most of the suicides occurred in the 15-to-19 age group (75, 7%). Most victims were from rural zones (70%). Self-poisoning was the most used method (47, 1 %) followed by hanging (35, 7%). Hanging was the most common method used by males (17/26) and self-poisoning by females (29/44). Self-poisoning was related to pesticides in the vast majority of cases (29 cases among 33). The identified precipitating factors were chronic family problems in 51.4%, sentimental deception in 8.6%.
Conclusion: This retrospective study raises concerns regarding the use of pesticides and the urgent need to provide rural areas with structures and medical equipment. This will ensure adequate suicide prevention in the region.
2.Introduction
3.Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Suicide ; Adolescent ; Autopsy ; Tunisia.
Introduction
Suicide is defined as a fatal, intentional and self-inflicted injury with the intent of ending their lives [1, 2]. According to the World Health Organization (WHO), approximately one million people per year commit suicide [3-4]. Suicide is a complex phenomenon and many factors are known to influence it in particular: region and culture [5]. Suicide ideation and suicide attempts are more common among children and adolescents [6].
Suicide attempts during adolescence are seen as prevalent compared to those in other age groups and there is a high rate between suicide attempts and actual suicide among adolescents [6-7].
Adolescent suicide has been widely studied in developed countries such as the USA and many countries in Europe [8-13]. In contrast, there has been little clinical study in many Arab and Muslim countries where the general incidence of suicide is unknown even though considered to be low [14-16]. The WHO considers adolescent suicide to be the one of a person between 10 and 19 years of age [3-4].
In Tunisia, an Arabic Muslim country in North Africa with a current estimated population of 11 millions, according to the law, suicide is considered as a suspect death; therefore a medico-legal autopsy should be performed in a forensic department. Police investigation, death scene investigation and autopsy allow us to determine the manner of death. But, in fact, except the cases of apparent suicide, several cases are hidden and reported by the families of the deceased persons as accidents. Probably out of fear of potential lawsuits and mostly for fear of family dishonor by the suicide of one of them, especially if the person involved is a young one. This is likely to be true for precipitation, and sometimes even drowning and poisoning whose manner of death (natural, suicide, homicide) still often undetermined. For this reason, there is currently no official data on the exact incidence of suicidal death in general in Tunisia and there is no data relating to adolescent suicide.
The aim of our study consists in describing the epidemiological aspects of death related to adolescent suicide in Sousse, a city in central Tunisia, in terms of age, sex, geographical origin, methods of suicide, and analyses the involved factors.
Methods
From January 1998 to December 2015, we retrospectively examined the autopsy files of all the cases of adolescent death autopsied at the Farhat Hached university hospital legal medicine department in Sousse, which receives all medico-legal deaths of the center of Tunisia, with an estimated population of one million.
All recorded cases were retrospectively analyzed with consideration of age, gender, place, mode of death, year and risk factors. Additional information regarding social and psychological background was obtained from family and police records. Combined examination of the autopsy and police records was intended to register death as suicide. Available data was analyzed using Microsoft Excel and Statistical Package for Social Sciences (SPSS) for Windows.
Results
A total of 70 cases of adolescent suicide were reported within the period between 1998 and 2015, and represent 10% of all suicides and 1.7% of all autopsies. Time distribution of adolescent suicide per year showed no increase over the years (Figure. 1).
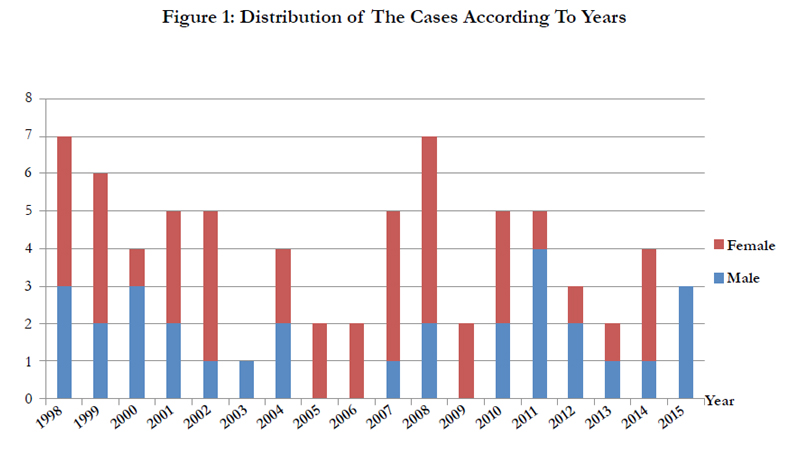
Figure 1: Distribution of The Cases According To Years.
Sex distribution revealed 44 females (62.8%), and 26 males (37.2%). Age range was from 10 to 19 year and most of the suicides occurred in the 15-to-19 age group (75.7%). However, 24.3% (17/70) were under the age of 15. Most victims were from rural zones (70%). History of suicidal ideation or suicide attempts hasn’t been reported in any case. A summary of cases characteristics is shown in Table 1.
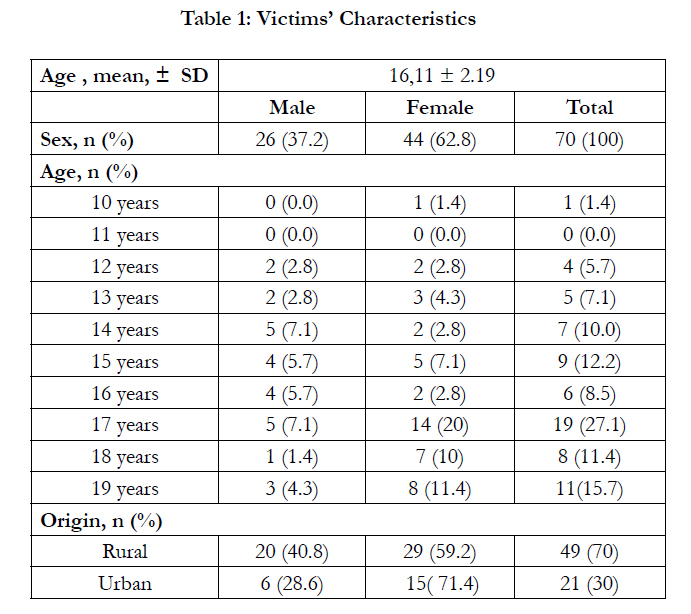

Table 1: Victims’ Characteristics
Self-poisoning was the most used suicidal means in 33 cases (47.1%) followed by hanging (35.7%). Hanging was the most common means used by male adolescents (17/26). In the 44 female adolescents suicides, 29 (65.9%) were related to self-poisoning and 8 (17,4%) to hanging. Self-poisoning was related to pesticides in the vast majority of cases (29 cases among 33). Carbamate pesticide was incriminated in 46 %, organophosphate pesticide in 36% and organochlorate pesticide in 2%. Only, four cases (4%) of self-poisoning with medicine (Beta-adrenergic blocking agents) were found.
In all cases, no information was mentioned about psychiatric disorders. However, the identified precipitating factors were chronic family problems (fight with a family member or stressed discipline at home), in 51.4%, sentimental deception (cheating boyfriend / girlfriend), in 8.6%, and illegitimate pregnancy in 5.7%.The suicide characteristics are shown in Table 2.
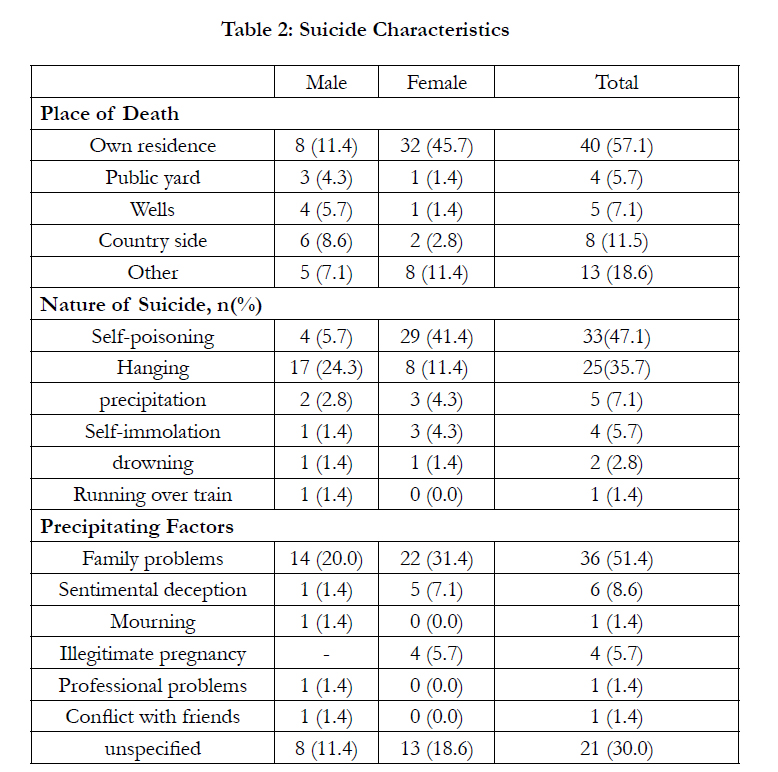
Table 2: Suicide Characteristics
Discussion
This is the first reported analysis of adolescent suicide cases in Tunisia. Although the experience of our staff indicates that the incidence of suicidal death is in continual progress, we believe it is still much lower than that reported in European or North American countries [8-13].This may be explained by the trend of life in occidental societies [17-19]. Underreporting is another issue to be considered especially in Arab Muslim context.
Actually, many studies emphasize the fact that religious values may protect against suicide [20-22]. This can be verified through Islam religion. Indeed, Islam explicitly prohibits taking one’s own life because by doing so you will interfere with God’s will, according to several Surats in the Quran. A study by Kok [23] examined the suicide rates among the 3 ethnic groups of Singapore concluding that the ethnic Malays, whose main religion is Islam, had by far the lowest suicide rate. A review of research from Israel showing that suicide epidemiology among the Arab population of children and adolescents displays a low incidence. However an increase has been observed over the past decade, but still much lower than within Jewish population [15].
Our study has shown that numbers of suicides of adolescents over the past 18 years have been small with no appreciable increase. This stability has also been noticed in South Australia and San Diego County (USA) [24]. This goes in opposition with other studies which have suggested that child’s suicide is a growing problem [9, 12, 25].
The WHO defines two categories among early suicide adolescent. A juvenile suicide as death of child between 10 and 15 years-old, and adolescent suicide between 15 and 19 years-old [3, 4]. In our study, suicide in the 15-19 years age group is three times (53/17) more predominant than in 10-14 age group. These findings are favorably compared to a recent study of Schmidtke et al which showed in Europe that the highest number of suicide attempts is reported among older adolescents (between 15 and 34 years-old) [18]. These results are confirmed by many other reports [10, 16, 25-27].
As observed in our study, the number of suicides among females is higher than that observed among males with a male-to-female suicide ratio being 2/3. This result is similar to that found in a study conducted in Turkey in similar age groups [7]. On the other hand, in the majority of studies, the rate of suicide was reported to be higher among men [19, 26-30]. This finding may be explained by social strains of women in Tunisia. In fact, women, and especially in rural regions where female suicide was predominant, are ranked in an inferior position with regards to men. In addition, the family is less tolerant towards female adolescents who are more exposed to mistreatment than men from their parents and even from their brothers. It has also been reported that women, especially at a younger age group, have a higher rate of suicide attempts than men, reflecting their emotional liability and vulnerability to frustrations when compared to males [31, 32].
Difference in suicidal rates between rural and urban areas was also remarkable (49 versus 21 cases). Differences in suicidal rates between urban and rural areas have previously been investigated internationally [7, 26, 27, 33] with higher rural suicide rates. Explanations for these differences have been largely speculated and have included urban–rural differences in employment opportunities, early marriage age, illiteracy, easy access to lethal methods especially to pesticide products and a dominant masculine culture [34-36]. Added to this, the lack of medical structure and distance from hospital in rural area,may explain that a majority of suicide attempts are becoming completed suicide and explains the absence of the so-called gender paradox, as reported by Canetto and Sakinofsky where usually it's women who most likely attempt suicide but succeed much less frequently than men [31].
Although it has been shown that mental disorders have the strongest associations with suicide [29, 37- 40], mental disorder history or a prior suicide attempt lacking in all cases of this study. Indeed, previous suicide attempts and mental illnesses are considered taboo and are not easily revealed by the family.
With regard to precipitating factors, chronic family problems and sentimental deception were the two major ones in this study. Sankey classified the adolescent suicide into three groups: in the first and majority group (66%), the suicide occurred in the context of significant enduring or chronic difficulties with family and at school. In the second group (14%), suicide occurred as a reaction to a stressful life event such as interpersonal issues including sentimental deceptions and relationship break-ups, deaths of significant people, legal problems and unemployment. In the last group [28], the adolescents died while engaging in common adolescent risk-taking behaviors, notably drug and alcohol use or dangerous driving [40].
Toxicology results show no drug or alcohol use in suicide adolescent victims, suggesting that in this population, suicide is probably an impulse reaction to a stressful life event. By contrast, as in many other reports, drugs or alcohol have been described as a significant risk factor to commit suicide especially among older adolescent male victims [41-43]. No victims left a suicide note, in contrast to the findings of other studies [8, 9, 44].
Methods of suicide were varied then our study and a gender difference existed. Self-agriculture pesticide poisoning, especially with Carbamate pesticide, was the first suicide method among female victims (27/44). The predominance of self-poisoning can be explained by the higher number of female victims (62,8%) which favors less violent methods [8]. We think, as reported in multiple studies [5,6, 19, 26, 35], that pesticide accessibility in rural environment where they are very used by farmers, promotes the choice of this method of suicide by the adolescents; both because of their availability and their low price in our markets. Similarly, the lack of knowledge on the potentially lethal nature of drugs and the lack of fatal drugs can explain the low number of drug-overdose deaths in our study (one case).
As reported in many studies, and with no regard to the number of female victims, hanging is still the most frequent and well-known method of suicide [10, 15]. It was the most used method by males. The private nature of hanging, its practicability and its known efficiency make of it the first suicide method for all ages. Precipitation is as well a common method of suicide in our country. All the victims coming from rural cities, where there is a widespread of unprotected wells, death occurs by poly-trauma or drowning [45].
In this study, there were no cases of firearm suicide ; in contrast with European countries and the USA, where one of the most common methods of suicide among adolescents and young adults are hanging and firearm [11-13, 24, 36] .In Tunisia, restrictive laws detentions of firearms explain the very low incidence of firearm suicides among adolescent and all age categories. In fact it has been shown that the greater is the availability of guns, the lower are the suicide rates by other methods [46].
Conclusion
This study showed that adolescents suicide in Tunisia, concerned more females than men and especially in rural areas. The most used methods of suicide were self-poisoning pesticide for females and hanging for males. Suicide appears to be an impulse reaction to a stressful life event. Victims have neither mental illness nor drug or alcohol abuse.
Finally, this retrospective review raises concerns regarding several issues, in particular the use of pesticides that should have strict regulation and the urgent need to provide rural areas with medical structures and equipment in order to allow easy resuscitation of victims of suicide attempts, and early diagnosis of psychiatric disorders. This will ensure adequate prevention of suicide.
References
- Silverman MM, Berman AL, Sanddal ND, O'carroll PW, Joiner TE (2007) Rebuilding the tower of Babel: a revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life Threat Behav. 37(3): 264-77.
- O'Carroll PW, Berman AL, Maris RW, Moscicki EK, Tanney BL, et al., (1996) Beyond the Tower of Babel: a nomenclature for suicidology. Suicide Life Threat Behav. 26(3): 237-52.
- No authors listed] (2003) Age limits and adolescents. Paediatr Child Health. 8(9): 577-8.
- World Health Organization (WHO), Preventing suicide: a resource for general physicians, 2000.
www.who.int/mental_health/media/en/56.pdf - Mendes R, Santos S, Taveira F, Dinis-Oliveira RJ, Santos A, et al., (2015) Child suicide in the north of Portugal. J Forensic Sci. 60(2): 471-475.
- Shain BN (2007) Suicide and suicide attempts in adolescents. American Academy of Pediatrics Committee on Adolescence. Pediatrics. 120(3): 669-76.
- Kafadar H, Kafadar S, Tokdemir M (2014) Suicides in adolescence: a twelve-year study from Eastern Turkey. J Forensic Leg Med. 27: 6-8.
- Perret G, Abudureheman A, Perret-Catipovic M, Flomenbaum M, La Harpe R (2006) Suicides in the young people of Geneva, Switzerland, from 1993 to 2002. J Forensic Sci. 51(5): 1169-73.
- Klostermann P, Ganswindt M, Schneider V (2005) Suicide among adolescents and young adults. Forensic Sci Int. 147: S41-2.
- Groholt B, Ekeberg O, Wichstrom L, Haldorsen T (1998) Suicide among children and younger and older adolescents in Norway: a comparative study. J Am Acad Child Adolesc Psychiatry. 37(5): 473-481.
- Baron D, Paglia C, Thorkelson G, Namdari M (2009) Suicide in teens and young adults in the United States. Quaderni Italiani di Psichiatria. 28(3): 96-101.
- Roesler J (1997) The incidence of child suicide in Minnesota. Minn Med. 80(12): 45-47.
- Lecomte D, Fornes P (1998) Suicide among youth and young adults, 15 through 24 years of age. A report of 392 cases from Paris, 1989-1996. J Forensic Sci. 43(5): 964-968.
- Koronfel AA (2002) Suicide in Dubai, United Arab Emirates. J Clin Forensic Med. 9(1): 5-11.
- Farbstein I, Dycian A, Gothelf D, King RA, Cohen DJ, et al., (2002) A follow-up study of adolescent attempted suicide in Israel. J Am Acad Child Adolesc Psychiatry. 41(11): 1342-1349.
- Agritmiş H, Yayci N, Colak B, Aksoy E (2004) Suicidal deaths in childhood and adolescence. Forensic Sci Int. 142(1): 25-31.
- Cantor CH, Leenaars AA, Lester D, Slater PJ, Wolanowski AM, et al., (1996) Suicide trends in eight predominantly English-speaking countries 1960-1989. Soc Psychiatry Psychiatr Epidemiol. 31(6): 364-73.
- Schmidtke A, Bille-Brahe U, DeLeo D, Kerkhof A, Crepet P, et al., (1996) Attempted suicide in Europe: rates, trends and sociodemographic characteristics of suicide attempters during the period 1989–1992. Results of the WHO/EURO multicentre study on parasuicide. Acta Psychiatr Scand. 93(5): 327-338.
- Lee CJ, Collins KA, Burgess SE (1999) Suicide under the age of eighteen: a 10-year retrospective study. Am J Forensic Med Pathol. 20(1): 27-30.
- Neeleman J, Mak V, Wessely S (1997) Suicide by age, ethnic group, coroners' verdicts and country of birth. A three-year survey in inner London. Br J Psychiatry. 171: 463-467.
- Dervic K, Oquendo MA, Grunebaum MF, Ellis S, Burke AK, et al., (2004) Religious affiliation and suicide attempt. Am J Psychiatry. 161(12): 2303- 2308.
- Gearing RE, Lizardi D (2009) Religion and suicide. J Relig Health. 48(3): 332-341.
- Kok LP (1988) Race, religion and female suicide attempters in Singapore. Soc Psychiatry Psychiatr Epidemiol. 23(4): 236-239.
- Byard RW, Markopoulos D, Prasad D, Eitzen D, James RA, et al., (2000) Early adolescent suicide: a comparative study. J Clin Forensic Med. 7(1): 6-9.
- Singh VD, Lathrop SL (2008) Youth suicide in New Mexico: a 26-year retrospective review. J Forensic Sci. 53(3): 703-708.
- Hoberman HM, Garfinkel BD (1988) Completed suicide in children and adolescents. J Am Acad Child Adolesc Psychiatry. 27(6): 689-695.
- Sharma B, Nam E, Kim H, Kim J (2015) Factors Associated with Suicidal Ideation and Suicide Attempt among School-Going Urban Adolescents in Peru. Int J Environ Res Public Health. 12(12): 14842-1456.
- Shaw D, Fernandes JR, Rao C (2005) Suicide in children and adolescents: a 10-year retrospective review. Am J Forensic Med Pathol. 26(4): 309-315.
- Lahti A, Harju A, Hakko H, Riala K, Räsänen P (2014) Suicide in children and young adolescents: a 25-year database on suicides from Northern Finland. J Psychiatr Res. 58: 123-128.
- Schmidt P, Müller R, Dettmeyer R, Madea B (2002) Suicide in children, adolescents and young adults. Forensic Sci Int. 127(3): 161-167.
- Canetto S, Sakinofsky I (1998) The gender paradox in suicide. Suicide and Life-Threat Behav. 28(1): 1-23.
- Brent DA (1995) Risk factors for adolescent suicide and suicidal behavior: mental and substance abuse disorders, family environmental factors, and life stress. Suicide Life Threat Behav. 25: 52-63.
- Choi K-H, Kim D-H (2015) Trend of Suicide Rates According to Urbanity among Adolescents by Gender and Suicide Method in Korea, 1997-2012. Int J Environ Res Public Health. 12(5): 5129-5142.
- Langhinrichsen-Rohling J, Friend J, Powell A (2009) Adolescent suicide, gender, and culture: A rate and risk factor analysis. Aggression and Violent Behavior. 14(5): 402-414.
- Sing Lee (2000) In China, suicide in young women is a problem too. BMJ. 321(7261): 636-637.
- Baume PJ, Clinton ME (1997) Social and cultural patterns of suicide in young people in rural Australia. Aust J Rural Health. 5(3): 115-20.
- Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM (2003) Psychological autopsy studies of suicide: a systematic review. Psychol Med. 33(3): 395-405.
- Dervic K, Gould MS, Lenz G, Kleinman M, Akkaya-Kalayci T, et al., (2006) Youth suicide risk factors and attitudes in New York and Vienna: a crosscultural comparison. Suicide Life Threat Behav. 36(5): 539-552.
- Bouhlel S, M’solly M, Benhawala S, Jones Y, El-Hechmi Z (2013) Les facteurs liés aux tentatives de suicide dans une population tunisienne de patients atteints de schizophrénie. Encephale. 39(1): 6-12.
- Sankey M, Lawrence R (2005) Brief report: classification of adolescent suicide and risk-taking deaths. J Adolesc. 28(6): 781-785.
- Chatterji P, Dave D, Kaestner R, Markowitz S (2004) Alcohol abuse and suicide attempts among youth. Econ Hum Biol. 2(2): 159-1580.
- Schilling EA, Aseltine RH Jr, Glanovsky JL, James A, Jacobs D (2009) Adolescent alcohol use, suicidal ideation, and suicide attempts. J Adolesc Health.44(4): 335-341.
- Wu P, Hoven CW, Liu X, Cohen P, Fuller CJ, et al., (2004) Substance use, suicidal ideation and attempts in children and adolescents. Suicide Life Threat Behav. 34(4): 408-420.
- Kuwabara H, Shioiri T, Nishimura A, Abe R, Nushida H, et al., (2006) Differences in characteristics between suicide victims who left notes or not. J Affect Disord. 94(1-3): 145-149.
- Perret G, Flomenbaum M, La Harpe R (2003) Suicides by fall from height in Geneva, Switzerland, from 1991 to 2000. J Forensic Sci. 48(4): 821-826.
- Lester D (1990) The availability of firearms and the use of firearms for suicide: a study of 20 countries. Acta Psychiatr Scand. 81(2): 146-147.





