Demographic Characteristics of Normal Tension Glaucoma Seen in a Suburban Tertiary Hospital
Ajite KO*, Fadamiro CO, Ajayi IA, Omotoye OJ, Salami TK, Abah EC
Department of Ophthalmology, Ekiti State University Teaching Hospital, Ado Ekiti, Ekiti State, Nigeria.
*Corresponding Author
Ajite KO, FWACS, FMCOph, MPH,
Department of Ophthalmology,
Ekiti State University Teaching Hospital, Ado Ekiti,
Ekiti State, Nigeria.
E-mail: bidemi_kayode@yahoo.com
Received: March 16, 2016; Accepted: June 10, 2016; Published: June 15, 2016
Citation: Ajite KO, et al., (2016) Demographic Characteristics of Normal Tension Glaucoma Seen in a Suburban Tertiary Hospital. Int J Ophthalmol Eye Res. 4(5), 215-219.DOI : dx.doi.org/10.19070/2332-290X-1500044
Copyright: Ajite KO© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Normal Tension Glaucoma (NTG) is a form of glaucoma in which there are distinct demographic characteristics and associated factors to its development. Identifying these characteristics helps early diagnosis and prevention of blindness. Aim of the study is to identify the various demographic characteristics and associated factors with the diagnosis of NTG in patients presenting to the glaucoma clinic of a tertiary hospital.
Methods: All consecutive newly diagnosed glaucoma patients attending the eye clinic of EKSUTH, Ado Ekiti, from January 2012 to December 2014 were selected for the study. They all had thorough ocular and systemic examination. The patients with diagnosis of normal tension glaucoma had a protocol prepared for the study administered on them. Demographic data, family history of glaucoma, history of migraine, hypertension, and use of antihypertensive drugs at night were obtained from them. Data were analysed using SPSS version 18 and presented as tables, and figures, in frequencies, and percentage.
Result: A total of 1265 patients were newly diagnosed to have glaucoma, of these, 864(68.3%) were POAG, 336(26.6%) were secondary glaucomas, 48(3.8%) normal tension glaucoma,12(0.9%) angle closure glaucoma and 5(0.4%) were developmental glaucoma. Among the NTG patients, 30(62.5%) were females and 18(37.5%) males,(M:F =1.7:1) Age range was between 30years to 68years, median age of 59.3years.The identifiable associated factors in NTG patients include; family history of glaucoma 33(68.8%), hypertension and use of antihypertensive at night before sleep 24(50%), history suggestive of sleep apnea 6(12.5%), migraine headaches 10(20.8%) and thyroid disease 2(4.2%). No statistically significant association of these factors with severity of visual field defect in the subjects studied.
Conclusion: This study suggests that age and positive family history of glaucoma are important demographic characteristics for consideration in diagnosis of NTG.
2.Introduction
3.Methods
4.Result
5.Discussion
6.Conclusion
7.References
Keywords
Associated Factors; Normal Tension Glaucoma; Family History; Health Education.
Introduction
Increased intraocular pressure (IOP) is a major risk factor for glaucomatous damage and reducing IOP improves prognosis. However, there are growing evidences in the literature that other associated factors besides IOP such as unstable ocular perfusion are involved [17, 18]. The definition of the normal tension glaucoma has been a diagnostic dilemma since its original description by Von Graefe in 1857 [23]. Kamal and Hitchings defined normal tension glaucoma with the following criteria; A mean IOP equal to or less than 21 mm Hg on diurnal testing, with no pressure spikes greater than 24 mm Hg, glaucomatous cupping of the optic nerve head with corresponding visual field defects, open angles on gonioscopy, absence of any possible contributing ocular or systemic disorders, and progression of glaucomatous damage [13]. The main theme in the current literature continues to be that NTG and primary open-angle glaucoma (POAG) represent a continuum of open-angle glaucomas. There is considerable overlap between the two conditions, however, within the population of NTG patients there are subsets in which IOP, blood flow and other factors assume relative importance [22]. The prevalence of normal tension glaucoma is not exactly known, however in individuals above 40 years of age, its prevalence is 0.2% [14]. It represents 16% to 50% of all cases of primary open angle glaucoma [14]. It is said to be more common in women than men [14]. A variety of cardiovascular and hematologic abnormalities have been described in patients with NTG including hemodynamic crisis, hypercoagulability, reduced diastolic ophthalmodynamometry, nocturnal systemic hypotension, increased blood and plasma viscosity, elevated blood cholesterol and lipids, carotid artery disease, slowed parapapillary, choroidal and retinal circulation and migraine [1, 25]. Therefore from the foregoing, there are associated factors with diagnosis NTG such as, female gender, hypotensive dips at nights in patients using antihypertensives at nights, migraine headache, Reynaud’s phenomenon, sleep apnea and thyroid disease [23]. Inability of the clinician to identify these factors may lead to misdiagnosis and progression of the disease to blindness. Identification of these factors in a given community will thus assist the eye care provider in planning and in the dissemination of evidence based health education to targeted community. This will help in early detention and prevention of blindness from the disease. Aim of the study is to identify the various characteristic factors associated with the diagnosis of NTG in patients presenting to the glaucoma clinic of a tertiary hospital.
Methods
All consecutive newly diagnosed glaucoma patients who attended the eye clinic of Ekiti state university teaching hospital, Ado Ekiti, from January 2012 to December 2014 were selected for the study. Approval for the study was obtained from the institution ethics and review board. All the patients had thorough ocular examinations; Visual acuity assessment with Snellen’s chart, slit lamp biomicroscope assessment of the anterior segment, intraocular pressure measured with Goldman applanation tonometer, central cornea thickness, colour vision test, optic disc stereoscopic evaluation with +78D lens, gonioscopy (with 4 mirror goniolens), central visual field test (24-2 and 10-2) taken minimum of 3 times of at least 4 months apart, and systemic examination particularly cardiovascular system. Examination and diagnosis were made by 2 ophthalmologists who had previously standardised their findings. The diagnosis of normal tension glaucoma was made based on the following criteria: A mean IOP equal to or less than 21 mm Hg on diurnal variation testing (DVT), with no pressure spikes greater than 24 mmHg, glaucomatous cupping of the optic nerve head with corresponding visual field defects, open angles on gonioscopy, absence of any possible contributing ocular or systemic disorder(s) and progression of glaucomatous damage. The patients with diagnosis of normal tension glaucoma had a protocol prepared for the study administered on them. Demographic data, family history of glaucoma, history of migraine, hypertension and use of antihypertensive drugs at night, history suggestive of sleep apnea were obtained from them. The Data were analysed using SPSS version 18 (Illinois, Chicago) and presented as tables, and figures, in frequencies, percentage and measure of association at p< 0.05.
Result
A total of 1265 patients were newly diagnosed to have glaucoma during the study period. Figure 1 showed that of these, 864(68.3%) were POAG, 336(26.6%) were secondary glaucomas, 48(3.8%) normal tension glaucoma, 12(0.9%) angle closure glaucoma and 5(0.4%) were developmental glaucoma. Among the NTG patients, 30(62.5%) were females and 18(37.5%) males,(F:M =1.7:1), (Table 1). Age range for NTG patients were between 30years to 75years, median age of 59.3years. Table 2 showed the identifiable associated factors in NTG patients include, family history of glaucoma 33(44%), hypertension and use of antihypertensives at night before sleep 24(32%), migraine headaches 10(13.3%), sleep apnea 6(8%), and thyroid disease 2(2.7%). Some of the subjects had more than one associated factor. 15 subjects had more than 1 associated factor; the factors are family history, use of antihypertensives at night and migraine headache. Table 3 showed the severity of visual field defect in NTG. In the multivariate analysis of associated factors with severity of visual field defect,none of the factors had statistically significant association with the severity of the visual field defect in NTG. p<0.05 (Table 4).
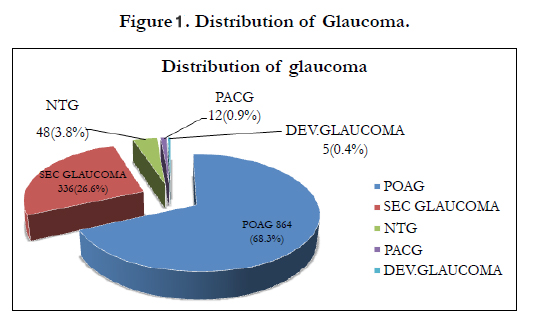
Figure 1. Distribution of Glaucoma.
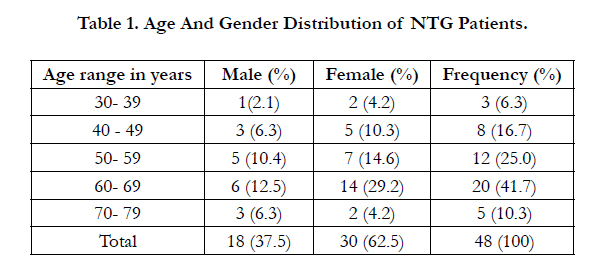

Table 1. Age And Gender Distribution of NTG Patients.
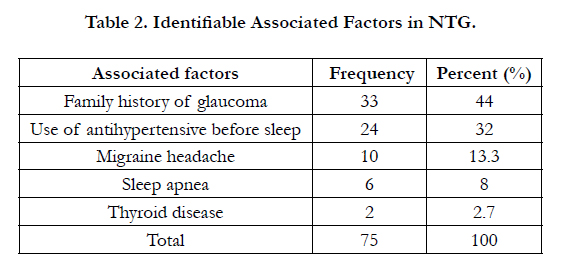
Table 2. Identifiable Associated Factors in NTG.
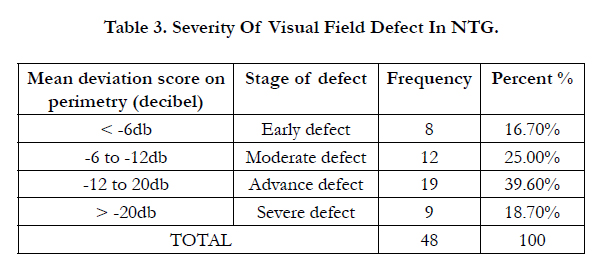
Table 3. Severity Of Visual Field Defect In NTG.
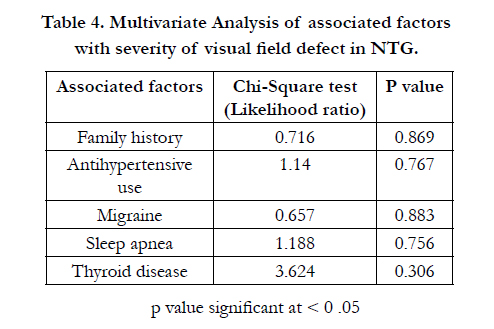
Table 4. Multivariate Analysis of associated factors with severity of visual field defect in NTG.
Discussion
The diagnosis of normal tension glaucoma needs not to be a herculean task for the clinician who is mindful of the various general, ocular and systemic factors associated with the disease. Every year as the World marks glaucoma week, efforts are made by various glaucoma societies and glaucoma care giver at creating awareness about the disease. A proportion of the populace desires to know the various associated factors that may predispose them to this cause of irreversible blindness. In our study, 1265 patients were newly diagnosed to have different forms of glaucoma presenting to the eye clinic, yet many are still undiagnosed in the community largely unaware of their having the disease or likelihood of having it. Of these newly diagnosed, majority, 864(68.3%) had POAG, this is similar to 73.4% reported by Enock in south east Nigeria [10], while Ashaye in Ibadan, south west Nigeria reported a slightly less value, 58.8% [2]. These differences may be due to the geographical as well as the socioeconomic setting of the hospitals where the studies were carried out.
In this study, normal tension glaucoma had a crude prevalence of 3.8% which is slightly higher when compared with 2% prevalence reported in Ethiopia [17]. Although this NTG prevalence rate appears to be small but it contributes to overall visual impairment and blindness burden of the society. The Beaver Dam Eye Study estimated the prevalence of normal-tension glaucoma to be up to 1.6% in patients over 75 years of age (15). Furthermore, females in this study have a slight preponderance over the male (1.7:1) and the age range was between 30 years to 75 years, with median age of 59.3 years. This was similar to reports by other authors [14, 15, 23] in the occurrence of NTG. The Tajimi eye study assessed the prevalence of POAG in patients over 40 years and found it to be 3.9%, in 92% the IOP was 21 mmHg or lower [12]. A nationwide survey in Japan estimated the normal-tension glaucoma with (IOP under 21mmHg) prevalence to be 3.5 times that of POAG, but these numbers are thought to be biased since normal IOP in Japan is lower than in the western population, averaging 10-18 mmHg. The prevalence of normal tension glaucoma is higher in women than in men [15]. Whatever the prevalence of normal tension glaucoma is in various populations, it is obvious that the numbers are higher than once assumed, and patients are sometimes diagnosed only when optic disc and visual field abnormalities are already present.
The management modalities of NTG are aimed at controlling IOP (a widely accepted factor in the progression of NTG) and other associated factors that may enhance disease progression. The Collaborative Normal Tension Glaucoma Study reported that aggressive IOP reduction of at least 30 percent from baseline levels reduced the extent of progressive visual field loss [9, 16]. In that study, therapy was initiated in patients with NTG with visual field loss threatening fixation, disc haemorrhage, and documented visual field or optic nerve progression. The results showed that aggressive IOP reduction with medications and/or surgery decreased the risk of progression from 35 percent to 12 percent over a five-year period [9].
A common initial approach in treating NTG is medical therapy [20]. It may be helpful to initiate a unilateral trial of the medication so that the contralateral eye can be used as a control to assess the drug's therapeutic and side-effect profile [20]. If medical therapy is insufficient and/or intolerable in reaching the target IOP level, laser trabeculoplasty may be considered. In certain instances, glaucoma filtering surgery is indicated to obtain IOP control. Use of antifibrotic agents such as mitomycin-C or 5-fluorouracil may improve the overall success rate of filtration surgery [11].
In clinical practice, control of IOP remains the mainstay of managing NTG patients, but consideration must also be given to other factors, especially those that may influence perfusion of the optic nerve head [22]. In our study, various associated factors were identified with family history of glaucoma having the highest frequency, followed by the use of antihypertensive at night before sleep and then migraine headache. It was also noted that some of the patients had more than one risk factor. These may suggest the possibility of more than one factor responsible for the development of the disease and may also contribute to the progression of the disease in an individual. This is similar to report by Ramli [21] that the nocturnal supine blood pressure parameters (systolic, diastolic and mean) and ocular perfusion pressure were significantly lower in the NTG group compared to ‘normals’. Moreover, increased incidence of migraine among patients with normal tension glaucoma, relative to patients with primary open angle glaucoma has been reported [5, 7]. Patients with obstructive sleep apnea/hypopnea syndrome (OSAHS) had a high prevalence of NTG, especially in patients with moderate and severe OSAHS. The severity of OSAHS inversely correlated with retinal nerve fiber layer thickness [16].
NTG is a disease entity in which non-ocular systemic abnormalities are believed to play a significant role in disease progression, optimization of potential IOP-independent factors, such as modification of a treatment regimen for systemic hypertension in order to alleviate nocturnal hypotension can be helpful in slowing the progression of their eye disease [3]. Therefore clinicians need to consider the possibility of glaucoma in patients with moderate and severe OSAHS [8]. Patients with NTG may be asymptomatic and present when they already have extensive visual field loss and optic nerve damage. A high index of suspicion is required for the diagnosis of the disease. In this study, the severity of NTG as shown by the mean deviation of the perimetry is seen in Table 3, Majority of these patients had advanced visual field defect. In patients with NTG, the optic disc rim may be significantly thinner, especially inferiorly and inferotemporally (compared to that observed in POAG patients) [4]. Optic disc haemorrhages and parapapillary disc atrophy (particularly in zone beta) may be observed in patients with NTG [24]. Moreover, the visual field defects tend to be more focal, deeper, and closer to fixation [6]. There are however no significant measure of association between the severity of the visual field defects and the associated factors seen in this study.
The consideration of the presence of these associated factors in these patients may further help the care giver in better diagnosis of NTG and most importantly target the society with health education based on the knowledge of these factors and eventually contribute to reduction of visual impairment and blindness.
Conclusion
This study suggests that age and positive family history of glaucoma are important demographic characteristics for consideration in diagnosis of NTG. These will be in conjunction with clinical findings such as disc haemorrhage, glaucomatous optic disc damage, characteristic visual field defect and intraocular pressure within normal range.
References
- Allingham RR, Damji K, Freedman S (2005) Shields' Textbook of Glaucoma. (5th edn), Philadelphia: Lippincott Williams & Wilkins 1: 197-216.
- Ashaye AO (2003) Clinical features of primary Glaucoma in Ibadan. Nigeria Journal of Ophthalmology 11(2): 70-75.
- Song BJ, Caprioli J (2014) New directions in the treatment of normal tension glaucoma. Indian J Ophthalmol 62(5): 529–537. doi: 10.4103/0301- 4738.133481.
- Caprioli J, Spaeth GL (1985) Comparison of the optic nerve head in highand low-tension glaucoma. Arch Ophthalmol 103(8): 1145-1149.
- Caprioli J (1998) The Treatment of normal tension glaucoma. Am J Ophthalmol 126(4): 578-581.
- Chauhan BC, Drance SM, Douglas GR, Johnson CA (1989) Visual field damage in NTG and high-tension glaucoma. Am J Ophthalmol 108(6):636-642.
- Collaborative Normal-Tension Glaucoma Study Group (1998) Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol 126(4): 487-497.
- Collaborative Normal-Tension Glaucoma Study Group (1998) The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Collaborative Normal-Tension Glaucoma Study Group. Am J Ophthalmol 126(4): 498-505.
- Corbett JJ, Phelps CD, Eslinger P (1985) The neurologic evaluation of patients with low tension glaucoma. Invest Ophthalmol Vis Sci 26(8): 1101- 1104.
- Enock ME, Omoti EA, Momoh RO(2010) Glaucoma in a Suburban Tertiary Care Hospital in Nigeria. J Ophthalmic Vis Res 5 (2): 87-91.
- Hitchings RA, Wu J, Poinoosawmy D, McNaught A (1997) Surgery for normal-tension glaucoma. Ophthalmology 104: 197-201.
- Iwase A, Suzuki Y, Araie M, Yamamoto T, Abe H, Shirato S, et al., (2004) The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology 111(9): 1641-1648.
- Kamal D, Hitchings R (1998) Normal tension glaucoma – a practical approach. Br J Ophthalmol 82(7): 835-840.
- Kanski JJ (2006) Normal tension glaucomas,Clinical Ophthalmology. (6thedn), Butterworth-Heinemann. 222-223.
- Klein BEK, Klein R, Sponsel WE, et al., (1992) Prevalence of glaucoma: The Beaver Dam eye study. Ophthalmology 99(10): 1499-1504.
- Lin PW, Friedman M, Lin HC, et al., (2011) Normal tension glaucoma in patients with obstructive sleep apnea/hypopnea syndrome. J Glaucoma 20(9): 553-558.
- Melka F, Alemu B (2006) The pattern of glaucoma in Menelik II Hospital Addis Ababa, Ethiopia. Ethiop Med J 44(2): 159-165.
- Mozaffarieh M, Flammer J (2013) New insights in the pathogenesis and treatment of normal tension glaucoma. Curr Opin Pharmacol 13(1): 43-49.
- Mroczkowska S, Benavente-Perez A, Negi A, et al., (2013) Primary Open- Angle Glaucoma vs Normal-Tension Glaucoma: The Vascular Perspective. JAMA Ophthalmol 131(1): 36-43.
- Orgul S, Zawinka C, Gugleta K, Flammer J (2005) Therapeutic strategies for normal-tension glaucoma. Ophthalmologica 219(6): 317-323.
- Ramli N, Nurull BS, Hairi NN, Mimiwati Z (2013) Low nocturnal ocular perfusion pressure as a risk factor for normal tension glaucoma. Prev Med 57(suppl): S47-S49.
- Shields MB (2008) Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol 19(2): 85-88.
- Tariq Farooq Babar, Muhammad Tariq Khan, Mir Zaman, Mohammad Daud Khan (2006) Normal Tension Glaucoma. Pak J Ophthalmol 22(2):60-67.
- Tezel G, Kass MA, Kolker AE, Wax MB (1996) Comparative optic disc analysis in normal pressure glaucoma, primary open-angle glaucoma, and ocular hypertension. Ophthalmology 103(12): 2105-2113.
- Wax MB, Barrett DA, Pestronk A (1994) Increased incidence of paraproteinemia and autoantibodies in patients with normal-pressure glaucoma. Am J Ophthalmol 117(5): 561-568.





