Anatomical Variations of Aortic Arch Branching Pattern Among the Chinese
Zhang Y1*, Kaka A.K. Katiella1, Wang li2, Zhang H3, Afzal F4, Sun H1, Xing YH1
1 School of International Education Zhengzhou University, Zhengzhou-Henan, P.R.China.
2 Department of Interventional Radiology Zhengzhou University, Zhengzhou-Henan, P.R.China.
3 Department of Orthopaedics Zhengzhou University, Zhengzhou-Henan, P.R.China.
4 Department of Obstetrics and Gynaecology-Fourth Affiliated Hospital Zhengzhou University, Zhengzhou-Henan, P.R.China.
*Corresponding Author
Zhang yanru, Ph.D,
Associate Professor, Research Direction, Nerve Regeneration, Director Anatomy Department,
School of International Education, Zhengzhou University, Zhengzhou-Henan, P.R.China.
Tel: (+86)155-14521367
Fax: (+86)0371-66658656
E-mail: jiaoxueban2010@126.com
Received: June 14, 2016; Accepted: June 24, 2016; Published: June 30, 2016
Citation: Zhang Y, et al., (2016) Anatomical Variations of Aortic Arch Branching Pattern Among the Chinese. Int J Anat Appl Physiol. 2(4), 43-48. doi: dx.doi.org/10.19070/2572-7451-160007
Copyright: Zhang Y© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Either from congenital or ischemic problems, difficulties in aortic bypass surgery are usually caused by the unrecognized variation of aortic arch anatomy.Objective: To investigate the frequency and anatomical basis of the aortic arch branching pattern from the world largest hospital.
Materials and Methods: Thirty eight adult human preserved cadavers, and one thousand fifty three aortic arches analyzed from images of computerized tomography and aortic angiography were used. Occurrence among gender, branching pattern of the aortic arch was studied; number of branches and distance from their origin to the mid-vertebrae line were measured.
Results: In 81.3% of the cases, the main most common brachiocephalic trunk, left common carotid and left subclavian artery originate independently. From the remaining variants of the aortic arch: 13.2% have two branches, an independent left subclavian artery and a common trunk for the brachiocephalic trunk and left common carotid. 4.8% has four branches with the left vertebral artery; 0.4% having the left common carotid artery originating from a common trunk. Any other variation falls within 0.1%. However, a strong significant positive correlation was found between the diameters of left common carotid artery and left subclavian artery.
Conclusion: The results in this study provide accurate information on aortic arch variations considered vital for academic purpose, and clinical vascular surgery and a primary data among the Chinese.
2.Introduction
3.Materials and Methods
3.1.Computer Aided Tomography Images
3.2.Statistical analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgments
8.References
KeyWords
Aortic Arch; Anatomical Variations; Branching Pattern; CT Scans; Academics; Chinese.
Introduction
From the arch of aorta (AA) arise most commonly three branches known from right to left as follows: (i) the brachiocephalic trunk (BT), (ii) the left common carotid artery (LCA), (iii) the left subclavian artery (LSA) as reported most workers. This pattern occurs in 65-80% of the cases [5,20]. The final configuration of the AA and its branches is probably related to the associated “migration” and “merging” of the branches, together with the different growth rates in the various arteries [15]. Nevertheless, the aortic arch is a challenging site for endovascular repair [8]. Anomalies of AA are also associated with chromosome 22q11 deletion [21]. Different variations concerning the origin and number of the branching pattern of the AA of its major branches were considered as normal variants [8]. The anatomic and morphologic variations of the AA and its branches are significant for diagnostic and surgical procedures in the thorax and neck [16]. With advances in technology, a patient could be operated either for a graft, a total arch replacement, a bypass or survive under stenosis of the AA (or of any of its branches). But techniques remain costly or not easily performed. Some abnormalities are discovered after operation [17], some stay unknown to the subjects due to financial problems or some, until studied on cadavers without a known history in the cause of death. Internal cerebrovascular injury still stays a cause of death and tough to be managed. Despite unpredictable complications, the use of stent through the brachial artery or the femoral artery is the main techniques used to avoid open chest surgery, but requires a well experienced surgeon.
Materials and Methods
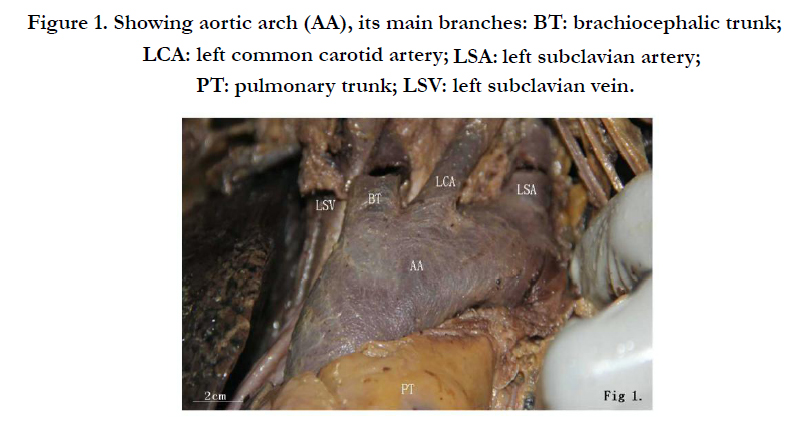
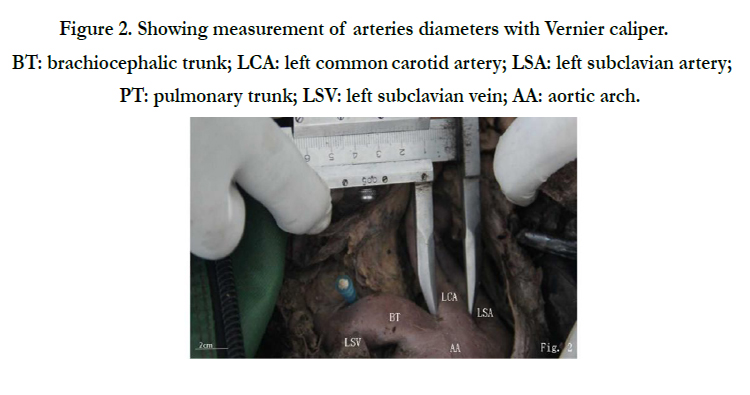
The study was approved by Zhengzhou University Institutional Review Board Committee and it followed strictly the principles outlined in keeping any reference to subjects or cadavers records confidential. It was performed on preserved thirty and eight adult human cadavers of both genders (Department of Anatomy, School of International Education); and one thousand and fifty three computer aided tomographic images (Department of Cardiac Surgery, First affiliated Hospital). Among the thirty and eight cadavers; eighteen were carefully dissected in the year 2013-2014, and twenty in the year 2014-2015 academic calendars. The thoracic cavity was completely open dissected and reflected antero-inferiorly, following the instructions from the Text book of Regional Anatomy Fifth Edition by Wang Huaijing and Liu Yong, and the Cunningham’s Manual of Practical Anatomy-Volume three, Fifth Edition by G.J. Romanes. In these dissected cadavers, pericardium was opened, fat and if any blood clots were cleaned, and aortic arch and its main branches [brachiocephalic trunk (BT), left common carotid artery (LCA), left subclavian artery (LSA)] exposed (Figure 1); their diameters and mid vertebral line distance measured, then hearts removed. There after, the complete respiratory tree was removed, assessed the vertebral arteries, the thoracic aorta and or any arising branch from the aortic arch or proximal thoracic aorta. Measurement of the diameters at the site of arteries’ origin from the AA was done using a Vernier caliper, accuracy 0.1 mm. (Figure 2). Photographs were taken using digital camera (Canon EOS-60D).


CT-images were conducted in Software for navigating in multidimensional DICOM images OsiriX MD®. Technology of 3D reconstruction surface of axial image to expose the variations in the aortic arch. CT can identify normal and abnormal structures, making it useful tool to guide radiotherapy, needle biopsies, and other invasive procedures. All protocols are respected as described by Alper (2013) [2]. Typically between 75 ml to 150 ml (about 2.5 oz. to 5 oz) of contrast is used depending upon the patient's age, weight, area being imaged and cardiovascular health.
Data were analyzed using SPSS software version 21.0 and significance set at value of P < 0.05. The study included computerized tomography images (Enhanced CT scan images) from patients with different purposes.
Results
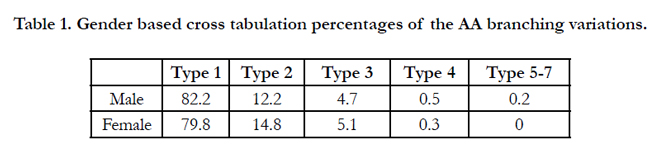
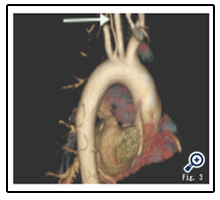
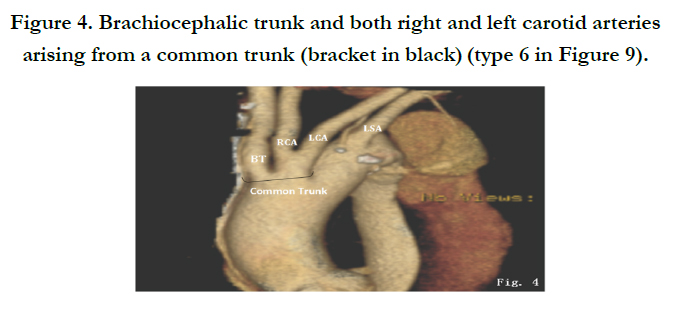
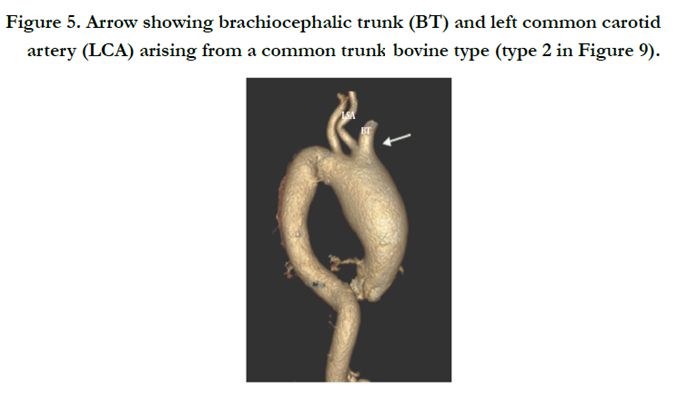
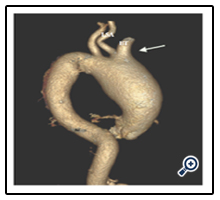
For any cardiac surgery, 3D computed tomography scanning has nowadays become core prior to intervention. Aortic arch branching pattern is usually detected and addressed; or in the other hand detected during dissection classes. In all subjects included in this study, no case of dextrocardia was recorded. All aortic arches studied have anatomically normal arising pattern from the left ventricle, antero supero-lateral to the right from the left atrium, arching backwards and towards the left side lateral to the trachea. It curves over the pulmonary trunk. Inferiorly the left recurrent laryngeal nerve takes its upward curve. The AA continues as thoracic aorta roughly from the level of the fourth to the twelfth thoracic vertebra. The left surface of the arch was crossed by the left phrenic nerve and pericardiacophrenic vessels. The right posterolateral surface was related to trachea, and the vertebral column. Figures 3; 4 and 5 show the CT scan outcomes of few variations.
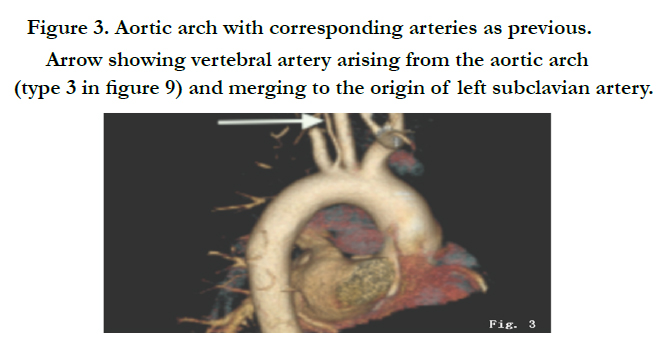
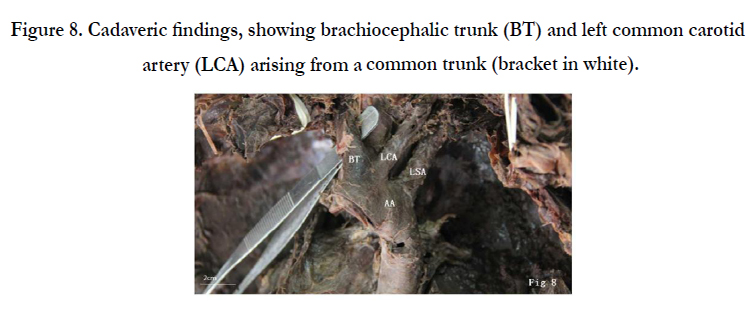
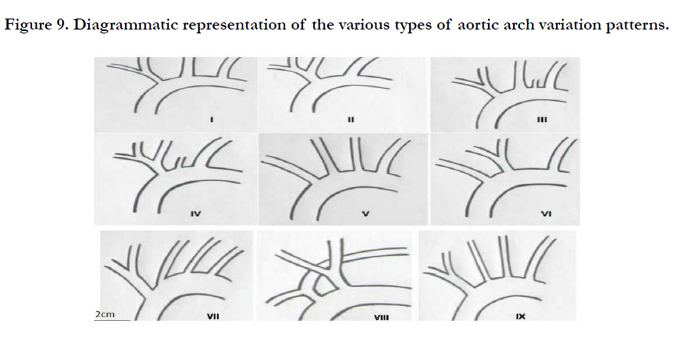
In this study the gender repartition of AA branching pattern is shown in Table 1 below, and only one variation (Figure 8 or type II in Figure 9) was encountered from the cadavers.


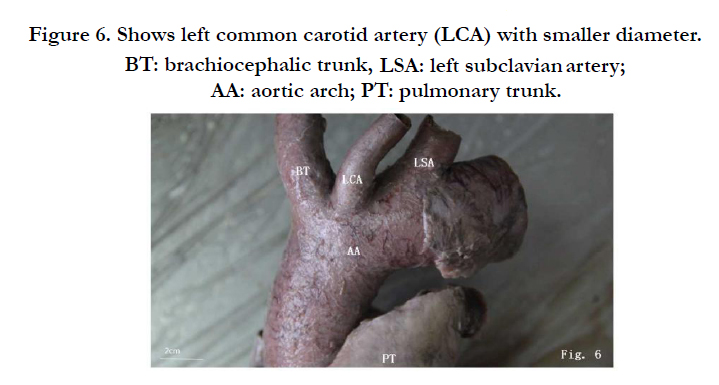

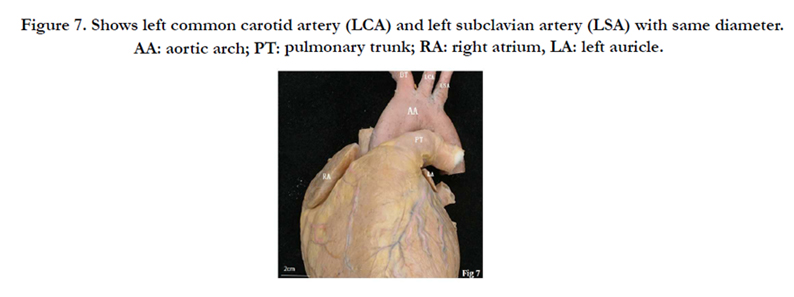

Overall in 81.3% of the cases the main common brachiocephalic trunk, left common carotid and left subclavian artery originated independently (Figure 2). Others variant proportions on the aortic arch are: 13.2% have two branches, an independent left subclavian artery and a common trunk for the brachiocephalic trunk and left common carotid. 4.8% has four branches with the added left vertebral artery; 0.4% having the right and left common carotid arteries originating from a common trunk. Any other variation falls within 0.1%. However, a strong significant positive correlation was found between the diameters and mid vertebral line distance of left common carotid artery and left subclavian artery (Table 2).
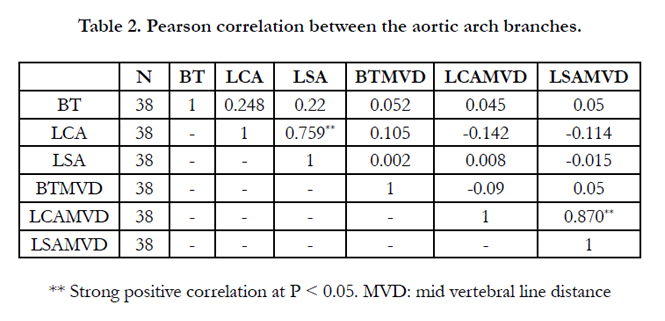

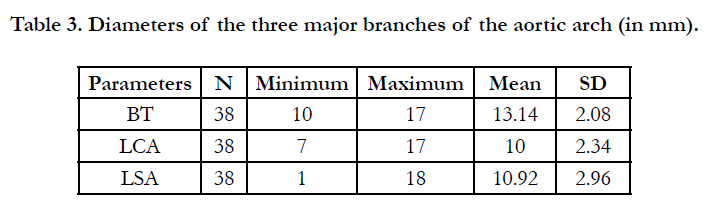
The mean diameter of the BT was 13.14 ± 2.08 mm while the mean mid vertebral line distance was 10.90 ± 3.61 mm. The mean diameter of LCA was 10.00 ± 2.34 mm and its mean distance to the mid vertebral line was 20.16 ± 5.70 mm. A negative correlation of r = -0.142; -0.114 was respectively found for the LCA, LSA to mid vertebral line (Table 3).
Percentage of age distribution prevalence among the subjects was 4.2% in male vs 3.3% in female at the age of 52 years; while it is 4.6% in female vs 1.5% in male at the age of 58 years.
The correlation of the left common carotid artery and the left subclavian artery was of P < 0.001 while the correlation between the other parameters and to the mid vertebral line was not significant. From the total descriptive statistics, the minimum age of the subject was 18.00, maximum 89.00 and the mean standard of deviation was 52.96 ± 14.39 years (Table 2 above). Figure 9 below represent all types of branching patterns so far described by many authors and to which we gradually made correlations in this study.
Discussion
Detection of the anomalous origins of the branches of the AA is attributed to the altered development of certain brachial arch arteries during the embryonic period of gestation [16]. In this study, the three major branches of the AA originated independently in 81.3% of the cases. This corresponds to Type I variation (Type A in Figure 9). This finding is similar to previous studies where 70% [4,8,13]; 84% [21] and 65% [18] of patients were reported to have this common branching pattern. Not with standing, the current study showed that the Type 5, 6, and 7 variations were found each one to be of same 0.1%. Type 2 [11] and the rarest Type 8 as shown in Figure 9 and Type 9 [19] were not encountered. Still, incidentally in a CT arch aortography, five branches originated directly from the AA in which an anomalous origin of both vertebral arteries originated beyond the left subclavian artery [22]. However, the approximation of the LCA to the BT is an important observation while invading the AA and its branches with instruments, since all cases are susceptible to surgical attack [6]; but in this study we found it rather for LCA and LSA. Also, in a study on hundred cadavers, the mean transverse distances between adjacent luminal openings of BT, LCA and LSA were found significantly greater than the mean vertical distances (P < 0.001) [7]. They also observed that approximation of LCA to BT trunk was seen in 10.0% specimens. Compared to the results of Shin et al. (2008) [21] who found the mean diameter of the BT, LC and LS respectively been 17.97 ± 3.85 mm, 9.77 ± 1.91 mm, and 14.33 ± 3.09 mm, in this study the values were 13.14 ± 2.08 mm; 10.92 ± 2.34 mm; 10.00 ± 2.96 mm respectively. Genetic, environmental and social factors might have an effect on these deviations. We also found a branching artery from the LCA in one cadaver (0.38%). While the vertebral artery may have duplicate origin from the arch and the subclavian artery [12] as shown in Figure 3 of this study. Supporting the present results (4.7% in male, 5.1% in female), the most frequent variant (2.4-5.8% from their study) is the LVA, arising directly from the AA between LCA and LSA [3,19]. It was reported a case in which RVA originated directly from the aortic arch [16] while another study found in eight cases that the variant of the RVA originating from the AA was distal to the LSA [9]. For the aberrant origin of the LVA directly from the AA is due to persistence of the 8th intersegmental artery [1]. Although many authors reported variations of AA in different populations; the presence of a similar incidence of variation in two closely located populations such as Turks and Greeks may suggest a relationship between the incidence of aortic arch variations and ethnicity [2]; but our result disagrees with these findings. Although the absence of truncus brachiocephalicus and origination of right subclavian artery and right common carotid artery directly from the aortic arch (Type 7 in Figure 9) was first described in the 18th century [5]. They conclude in their study that variations in branching pattern of arcus aorta which have an incidence of 14.7 % are common, and most of them have no clinical importance. The latter and this study are in line with the study of Marital and Chad (2001) [14]. Insight to genetic background and congenital abnormalities will be more helpful [10].
Conclusion
Common among Chinese, recognition of the variations of the aortic arch branching pattern is relevant because of tracheoesophageal compression or complications (in case of stenosis, occlusion or accident) during surgical or endovascular interventional procedures; or help determine risk factors or advantages in bypass procedures. However, variations in AA branching patterns are quite safe for the patients’ life span, but the knowledge of the morphology are necessary for thoracic surgeons, for academic and professional awareness, and in the understanding of clinical conditions. Currently, CT scan stays still the best safe approach to get the 3D-image of the circulatory system in general for a better surgical procedure. Rare are the books in clinical anatomy addressing these anatomical variations supported by fine images and the knowledge staying more clinical, create the surprise of students during dissection classes. It will be helpful that genetic studies be carried out for a better understanding of human anthropology and efficient clinical management.
Acknowledgments
We are thankful to the Department of Cardiac Surgery and Department of Interventional Radiology for all the CT-scans provided.
References
- Albayram S, Gailloud P, Wasserman BA (2002) Bilateral arch origin of the vertebral arteries. AJNR Am J Neuroradiol 23(3): 455-458.
- Karacan A, Türkvatan A, Karacan K (2013) Anatomical variations of aortic arch branching: evaluation with computed tomographic angiography; Cardiology in the Young. 24(3): 485-493.
- Best IM, Bumpers HL (2002) Anomalous origins of the right vertebral, subclavian, and common carotid arteries in a patient with a four-vessel aortic arch. Ann Vasc Surg 16(2): 231-234.
- Bhatia K, Ghabriel MN, Henneberg M (2005) Anatomical variations in the branches the human aortic arch: a recent study of a South Australian population. Folia Morphol (Warsz) 64(3): 217-223.
- Ergun E, Şimşek B, Koşar PN, Yılmaz BK, Turgut AT (2013) Anatomical variations in branching pattern of arcus aorta: 64-slice CTA appearance. Surg Radiol Anat 35(6): 503–509.
- Goray VB, Joshi AR, Garg A, Merchant S, Yadav B, Maheshwari P (2005) Aortic archvariation: a unique case with anomalous origin of both vertebral arteries as additionalbranches of the aortic arch distal to left subclavian artery. AJNR Am J Neuroradiol 26(1): 93-95.
- Gupta M, Sodhi L (2005) Variations in branching pattern, shape, size and relative distances of arteries arising from arch of aorta. Nepal Med Coll J 7(1): 13-17.
- Haifa A. Alsaif, and Wafaa S. Ramadan (2010) An Anatomical Study of the Aortic Arch Variations. JKAU Med Sci 17(2): 37-54. DOI: 10.4197/Med.17-2.4.
- Karcaaltincaba M, Strottman J, Washington L (2003) Multidetector-row CT angiographic findings in the bilateral aortic arch origin of the vertebral arteries. AJNR Am J Neuroradiol. 24(1): 157.
- Natsis KI, Tsitouridis IA, Didagelos MV, Fillipidis AA, Vlasis KG, Tsikaras PD (2009) Anatomical variations in the branches of the human aortic arch in 633 angiographies: clinical significance and literature review. Surg Radiol Anat 31(5): 319–323.
- Layton KF, Kallmes DF, Cloft HJ, Lindell EP, Cox VS (2006) Bovine Aortic Arch Variant in Humans: Clarification of a Common Misnomer. AJNR Am J Neuroradiol 27(7): 1541-1542.
- Lemke AJ, Benndorf G, Liebig T, Felix R (1999) Anomalous origin of the right vertebral artery: review of the literature and case report of right vertebral artery origin distal to the left subclavian artery. AJNR Am J Neuroradiol 20(7): 1318-1321.
- Lippert H, Pabst R (1985) Aortic arch. In: Arterial Variations in Man: Classification and Frequency. Munich, Germany. JF Bergmann-Verlag 3–10.
- Nelson ML, Sparks CD (2001) Unusual Aortic Arch Variation: Distal Origin of Common Carotid Arteries. Clinical Anatomy 14(1): 62–65.
- Mligiliche NL, Isaac ND (2009) A three branches aortic arch variant with a bi-carotid trunk and a retro-esophageal right subclavian artery. IJAV 2: 11–14.
- Momma K, Matsuoka R, Takao A (1999) Aortic arch anomalies associated with chromosome 22q11 deletion (CATCH 22). Pediatr Cardiol 20(2): 97-102.
- Nayak SR, Pai MM, Prabhu LV, D’Costa S, Shetty P (2006) Anatomical organization of aortic arch variations in the India: embryological basis and review. J Vasc Bras 5(2): 95-100.
- Paraskevas G, Agios P, Stavrakas M, Stoltidou A, Tzaveas A (2008) Left common carotid artery arising from the brachiocephalic trunk: a case report. Cases J 1(1): 83.
- Schwarzacher SW, Krammer EB (1989) Complex anomalies of the human aortic arch system: unique case with both vertebral arteries as additional branches of the aortic arch. Anat Rec, 225(3): 246-250.
- Shakeri A, Pourisa M, Deldar A, Goldust M (2013) Anatomic variations of aortic arch branches and relationship with diameter of aortic arch by 64-row CTangiography. Pak J Biol Sci 16(10): 496-500.
- Shin Y, Chung Y, Shin W, Im S, Hwang S, Kim B (2008) A morphometric study on cadaveric aortic arch and its major branches in 25 Korean adults: the perspective of endovascular surgery. J Korean Neurosurg Soc 44(2): 78-83.
- Suzuki K, Kazui T, Bashar AH, Yamashita K, Terada H, Washiyama N, Suzuki T (2006) Total aortic arch replacement in patients with arch vessel anomalies. Ann Thorac Surg 81(6): 2079-2083.





