Tinnitus - Characteristics and Therapy
Zofia A. Dziuganowska
Department of Bioorganic Chemistry, Faculty of Chemistry, Wrocław University of Technology, Wybrzeże Wyspiańskiego, Wrocław, Poland.
*Corresponding Author
Zofia A. Dziuganowska,
Department of Bioorganic Chemistry,
Faculty of Chemistry, Wrocław University of Technology,
Wybrzeże Wyspiańskiego 27, Wrocław, 50-370, Poland.
E-mail: zofia.a.dziuganowska@gmail.com
zofia.a.dziuganowska@pwr.edu.pl
Received: December 11, 2015; Accepted: January 29, 2016; Published: February 03, 2016
Citation: Zofia A. Dziuganowska (2016) Tinnitus - Characteristics and Therapy. Int J Bioorg Chem Mol Biol. 4(2):17-23.DOI : dx.doi.org/10.19070/2332-2756-160003
Copyright: Zofia A. Dziuganowska© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Many papers have been published so far that the need for an updated review prompted the author to write this article and to describe historical perspective, characteristics, epidemiology, causes, pathophysiology, and treatments of tinnitus.Despite of the common opinion,this one of the most annoying of ear disorders, has been known from the Antiquity. Nowadays, it touches about 11% of population of Western Europe. Tinnitus, as the complex symptom, is associated with other annoying ear disorders.While indication of its reason is very often impossible, the factors contributing to the development of disorder were determined. Several theories explaining the mechanism of tinnitus have showed that extensive levels of nervous system may be involved in its generation. Although no convincing treatment is available, some alleviating therapies are recommended. They can be divided into two categories: relieving of its severity and reduction of its intensity.
2.Tinnitus from Historical Perspective
3.Characteristics of Tinnitus
3.1.Definition and Description
3.2.Accompanying ailments
3.3.Epidemiology of tinnitus
3.4.The causes of tinnitus
3.5.Pathophysiology of tinnitus
4.Treatment of Tinnitus
4.1.Pharmacotherapy
4.2.Non-pharmacological therapies
5.Conclusion
6.References
Keywords
Tinnitus; Characteristics; Causes; Mechanisms; Therapy; Pharmacology.
Tinnitus from Historical Perspective
The origin of a name of a disorder derives from the Latin word “tinnire” that means “to ring” and in this context is defined as “ringing in the ear”. Tinnitus – on the contrary to the common opinion – is the disorder known from the Antiquity. According to some authors [1], the first reference to tinnitus can be found in the Ebers Papyrus dated back to the 17th Egyptian dynasty (1650-1532 B.C.) where it was defined as ‘bewitched ear’. Tinnitus was not always treated as disease:ancient Indians recognized it as a sign of communion with space reserved only to spiritual elite; ancient Egyptians as a gift for divination; other civilizations considered it as Titus’s curse– one of the most severe mythical punishments put on humanity [2]. The first undisputed reference to tinnitus was found in Corpus Hippocraticum where it was claimed that symptom is connected with hearing loss, headache and menstruation disorders.
These annotations did not only concern the description of the disease but also methods of its treatment. Three methods were used: fumigation involving a variety of substances deriving from trees, herbs, sometimes even animal materials (bones or horns); insertion of wool treated with various materials into ears; direct administration of drugs to ear via a bronze tube [3]. Various materials such as honey, vinegar, rose oils, laurel oil etc. were applied. Galen (130-200 A.D.) used, as the first, sedatives like opium or mandrake juice in order to dull the brain’s response to tinnitus. Therapy of tinnitus changed in the Renaissance when Paracelsus introduced first mineral-based drugs. Later, the more advanced techniques such as surgeries (beginning of 17th century), electric stimulations (second half of 18th century) or acoustic stimulation (middle of 19th century) were developed.
Characteristics of Tinnitus
Tinnitus is defined as phantom auditory perception [4]. This broad definition includes the auditory hallucinations of schizophrenia, a variety of somatosounds such as palatal myoclonus, abnormal opening or patency of the Eustachian tube, temporomandibular joint disease, spontaneous otoacoustic emissions and sounds of vascular origin as well as sensation resulting from a malfunction of the cochlea or auditory nerve. Tinnitus can be classified as objective or subjective. Objective tinnitus can be heard by an observer and, what is more, it can be measured by means of appropriate equipment. Subjective tinnitus is heard only by the sufferer. Nowadays, objective tinnitus is treated as somatosounds.
Such classification simplified diagnosis and allowed proposing one definition of disorder as “the perception of sound that results exclusively from activity within the nervous system without any corresponding mechanical, vibratory activity within the cochlea, and not related to external stimulation of any kind” [5].
Sufferers describe the sound related to tinnitus as similar to cicadas, crickets, winds, falling trap water, grinding steel, running engines, escaping steam and etc. Most patients match their tinnitus to a pitch above 3 kHz. However, tinnitus associated with Ménière’s disease is usually low-frequency tone from 125 to 250 Hz [6].
Tinnitus is often associated with other annoying symptoms such as decreased sound tolerance, hyperacusis (an abnormally strong reaction to sound occurring within the auditory pathways), phonophobia (a fear of certain sounds) and misophonia (the aversion to sounds). Moreover, it frequently coexists with hearing loss or Ménière’s disease.
Tinnitus has also influence on mental condition of sufferers as it causes stress, annoyance, anxiety or even depression [7]. It also increases difficulties in concentration and decreases the quality of sleep [8].
The epidemiological studies of tinnitus are difficult because of very broad definition of disorder. Furthermore, this subjective perception differs from patient to patient what makes preparation of questionnaire very complicated.
Tinnitus has become the public health problem. It touches about 10% of population in Great Britain, 14.2% in Sweden, 8.4% in USA, 15.1% in Norway [9], 13% in Germany [10], 8% in France [11] and 20.1% in Poland [12] (Figure 1).
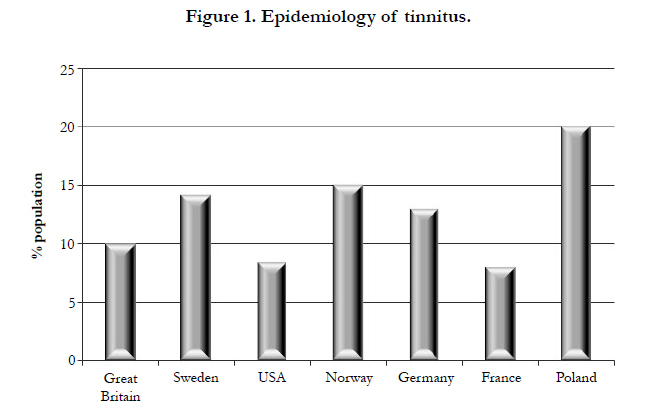
Figure 1. Epidemiology of tinnitus.
The frequency of occurrence of tinnitus increases with age as about 18% of population older than 70-years old suffer from this ailment [13]. The disorder was also observed in children and youngsters when the percentage of patients varied from 7% to 34% of population of this age group [14].
While indication of the reason of tinnitus is very often not possible, the factors contributing to the development of disorder were determined. The major causes are accumulated noise exposure, acoustic trauma [15] and age-related changes [16]. The other disorders which can provoke it are: occlusion of the ear canal, external, middle ear and internal ear otitis, cholesteatoma, otosclerosis, Ménière’s disease, alteration in blood flow, barotrauma and head trauma [17]. Vestibular schwannoma [18], microvascular compression of the vestibulocochlear nerve [19] and cerebrovascular diseases [20] also can lead to tinnitus. The other factors are jaw and neck disorders or temporomandibular joint dysfunction [21].
Tinnitus can be also a side effect of taking some medicines, for example analgesics like salicylates and non-steroidal antiinflammatory agents. Moreover, the use of antibiotics such as aminoglycosides (gentamycin, streptomycin and neomycin), erythromycin, azithromycin, vancomycin, tetracycline and chloramphenicol evokes tinnitus. It can be the side effect of treatment with antineoplastic agents (bleomycin, cisplatinum, methotrexate and vincristine), loop diuretics (bumetanide, ethacrynic acid and furosemide), tricyclic antidepressants (amitryptylline, doxepin and imipramine) and quinine or chloroquine [22]. Finally, severe stress also causes tinnitus [6].
Tinnitus is the complex symptom, therefore,extensive levels of nervous system can be involved in mechanism of its generation.
At the beginning, tinnitus was treated as spontaneous otoacoustic emissions. They are small acoustic signals which appear in the ear canal when tympanic membrane received vibrations from cochlea [6]. However, since spontaneous acoustic emissions can be measured by means of special equipment, thus, they cannot be treated as tinnitus.
The discordant dysfunction/damage theory proposes the other mechanism of generation of tinnitus [5]. The discordant damage of sensory cells in the mammalian auditory epithelium (one type of sensory cells – outer hair cells - is more dysfunctional than the other type of sensory hair cells – inner hair cells) leads to deregulation of sound transduction.This results in abnormal activity within the auditory pathways that can cause tinnitus.
Generation of the symptom can be also the result of hyperactivity of dorsal cochlear nucleus [23]. Interestingly, neuroimaging techniques showed that reorganization of the auditory cortex, caused by head or cochlea injuries, relates to tinnitus [24, 25]. Cross-talk theory postulates that disease can be the effect of spontaneous activity of auditory neurons connected by artificial synapses (called “crosstalk”) that could be formed after damage of auditory nerve fibers [6].
The alternative mechanism concerns alterations of intracellular Ca2+ concentration. Cytosolic concentration of Ca2+ affects electromotility, therefore sensitivity of outer hair cells. Thus, any abnormality in Ca2+ concentration may cause deregulation of proper functioning of outer hair cells (the cochlear amplifier) that may evoke tinnitus of cochlear origin [26].
Tinnitus may be also caused by anomalies in neurotransmission in inner hair cells [27]. Glutamate and aspartate (Figure 2)imitate the effect of acoustic stimulation by increasing the spontaneous activity of neurons of auditory nerve. Two classes of glutamate receptors ionotropic (ligand gated ion channels) and metabotropic (G-protein coupled) ones are related to this mechanism.
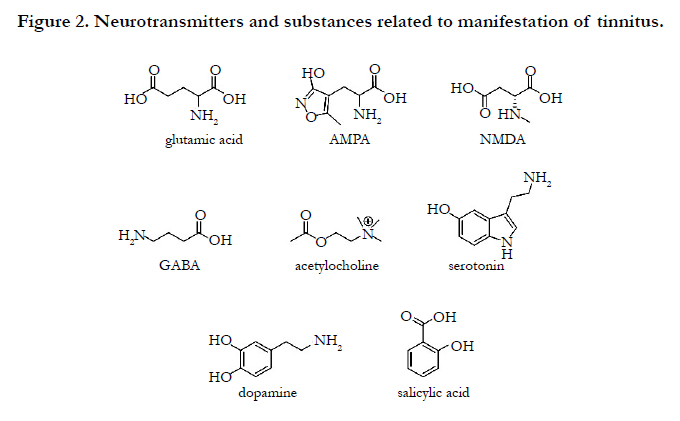
Figure 2. Neurotransmitters and substances related to manifestation of tinnitus.
The expression of AMPA (α-amino-3-hydroxy-5-methyl-4- isoxazolepropionate) (subunits: GluA2-4) and kainate (subunits: GluK1-3, previous nomenclature GluK5-7) receptors in auditory nerve cells is well acknowledged [28] (Figure 2). AMPA receptors are responsible for high AMPA, kainate and glutamate excitotoxicity. AMPA and kainate cause acute destruction of dendrites of neurons of the auditory nerve. The other group of ionotropic glutamate receptors, NMDA (N-methyl-D-aspartate) (Figure 2) receptor (subunits: GluN1, GluN2B, GluN2C, GluN2D), is also expressed in auditory nerve [29]. Behavioral tests on animals, later confirmed by electrophysiological studies, showed that while salicylate, which induces tinnitus, increases the activity of NMDA receptors, NMDA antagonist blocks this effect [30].
Metabotropic glutamate receptors are also expressed in the cochlea. Although their role still remains unknown [27], they have influence on activity of neurons and they are related to the soundevoked suppression of neuronal firing in the auditory system [31].
The mechanism of generation of tinnitus is also connected with the activity of GABA (γ-aminobutyric acid)(Figure 2) receptor [32]. Behavioral tests showed that GABA agonist attenuates chronic noise-induced tinnitus. Other studies on animals with induced tinnitus indicated modifications in the activity of choline acetyltransferase and cholinergic receptors in the cochlear nucleus [33].
The mechanism of manifestation of tinnitus can be also related to dysfunction of serotonin (5-HT) (Figure 2) at one or more levels in the central nervous system [34]. Tinnitus activates the same cerebral structures as dopaminergic pathways, therefore substances active towards dopamine receptors may also effect on its severity [35].
The neurophysiological model of tinnitus, although it does not explain the mechanism of its generation, postulates that apart from the auditory system, the number of other systems in brain are involved in its manifestation [5]. Moreover, it emphasizes interactions between the auditory system and emotional (limbic) and autonomic nervous system.
Treatment of Tinnitus
The methods of treatment of tinnitus can be divided into two categories: relieving of its severity and reduction of its intensity. Cognitive behavioral therapy, sound therapies, Tinnitus Retraining Therapy, hearing aids, massage and stretching belong to the first group while electrical or magnetic stimulation and surgeries to the second one. Pharmacotherapy can be included in both categories.
Pharmacotherapy of tinnitus differs depending on its type. Despite various approaches to the treatment of the symptom, FDA (Food and Drug Administration) or EMA (European Medicine Agency) [36-37] have not yet approved any drug.
One of effective substances is lidocaine (Figure 3), a local anaesthetic and anti-arrhythmic agent [38]. Given intravenously or by intratympanic administration, lidocaine results in the temporary disappearance of tinnitus or major change in its severity in 70% of patients. However, because of its significant side effects, lidocaine is no longer used.
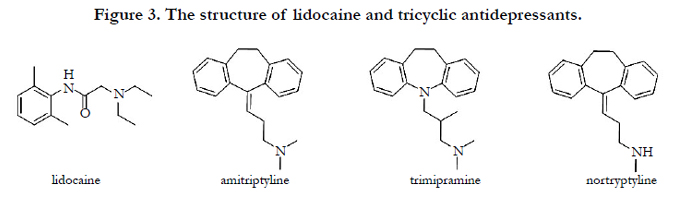
Figure 3. The structure of lidocaine and tricyclic antidepressants.
Although some antidepressants provoke tinnitus, the other ones are commonly prescribed for its treatment [39]. Among tricyclic antidepressants (Figure 3)- amitriptyline, trimipramine and nortriptyline – only nortriptyline decreases both tinnitus and depression. However, it is less effective in case of non-depressive patients.
The activity of selective serotonin reuptake inhibitors – paroxetine and sertraline was also investigated towards tinnitus(Figure 4). While sertraline reduces its loudness and severity, the combination of paroxetine with vestipitant (neurokinin-1 receptor P substance antagonist) or vestipitant alone are even more effective and thus they undergo clinical trials [40].
Benzodiazepines, allosteric modulators of the GABAA receptor, were also considered as the treatment for tinnitus [41]. Clonazepam (Figure 4) significantly decreases tinnitus symptoms in 32% of patients. However, treatment with benzodiazepines is restricted because of high risk of drug addiction.
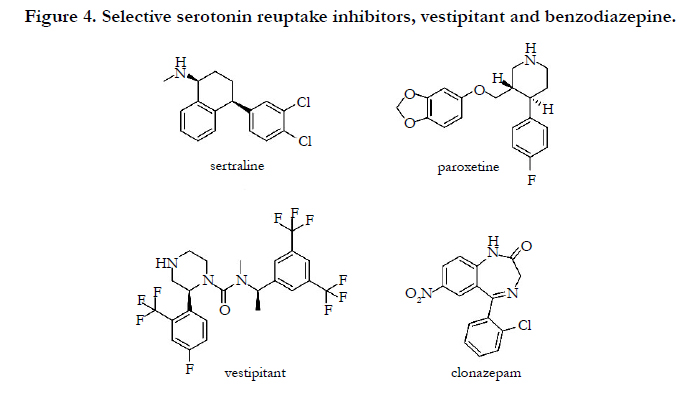
Figure 4. Selective serotonin reuptake inhibitors, vestipitant and benzodiazepine.
As it was mentioned, tinnitus may be caused by overstimulation of glutamate receptors, exactly NMDA receptors. Behavioral studies showed that NMDA receptor antagonists such as ifenprodil [42], MK-801 (dizocilpine), 7-chlorokynurenate and gacyclidine (Figure 5) [30] reduce its occurrence.
Therefore, the activity of many NMDA antagonists has been also investigated. Among them, acamprosate, which acts both on NMDA (as antagonist) and GABA receptors (as agonist), decreases the severity of the symptom in more than 80% of patients [43]. The other NMDA and nicotinic acetylcholine receptor antagonist, neramexane, is effective and undergoes III phase of clinical trials [44] (Figure 5). Gacyclidine, earlier mentioned compound, is also regarded as potential drug against tinnitus [45-46].
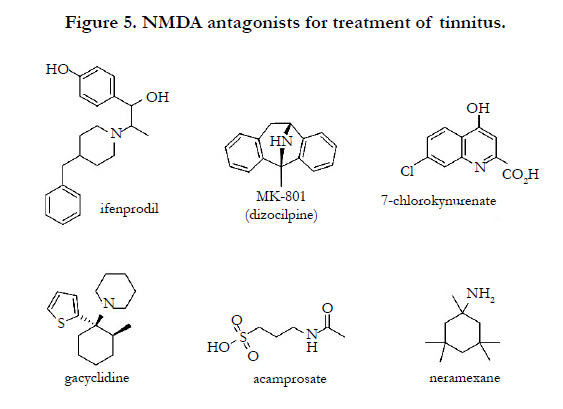
Figure 5. NMDA antagonists for treatment of tinnitus.
Compounds active towards dopamine receptors (Figure 6) were also proposed for the treatment of tinnitus [40]. A double-blind placebo-controlled study indicated that sulpiride significantly decreases its severity. Moreover, combination of sulpiride with hydroxyzine or melatonin intensifies the effectiveness of the treatment. The combination of the other compounds from this category, flupenthixol with clonazepam, is as active as clonazepam alone and is already during clinical trials.
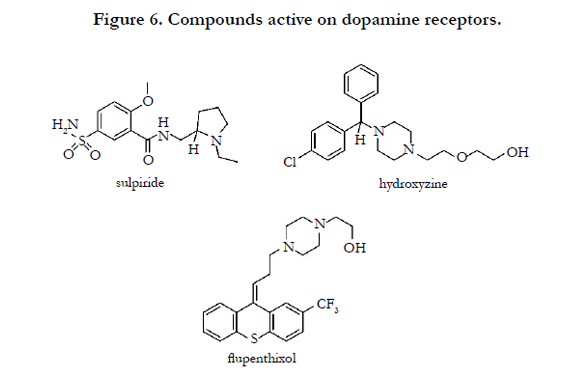
Figure 6. Compounds active on dopamine receptors.
Studies on anticonvulsants [47] (Figure 7) showed that carbamazepine is effective only if tinnitus derives from neurovascular conflict while the other compound, gabapentin, only when the disorder origins from acoustic trauma [48].
The loop inhibiting diuretic, furosemide(Figure 7), given intravenously, reduces the severity of this symptom in 50% of patients. Moreover, studies indicated that it affects tinnitus connected with Ménière’s disease. However, high doses of compound may induce temporary hearing loss and recovery of tinnitus [41].
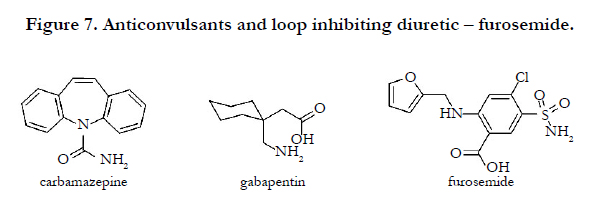
Figure 7. Anticonvulsants and loop inhibiting diuretic – furosemide.
The activity of other substances towards tinnitus was also studied. For example, misoprostol (Figure 8), a synthetic prostaglandin E1 analogue, is effective and safe medicine in therapy of this symptom in hypertensive and/or diabetic patients [49]. Although the first clinical trials of nimodipine (Figure 8), calcium channel blocker, suggested its positive effect on tinnitus patients, the second trials did not confirmed this result [40]. Melatonin (Figure 8), a neurohormone that influences sleep cycle and circadian rhythm, has also a positive effect on the disorder. Although it does not reduce the loudness and frequency of the symptom, it improves the quality of sleep in tinnitus patients [50]. However, it is effective only in combination with sulpiride [40].
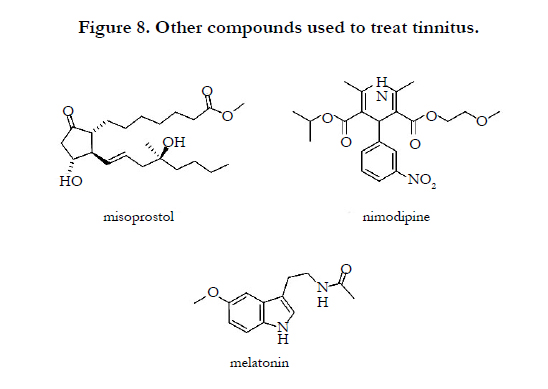
Figure 8. Other compounds used to treat tinnitus.
The other substances, mostly natural ones, were also studied for the treatment for tinnitus. Zinc, for example, has relieving effect but only on patients with hypozincemia [51]. Gingko biloba extract is frequently prescribed for tinnitus patients [52] and the standardized EGb 761® extract is under clinical trials. Some other herbs such as Cimicifugaracemosa, Cornusofficinalis, Verbascumdensiflorum and herbal mixture called Yoku-kan-san have similar effect to Gingko biloba [53]. Even botulinum toxin type A decreases the severity of tinnitus [54] as it reduces inputs from cervical, frontal, temporal and periauricular muscles.
There are also non-pharmacological treatments available: cognitive behavioral therapy, sound therapy, Tinnitus Retraining Therapy, hearing aids, the massage and stretching, and other, more invasive techniques.
Cognitive behavioral therapy consists of two components: the cognitive restructuring, based on identifying and modifying negative thoughts concerning tinnitus, and the behavioral modification promoting habituation to tinnitus by positive imagery, attention control and relaxation [55]. The method is efficient especially in cases when tinnitus leads to severe stress, anxiety or depression [56].
The sound therapy is based on using normal natural sounds from the environment such as streams, rain wind or etc. Such treatment decreases the strength of tinnitus-related activity within the auditory system [57]. Tinnitus Retraining Therapy relies on the neurophysiological model of tinnitus. The first step, retraining teaching/counseling, aims at reclassification of tinnitus sound to the neutral sound (not provoking negative emotions). The second step is the sound therapy [58].
The use of hearing aids is effective only if tinnitus is accompanied by hearing loss [59]. As tinnitus sometimes derives from jaw and neck disorders or temporomandibular joint dysfunction, the massage and stretching of these parts of the body can bring relief [21].
The efficacy of other techniques such as repetitive transcranial magnetic stimulation [60] and electrical stimulation [61] of auditory cortex still requires further investigation. Surgical techniques, still controversial, such as microvascular decompression of cochleovestibular nerve are rarely performed [62].
Conclusion
Tinnitus is the complex disorder and although all pathophysiological mechanisms of its generation are related to dysfunction of auditory nerve and/or dysfunction in transmission of acoustic signal, it is hard to determine which of them may be the most plausible. It might be also possible that all of them are connected with each other or one might trigger the another. Therefore, proposing therapy should be based on detailed examination and individual approach. It seems that combining pharmacological treatment with non-pharmacological one may be the most successful. However, as the mechanism of tinnitus is still not fully understood, more investigation should be performed to explain it.
References
- Dietrich S (2004) Earliest historic reference of 'tinnitus' is controversial. J Laryngol Otol 118(7): 487-488.
- Dan B (2005) Titus's tinnitus. J Hist Neurosci 14(3): 210-213.
- Stephens SD (1984) The treatment of tinnitus-a historical perspective. J Laryngol Otol 98(10): 963-972.
- Jastreboff PJ (1990) Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res 8(4): 221-254.
- Jastreboff PJ, Hazell JW (2004) Tinnitus Retraining Therapy, Implementing the Neurophysiological Model. Cambridge University Press.
- Han BI, Lee HW, Kim TY, Lim JS, Shin KS (2009) Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neurol 5(1): 11-19.
- Langguth B, Kleinjung T, Fischer B, Hajak G, Eichhammer P, et al. (2007) Tinnitus severity, depression, and the big five personality traits. Prog Brain Res 166: 221-225.
- Hébert S, Fullum S, Carrier J (2011) Polysomnographic and quantitative electroencephalographic correlates of subjective sleep complaints in chronic tinnitus. J Sleep Res 20(1 Pt 1): 38-44.
- Møller AR (2011) Texbook of Tinnitus. Epidemiology of Tinnitus in Adults. Springer-Verlag, New York. 29-37.
- Pilgramm M, Rychlick R, Lebisch H, Siedentop H, Goebel G, Kirchhoff D (1999) Tinnitus in the Federal Republic of Germany: a representative epidemiological study. Proceedings of the Sixth International Tinnitus Seminar, London. 64-72.
- Bouccara D (2007) d’ENT World 4: 15.
- Fabijańska A, Rogowski M, Bartnik G, Skarżyński H (1999) Epidemiology of tinnitus and hyperacusis in Poland. Proceedings of the Sixth International Tinnitus Seminar, The Tinnitus and Hyperacusis Centre: London. 569-571.
- Sanchez L, Boyd C, Davis A (1999) Proceedings of the Sixth International innitus Seminar. ed. Hazell J 58–63, The Tinnitus and Hyperacusis Centre: London.
- Coelho CB (2011) Texbook of Tinnitus. Epidemiology of Tinnitus in Children. Springer-Verlag, New York. 39-45.
- Syka J (2002) Plastic Changes in the Central Auditory System After Hearing Loss, Restoration of Function, and During Learning. Physiol Rev 82(3): 601-636.
- Møller AR (2011) Texbook of Tinnitus. Cochlear and Non-cochlear Age- Related Hearing Loss and Tinnitus. Springer, New York. 293-300.
- Baracca G, Del Bo L, Ambrosetti U (2011) Texbook of Tinnitus. Tinnitus and Hearing Loss. Springer, New York. 285-291.
- Gimsing S (2010) Vestibular schwannoma: when to look for it? J Laryngol Otol 124(3): 258-264.
- De Ridder D, Møller AR (2011) Texbook of Tinnitus ed. Møller AR, Langguth B, De Ridder D, Kleinjung T, Microvascular Compression of the Vestibulocochlear Nerve. Springer, New York. 327-335.
- Láinez MJA, Ponz A, Piera A (2011) Texbook of Tinnitus ed. Møller AR, Langguth B, De Ridder D, Kleinjung T, Causes of Tinnitus: Cerebrovascular Diseases. Springer, New York. 337-342.
- Bjorne A (2007) Assessment of temporomandibular and cervical spine disorders in tinnitus patients. Prog Brain Res 166: 215-219.
- Holmes S, Padgham ND (2011) ''Ringing in the ears'': narrative review of tinnitus and its impact. Biol Res Nurs 13(1): 97-108.
- Kaltenbach JA, Godfrey DA (2008) Dorsal cochlear nucleus hyperactivity and tinnitus: are they related? Am J Audiol 17(2): S148-161.
- Mühlnickel W, Elbert T, Taub E, Flor H (1998) Reorganization of auditory cortex in tinnitus. Proc Nat Acad Sci USA 95(17): 10340-10343.
- Eggermont JJ, Roberts LE (2004) The neuroscience of tinnitus. Trends Neurosci 27(11): 676-682.
- Sziklai I (2004) The significance of the calcium signal in the outer hair cells and its possible role in tinnitus of cochlear origin. Eur Arch Otorhinolaryngol 261(10): 517-525.
- Puel JL (1995) Chemical synaptic transmission in the cochlea. Prog Neurobiol 47(6): 449-476.
- Ruel J, Bobbin RP, Vidal D, Pujol R, Puel JL (2000) The selective AMPA receptor antagonist GYKI 53784 blocks action potential generation and excitotoxicity in the guinea pig cochlea. Neuropharmacology 39(11): 1959- 1973.
- Ruel J, Chabbert C, Nouvian R, Bendris R, Eybalin M, et al. (2008) Salicylate enables cochlear arachidonic-acid-sensitive NMDA receptor responses. J Neurosci 28(29): 7313-7323.
- Guitton MJ, Caston J, Ruel J, Johnson RM, Pujol R, et al. (2003) Salicylate induces tinnitus through activation of cochlear NMDA receptors. J Neurosci 23(9): 3944-3952.
- Voytenko SV, Galazyuk AV (2011) mGluRs modulate neuronal firing in the auditory midbrain. Neurosci Lett 492(3): 145-149.
- Brozoski TJ, Caspary DM, Bauer CA, Richardson BD (2010) The effect of supplemental dietary taurine on tinnitus and auditory discrimination in an animal model. Hear Res 270(1-2): 71-80.
- Mellott JG, Motts SD, Schofield BR (2011) Multiple origins of cholinergic innervation of the cochlear nucleus. Neuroscience 180: 138-147.
- Simpson JJ, Davies WE (2000) A review of evidence in support of a role for 5-HT in the perception of tinnitus. Hear Res 145(1-2): 1-7.
- Fornaro M, Martino M (2010) Tinnitus psychopharmacology: A comprehensive review of its pathomechanisms and management. Neuropsychiatr Dis Treat 6: 209-218.
- Langguth B, Elgoyhen AB (2012) Current pharmacological treatments for tinnitus. Expert Opin Pharmacother 13(17): 2495-2509.
- www.ata.org/research-toward-cure .
- Trellakis S, Lautermann J, Lehnerdt G (2007) Lidocaine: neurobiological targets and effects on the auditory system. Prog Brain Res 166: 303-322.
- Robinson S (2007) Antidepressants for treatment of tinnitus. Prog Brain Res 166: 263-271.
- Elgoyhen AB, Langguth B (2011) Texbook of Tinnitus. Pharmacological Approaches to Tinnitus Treatment. Springer, New York. 625-637.
- Langguth B, Salvi R, Elgoyhen AB (2009) Emerging pharmacotherapy of tinnitus. Expert Opin Emerg Drugs 14(4): 687-702.
- Guitton MJ, Dudai Y (2007) Blockade of cochlear NMDA receptors prevents long-term tinnitus during a brief consolidation window after acoustic trauma. Neural Plast 2007: 1-11.
- Sharma DK, Kaur S, Singh J, Kaur I (2012) Role of acamprosate in sensorineural tinnitus. Indian J Pharmacol 44(1): 93-96.
- Suckfüll M, Althaus M, Ellers-Lenz B, Gebauer A, Görtelmeyer R, et al. (2011) A randomized, double-blind, placebo-controlled clinical trial to evaluate the efficacy and safety of neramexane in patients with moderate to severe subjective tinnitus. BMC Ear Nose Throat Disord 11: 1-10.
- Wenzel GI, Warnecke A, Stöver T, Lenarz T (2010) Effects of extracochlear gacyclidine perfusion on tinnitus in humans: a case series. Eur Arch Otorhinolaryngol 267(5): 691-699.
- Lobl JT, Schloss VJ (2009) Patent WO2009155421A1, published also as EP2306839A4 or EP 2306839 A1, Neurosystec Corporation, Jun 18.
- Levine RA (2006) Typewriter tinnitus: a carbamazepine-responsive syndrome related to auditory nerve vascular compression. ORL J Otorhinolaryngol Relat Spec 68(1): 43-47.
- Elgoyhen AB, Langguth B (2010) Pharmacological approaches to the treatment of tinnitus. Drug Discov Today 15(7-8): 300-305.
- Akkuzu B, Yilmaz I, Cakmak O, Ozluoglu LN (2004) Efficacy of misoprostol in the treatment of tinnitus in patients with diabetes and/or hypertension. Auris Nasus Larynx 31(3): 226-232.
- PiccirilloJF (2007) Melatonin. Prog Brain Res 166: 331-333.
- Coelho CB, Tyler R, Hansen M (2007) Zinc as a possible treatment for tinnitus. Prog Brain Res 166: 279-285.
- von Boetticher A (2011) Ginkgo biloba extract in the treatment of tinnitus: a systematic review. Neuropsychiatr Dis Treat 7: 441-447.
- Enrico P, Sirca D, Mereu M (2007) Antioxidants, minerals, vitamins, and herbal remedies in tinnitus therapy. Prog Brain Res 166: 323-330.
- Lainez MJ, Piera A (2007) Botulinum toxin for the treatment of somatic tinnitus. Prog Brain Res 166: 335-338.
- Greimel KV, Kröner-Herwig B (2011) Texbook of Tinnitus. Cognitive Behavioral Treatment (CBT). Springer, New York. 557-561.
- Hesser H, Weise C, Westin VZ, Andersson G (2011) A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress. Clin Psychol Rev 31(4): 545-553.
- Jastreboff MM (2007) Sound therapies for tinnitus management. Prog Brain Res 166: 435-440.
- Jastreboff PF, Jastreboff MM (2006) Tinnitus retraining therapy: a different view on tinnitus. ORL J Otorhinolaryngol Relat Spec 68(1): 23-30.
- Del Bo L, Ambrosetti U (2007) Hearing aids for the treatment of tinnitus. Prog Brain Res 166: 341-345.
- Langguth B, Kleinjung T, Landgrebe M, de Ridder D, Hajak G (2010) rTMS for the treatment of tinnitus: the role of neuronavigation for coil positioning. Neurophysiol Clin 40(1): 45-58.
- De Ridder D, De Mulder G, Menovsky T, Sunaert S, Kovacs S (2007) Electrical stimulation of auditory and somatosensory cortices for treatment of tinnitus and pain. Prog Brain Res 166: 377-388.
- Yap L, Pothula VB, Lesser T (2008) Microvascular decompression of cochleovestibular nerve. Eur Arch Otorhinolaryngol 265(8): 861-869.





