Neuroendocrine Tumor Orthopedic Sequela: Literature Review and Case Presentation
Samona J*, Ndubaku O, Fernández D
McLaren Regional Medical Center, Orthopaedic Surgery Department, Ballenger Highway, USA.
*Corresponding Author
Jason Samona DO,
McLaren Regional Medical Center,
Orthopaedic Surgery Department,
401 S. Ballenger Highway, Flint, MI 48532,
USA.
Tel: 248.939.6263
Fax: 810.342.2150
E-mail: Jasonsamona@yahoo.com
Received: January 09, 2016; Accepted: February 09, 2016; Published: February 11, 2016
Citation: Samona J, Ndubaku O, Fernández D (2016) Neuroendocrine Tumor Orthopedic Sequela: Literature Review and Case Presentation. Int J Bone Rheumatol Res. 3(1), 25-27.DOI : dx.doi.org/10.19070/2470-4520-160006
Copyright: Samona J© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
This report presents a very aggressive and unusual case of a rare musculoskeletal neoplastic process, which ultimately resulted in the death of a patient. It is of utmost importance to present this case, in order to display the abnormal nature of this disease process, improve future treatment, and reduce morbidity and mortality. The abnormal pathological variant presented in this case and the lack of literature on the malignancy, highlights the lack of studies into the orthopedic sequela of these tumors. Further research regarding this entity, will decrease the complications, including; pathological fractures, subsequent debility and death.
2.Case Report
3. Discussion
4.Conclusion
5.References
Introduction
Neuroendocrine neurosecretory cells receive neuronal input and release messenger molecules in the form of hormones into the circulatory system. These cells are distributed throughout the human body; within the substance of numerous organs and throughout numerous systems. Neuroendocrine cells and their associated tumors, most commonly occur in the intestinal tract, although they are also found throughout the body [1, 2]. Neuroendocrine tumors (NETs) classification scheme includes; typical carcinoid, atypical carcinoid, small cell carcinoma (neuroendocrine type), combined small cell carcinoma (neuroendocrine type), as well as paraganglioma (both benign and malignant forms) [3, 4].
Metastatic bone disease overall has been proven to be the 3rd most common metastatic site (after lung and liver) [5]. Tumors found to carry the highest rate of developing metastatic bone lesions have proven to be the prostate 32.4%, breast 21.9%, kidney 16.4%, thyroid 11.7%, lung 10.9%, and testes 10.2%. Postmortem studies have revealed the prevalence of bone metastases for cancers of all types, ranging from 7-27%, in contrast to approximately 7% of patients with neuroendocrine tumors [5]. The most common skeletal manifestation of malignancy is focal or generalized osteolysis [6], and commonly associated with bone pain, pathologic fractures, and hypercalcemia. Bone pain being by far the most common symptom [7, 8]. In a study named “Bone Metastases in Carcinoid Tumors”, over 90% of patients with this particular form of NET experienced bone pain in association with bone metastases [8]. Some patients may even display tenderness with pressure when applied to the regions of the bone affected by the metastatic disease [5]. Rarely, NET associated osteolytic lesions may cause swelling or neurological symptoms and signs. Multiple vertebral and skeletal lesions commonly present simultaneously in a given patient [7]. Bone metastases are not usually detected until after the primary tumor has been identified. Only 22.6% of patients with metastatic bone lesions are identified by their neoplastic osseous involvement [5]. In 30% of cases it has been found the origin of the skeletal metastasis remains unidentified.
Metastases to bone in association with neuroendocrine tumors is an indication of advanced disease and worsen prognosis, thus early detection plays a vital role in therapy [9]. In one study, 100% of the subjects with bone metastases displayed advanced disease characterized by widespread metastases. The indolent course of the disease process and its difficult diagnosis leads to widespread metastases before the malignancy is identified [8].
Bone metastases in many NETs predominantly collect within the axial skeleton, at comparable rates to those found in nonendocrine tumors [8]. When further broken down, the sites found to be most frequently involved with metastases from neuroendocrine tumors are the vertebrae, pelvis, ribs, femur and skull [8]. Incidence at the spine varies depending on the region in question. The thoracic spine being affected in greater than 66% of cases, the lumbosacral region in 20% and cervical spine comprising 10% of bone metastatic lesions [5]. Instability created in the spine is the major cause of back pain in 10% of cancer patients. Metastatic destruction of bone leads to trabecular disruption and microfractures, leading to a deceased load bearing capacity of the bone, and subsequently a total loss of bone integrity. Most commonly seen are rib fractures and collapse of the vertebral column. These in turn will result in a degree of restrictive lung disease, loss of height, kyphoscoliosis, and debility. The probability of developing a metastatic fracture is directly related to the duration of metastatic involvement.
This report presents a very aggressive and unusual case of a rare musculoskeletal neoplastic process, which ultimately resulted in the death of a patient. It is of utmost importance to present this case, in order to display the abnormal nature of this disease process, improve future treatment, and reduce morbidity and mortality.
Case Report
A 59 year old African American female originally presented to the emergency department, with the chief complaint of low blood pressure, dizziness, dyspnea and a “knot” on her scalp. The patient had a 40 pound weight loss in the past month. A mass along the right frontal scalp region was noticed approximately 1 week prior to presentation at the Emergency Department. The mass was initially the size of a peanut, however, it has rapidly increased in size since in the week or so time frame from when it was first noticed. A CT of the brain revealed a 5.9 x 5.0 cm soft tissue mass. It was associated with osteolytic defects in the right frontal bone, effacement of the right frontal lobe, abutting of the dura of the brain, and an associated 4 mm midline shift of the right frontal lobe (image 1).
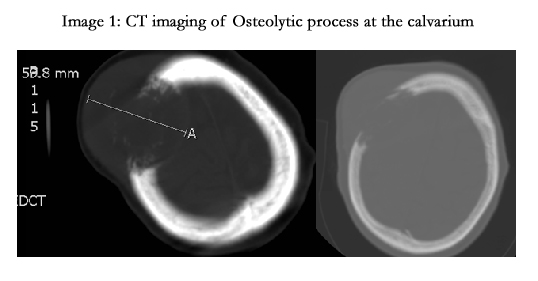
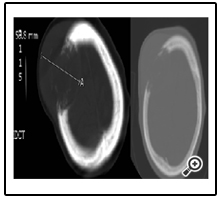
Image 1: CT imaging of Osteolytic process at the calvarium
A CT of the thorax-abdomen-pelvis as well as Scintigraphy with technetium 99m revealed widespread metastatic involvement of the appendicular and axial skeleton (image 2). Imaging displayed disease in the left paraspinal region of the left psoas muscle, L4 vertebral body & transverse process with osteolysis, pathologic rib destruction and fracturing involving the posterior medial aspect of the right ninth rib. Abnormal activity was seen in the left femoral midshaft as well. Significant neoplastic lesions were noted at the pulmonary hilum and mediastinum, posterior to the bladder, anterior to the rectum, and vaginal cuff, with an associated irregular exophytic mass at the periurethral area. Biopsies and patient evaluation revealed a high-grade poorly differentiated invasive neuroendocrine carcinoma with diffuse metastatic disease throughout the body.
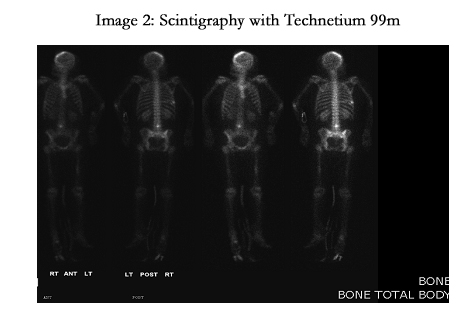
Image 2: Scintigraphy with Technetium 99m
3 weeks from initial presentation to the hospital, the cranial mass had grown to approximately 8.5 cm at its greatest dimension, extending approximately 4 cm away from the patient’s scalp. The large mass invaded through the bone and was causing a soft tissue mass effect of 7 mm intracranial shift, leading to impingement on the right frontal lobe and became unresponsive to sensory stimuli or commands. This state is in stark contrast to less than 3 weeks prior when the patient had presented to the hospital with a “knot” on her scalp, was alert and oriented, talkative and following commands. Upon review of her laboratory studies, the serum calcium was 12.9, denoting hypercalcemia. The patient ultimately died secondary to complications associated with diffuse metastatic lesions.
Discussion
In contrast to the presentation of the patient, only approximately 7% of patients with neuroendocrine tumors have diagnosed metastases to the bone. Not only were there neoplastic processes effecting osseous structures, but the vast majority of the body’s metastatic lesions involved bone. Therefore the patient shattered what is considered normal for most neuroendocrine derived tumors. This is surprising considering the marked metastases diffusely throughout the calvarium, nearly the entire vertebral column, multiple ribs, pelvis, the left femoral midshaft, and the remarkable rapidly enlarging grapefruit-like sized osteolytic lesion protruding from the patient’s skull.
Osteolytic bone metastases from NETs often present with “stereotypical symptoms”. These include pathologic fractures, hypercalcemia, but bone pain is by far the most common symptom [7, 8]. Over 90% of the patients with NET derived bone metastases experience bone pain, although it was not seen in this patient. The traditionally less common neurological signs and symptoms were the major presenting feature in the patient, despite the wide spread destructive osteolytic processes.
Only 22.6% of patients with bone metastases are initially identified by the actual osseous involvement of their cancer. Although, in this patient the signs and symptoms of bone metastases were the first features of the underlying neoplastic process. Osteolysis of the calvarium and the brain tumor were first to be detected, and the widespread boney metastases was subsequently discovered via further diagnostic imaging. Unique to this patient’s case is that bone metastases was detected without proper identification of the primary tumor. The primary tumor was never detected in this patient. The origin of skeletal metastases remains unknown in only 30% of cases. This is yet another indication this tumor differs from that of what is considered “common” for most NETs, and all tumors in general.
Conclusion
Neuroendocrine derived tumors may involve skeletal lesions related to bone metastases more commonly than what is currently accepted in the literature. This study also reminds the scientific community that although rare, neoplasms may reveal themselves by the sequela of the boney involvement, rather than the signs and symptoms created by the primary tumor. When present, boney lesions may represent a rapidly expanding life threatening scenario in which immediate action is necessary in order to prevent mortality. Even in the scenario of wide spread osseous destruction, the patient may lack the presentation seen in over 90% of such patients, pain.
“Syndromes” or particular “pathologies” are characterized by a similar constellation of signs, symptoms, and epidemiological factors. The stark differences in the presentation of this patient in comparison to the more common presentation of NETs, gives credence to the possibility of the discovery of a new highly invasive cancerous process. The various subtypes of this form of cancer are sporadically discovered and the recognition is the first step in devising appropriate treatments to save life and limb.
Through a review of the literature of the osseous effects of neuroendocrine tumors, it is evident there is a lack of studies into the subtypes. The currently accepted clinical presentations and definitions are largely based off the qualities of the carcinoid and oat cell forms of NETs. These are the most common forms, thus the majority of the literature involves these variants. The authors of this paper call for further studies into other variants and a more specific classification scheme. This may allow clinicians to better identify, develop treatment regimens and ultimately cure patients of NETs. This would decrease the osseous and therefore orthopedic implications of neuroendocrine tumors, which include pathological fractures, subsequent debility and possible death.
References
- Neuroendocrine tumors are complex malignancies (2011) Novartis Pharmaceuticals Corporation.
- Neuroendocrine Tumors (2008) Dana-Farber Cancer Institute, Harvard Medical School.
- World Health Organization Classification of Tumours (2005) Pathology and Genetics of Head and Neck Tumors. IARC Press, Lyon, France. 9: 1-435.
- Fitzgibbon DR, Loeser JD (2010) Cancer Pain: Assessment, Diagnosis, and Management. Lippincott Williams & Wilkins, New York.
- Tubiana-Hulin M (1991) Incidence, prevalence and distribution of bone metastases. Bone 12(Suppl 1): S9-10.
- Putzer D, Gabriel M, Henninger B, Kendler D, Uprimny C, et al. (2009) Bone metastases in patients with neuroendocrine tumor: 68Ga-DOTATyr3-octreotide PET in comparison to CT and bone scintigraphy. J Nucl Med 50(8): 1214-1221.
- Holmen J, Stevens MA, El-Khoury GY (1999) Case report: paraarticular soft-tissue osteoma of the hip. Iowa Orthop J 19: 139-141.
- Meijer WG, van der Veer E, Jager PL, van der Jagt EJ, Piers BA, et al. (2003) Bone metastases in carcinoid tumors: clinical features, imaging characteristics,and markers of bone metabolism. J Nucl Med 44(2): 184-191.
- Lebtahi R, Cadiot G, Delahaye N, Genin R, Daou D, et al. (1999) Detection of bone metastases in patients with endocrine gastroenteropancreatic tumors: bone scintigraphy compared with somatostatin receptor scintigraphy. J Nucl Med 40(10): 1602-1608.





