Occupational Contact Dermatitis in the Food Industry
Lahya Afshari Saleh1, Nasrin anvari2, Bita Kiafar3, Farzaneh Rahimpour4*
1 Assistant professor, Department of Occupational Medicine, Division of Sleep Medicine, Psychiatry and Behavioral Sciences Research Center,Mashhad
University of Medical Sciences, Mashhad, Iran.
2 Occupational Medicine specialist, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
3 Associate professor, Cutaneous leishmaniasis research center, Mashhad University of Medical Sciences, Mashhad, Iran.
4 Assistant professor, Department of Occupational Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author
Farzaneh Rahimpour,
Assistant professor, Department of Occupational Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
E-mail: rahimpourf@mums.ac.ir
Received: September 18, 2021; Accepted: November 13, 2021; Published: November 23, 2021
Citation: Lahya Afshari Saleh, Nasrin Anvari, Bita Kiafar, Farzaneh Rahimpour. Occupational Contact Dermatitis in the Food Industry. Int J Dentistry Oral Sci. 2021;8(11):5117-5121. doi: dx.doi.org/10.19070/2572-7613-2100024
Copyright: Farzaneh Rahimpour�2021. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Contact dermatitis accounts for 90% of all occupational skin diseases which is considered a costly occupational
disease. The aim of the present study was to investigate contact dermatitis and relevant occupational factors among food
industry workers.
Study Design: The present cross-sectional study was carried out among food supply, production, distribution and preservation
centers of Mashhad, Iran from 2017 to 2018.
Methods: Workers in food industry who were referred to periodic training centers for employees entered the study with at
least one year of work experience. The two-part questionnaire including demographic and occupational information and the
occupational skin questionnaire (Nordic Occupational Skin Questionnaire (NOSQ-2002/SHORT), which is validated in Persian,
was filled by the participants. Individuals with dermatitis were examined and the results were recorded.
Results: A total of 384 food industry workers entered the study including 316 (82.3%) men and 68 (17.7%) women. 32 (8.4%)
subjects were suffering from eczema, among which 25 (78.1%) had hand eczema, 6 (18.8%) had both wrist and hand eczema
and 1 (3.1%) had eczema confined to the wrist. The statistical analysis revealed that gender and previous familial and personal
history of atopy were significantly correlated with hand and wrist eczema (P-value =0.05 was significant).
Conclusion: Prevalence of dermatitis varies in food industry workers regarding the job status. In this study, occupational
dermatitis proved to be more prevalent among men and individuals with a personal or family history of atopy, thus these people
should be under strict supervision of health practitioners working in the food industry. Further studies are recommended
among the employees of certain subunits of the food industry.
2.Introduction
3.Materials and Methods
3.Results
4.Discussion
5.Conclusion
5.References
Keywords
Occupational Dermatitis; Contact Dermatitis; Nordic Occupational Skin Questionnaire; Food Industry Workers.
Introduction
Occupational dermatosis (OD) or occupational skin disease
(OSD) is described as any pathological condition of the skin,
which is caused or worsened by an occupational exposure [1].
Skin diseases account for more than 30% of all occupational diseases,
affecting approximately 1 per 1000 workers annually and
are responsible for decreased productivity and lost workdays in
different industries [1]. Environmental chemicals are among the
main causes of OSDs and there are about 2000 substances known
as contact allergens [1]. Approximately 90% of all OSDs are reported
as contact dermatitis [9, 10]. The food and catering industries
account for more than 10% of all occupational dermatitis,
which is considered as a major occupational health threat. The
most important workers at risk include chefs, cooks, kitchen and
catering assistants and counter hands. Waiters, cleaners, bakers,
confectioners, greengrocers and meat, poultry and fish handlers
are among other workers at risk in this area [5]. In most of the
food and catering jobs, prolonged contact with water, soap and
disinfectants required for hygiene issues causes more than 55%
of dermatitis cases. More than 40% of occupational dermatitis in
industry is due to contact with foods, including sugar, flour, fruits,
vegetables, seasonings, seafood, meat and poultry [5]. Occupational
dermatitis may be seen mainly as irritant contact dermatitis and allergic contact dermatitis [6]. Various host factors may
have a role in developing occupational dermatitis, such as history
of atopy, pigmented skins, old and wrinkled skins and immune
deficient workers. White people, compared with blacks are more
prone to dermatitis [7, 8]. The primary aim of this research was to
investigate contact dermatitis and its related occupational factors
among food handlers and sellers.
Materials And Methods
This cross-sectional study was carried out under supervision of
Mashhad University of Medical Sciences form 2017 to 2018. Regular
training courses are conducted in Iran for food preparers,
distributers and sellers including greengrocers, butchers, bakers,
confectioners and restaurant, catering and fast-food staff. Subjects
referred to these training centers were studied using random
sampling method within one year period. Those who had foodrelated
occupations for at least one year in the city of Mashhad
were included in this study and exclusion criteria were as follows:
dissatisfaction for entering the study, immunocompromised cases,
using immunosuppressive drugs and previous history of a skin
disease before employment. A two-part questionnaire, including
a demographic checklist designed by the author and the validated
Nordic Occupational Skin Questionnaire (NOSQ-2002/SHORT)
was used. Cases with dermatitis were examined by occupational
medicine specialists and referred to our dermatologist colleague
for a precise diagnosis. Data were collected and entered into the
SPSS V.20 Software. The relationship between the frequency of
dermatitis and job-related factors were evaluated with the T-test,
chi-squared test and Fisher�s exact test. The level of significance
was 0.05 for all tests.
Findings
Demographic indices
A total of 384 food handlers in the city of Mashhad were studied.
316 (82.3%) cases were male and 68 (17.7%) cases were female.
Among the participants, 288 (75%) cases were married and 96
(25%) were single. According to education levels, 6 were illiterate
(1.6%), 340 had a high school diploma or less (88.5%) and 38 had
higher education (9.9%). Among the participants of this study 32
(8.3%) cases had a pet. 32 (8.4%) subjects were suffering from
eczema, 25 (78.1%) of those had hand eczema, 6 (18.8%) had
both wrist and hand eczema and 1 (3.1%) had eczema confined
to the wrist. Subjects with hand and/or wrist eczema were asked
regarding probable factors of dermatitis in or out of the work
place. Among them 4 (12.5%) cases believed that the probable
factor was outside the workplace while 17 (58.6%) cases blamed
workplace for developing the disease. The number of subjects
suffered from itchy, dry and scaly skin were 2 (0.5%), 54 (14.1%)
and 2 (0.5%), respectively. 18 (4.7%) cases reported more than
one skin symptom and 308 (80.2%) cases showed no skin symptoms.
42 (10.9%) cases stated that seasonal changes altered the
skin symptoms and 342 (89.1%) believed that seasonal changes
had no effect on their skin. Table 1 shows the frequency of hand
eczema according to the time of occurrence.
The relationship between the quantitative and qualitative demographic
and occupational variables was appropriate according to
the statistical tests. Table 2 illustrates the qualitative demographic
and occupational variables in two groups of patients with hand
eczema and healthy individuals.
Table 3 shows the frequency of occupations in both study groups.
Chi-squared test was used to compare the frequency of jobs in
both study groups, through which no significant difference
was detected between the two groups, in terms of current jobs
(P=0.49).
Moreover, table 4 depicts the quantitative demographic and job
variables in two groups of patients with hand eczema and healthy
individuals. The relationship between annual eczema recurrence
while working and occupation types was studied based on an appropriate
statistical test and no significant relationship was found
(P=0.67) (Table 5).
The relationship between eczema improvement during weekends
within a year and occupation types was studies and no significant
relationship was detected (P=0.86) (Table 6).
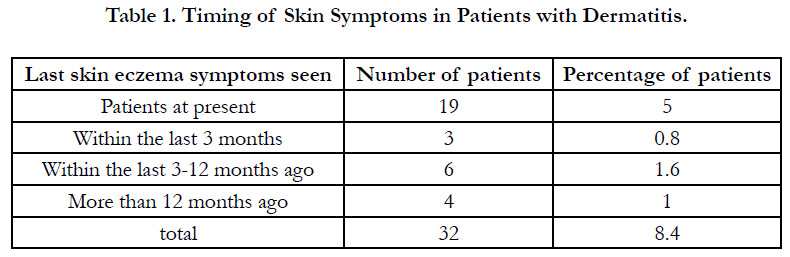

Table 1. Timing of Skin Symptoms in Patients with Dermatitis.
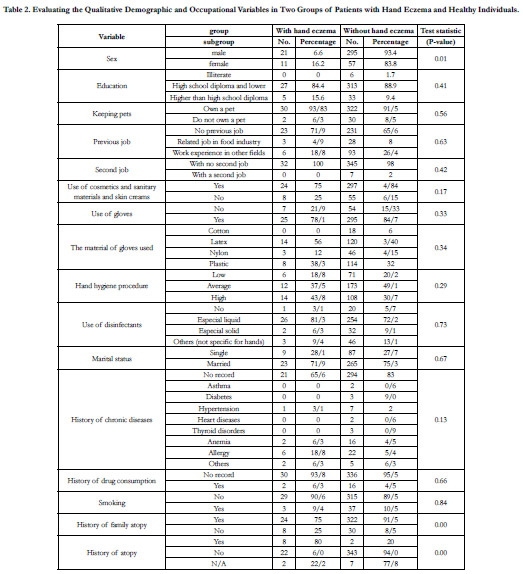
Table 2. Evaluating the Qualitative Demographic and Occupational Variables in Two Groups of Patients with Hand Eczema and Healthy Individuals.
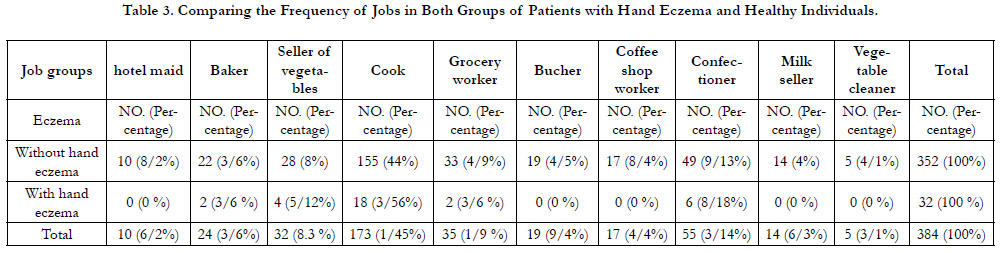
Table 3. Comparing the Frequency of Jobs in Both Groups of Patients with Hand Eczema and Healthy Individuals.
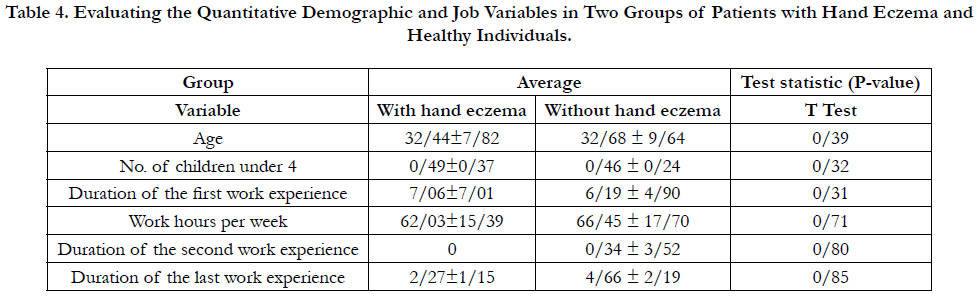
Table 4. Evaluating the Quantitative Demographic and Job Variables in Two Groups of Patients with Hand Eczema and Healthy Individuals.
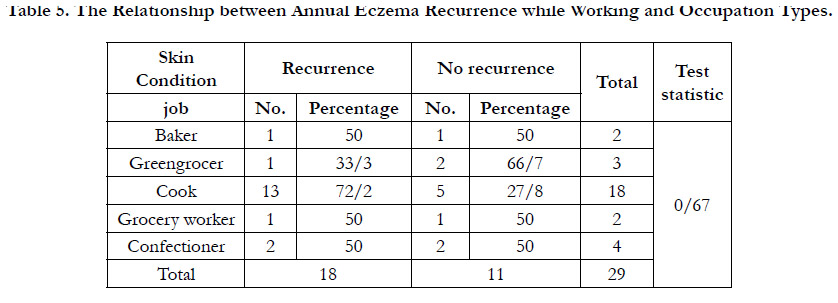
Table 5. The Relationship between Annual Eczema Recurrence while Working and Occupation Types.
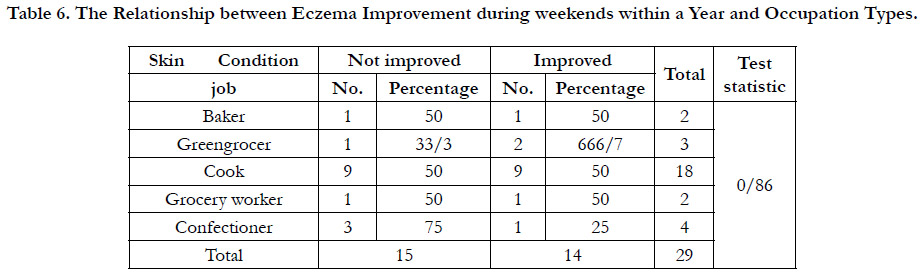
Table 6. The Relationship between Eczema Improvement during weekends within a Year and Occupation Types.
Discussion and Conclusion
Of the 345 employees working as food preparers, distributers and
sellers 32 (8.4%) subjects had eczema. The annual prevalence of
dermatitis was 7.5% in this study. Recent studies on occupational
health indicate that food-related occupations are among the major
factors contributing to contact dermatitis [2, 5]. Smith et al.
reported the annual prevalence of skin disorders in food industry
among kitchen workers was 1414 people per million. The study
was performed on 193,132 personnel using a questionnaire. Skin
disorders were higher among cases who had wet-work exposure
[21]. In another study on 1052 food industry workers in Finland
in 1985, Peltonen et al. showed that 17% of their study population
were suffering from skin diseases. The frequency of occupational
eczema was 8.5% which was twice higher among fish, meat
and vegetable handlers and also confectioners. Hand eczema existed
in 15% of the food handlers and 6% of the office employees
[19]. Other studies reported a higher prevalence. According to a
study by Sylvia Teo et al. (2003), the prevalence of occupational
dermatitis among 457 restaurant, catering and fast-food staff in
Singapore was 10% within a year [22]. The incidence of occupational dermatitis was reported 34% among 90 food services
workers in Poland [18] and in another research the annual incidence
rates of occupational dermatoses in Germany were 33.2%
and 23.9% among bakers and pastry cooks, respectively [23]. In
a similar study conducted in Iran by Fathi et al., the incidence of
occupational dermatitis among the food industry staff was 9.5%
in a 5-year period in the city of Yazd [15]. In the present study, the
one-year prevalence of dermatitis among food industry workers
was 7.3%. The following factors may account for the significant
difference in the rate of occupational dermatitis between Iranians
and other populations:
1- Genetic: Genetic effects, particularly atopic backgrounds, vary
in different populations (7 and 8).
2- Risk factors for contact dermatitis: Food consumption patterns
of Iran is different from other countries. For example, mustard
which is a popular ingredient of salad dressings and induces contact
dermatitis, is less commonly used in our country (7 and 8).
Furthermore, seafood types, meat types and spices are different
from each other in East Asia, Europe and Iran. In addition, cooking
traditions in some countries are different from our country.
3- Hand washing: Based on the guideline for the workplace and
environmental health center, the workers of food supply, distribution
and preservation units should frequently wash their hands
with a particular method. Considering the significant role of soap
and water in developing contact dermatitis, dermatitis types in different countries may be due to the number of hand-washing
episodes per day. In this study, 77 participants (20%) reported a
low frequency of daily hand-washing. In addition, despite ensuring
confidentiality, honesty of workers in completing questionnaires
is still doubtful.
4- Unbalanced job distribution of the subjects: In the current
study, different jobs related to raw foods, food preparation and
preservation and food products were assessed. Similar studies
were mostly concentrated on fast-food employees, bakers and
confectioners. Hence, a reason for the presence of various prevalence
rates may be the diversified variable in the subcategories of
industry.
5- No defined job duty: Another distribution difference may be
the duty of individuals in some units, so that there are no factors
related to dermatitis. For example the exposure factors would
change for a cook assistant working the whole day or all days of
the week.
6- Climate conditions: The amount of moisture alters the frequency
of dermatitis [2].
Current study demonstrated that a personal or family history of
atopy and also gender differences affected the prevalence of the
contact dermatitis, highlights the role of genetics in the outbreak
of dermatitis in the study population. Similar studies showed a
significant relationship between the hand washing frequency, job
safety and etc., and the prevalence of contact dermatitis [22]. In
this study, the aforementioned factors were different between
dermatitis patients and healthy subjects. Nevertheless, no statistically
significant difference was detected. The reasons to explain
this issue may be explained as follows:
1- The presence of recall bias in symptom improvement during
the holiday period. Considering the fact that symptom improvement
requires at least one week off, the employees had probably
no such long holidays since Mashhad is a touristic city.
2. The presence of reporting bias in hand washing frequency and
using personal protective equipment, which is less frequent considering
the random sampling.
3. Short-term employment record, economic status of the country
and new employments may be among other influencing factors.
The number of children under 4 years was considered as a contributing
factor to dermatitis but no statistically significant result
was achieved in our study. This outcome could be explained as
the lower percentage of females (17.7%), who are more responsible
for child care in our country (24). In this article, the average
employment period in dermatitis group was more than the
healthy group, however, the difference was not statistically significant.
This may be due to a relatively low average of working
years in the study population (7 years on average) according
to the employment of young persons and frequent job change
in industry. The findings of this study indicate that the annual
prevalence of dermatitis is higher among men, which is probably
because of the job type (women mostly work as packaging staff
and men work as food preparers and have direct contact with raw
materials). The incidence of chronic diseases was low in the study
population (probably due to a lower average age) which made the
application of statistical tests difficult. The level of education had
no relationship with the prevalence of dermatitis, because of the
proximity of the educational levels in the study groups. Moreover,
the reporting bias (inaccurate reporting of educational level) was
inevitable.
Advantages
The translation and assessment of reliability and validity of Nordic
skin Questionnaire was a major advantage of this study. The
study sample is relatively larger than similar studies.
Disadvantages
It was not possible to assure the job relatedness of a skin disease
due to the unavailability of a certain paraclinical test for food materials
and high costs of testing procedures.
Suggestions
1- Developing electronic records related to the information of
personnel is one of the main infrastructure actions. Considering
the reasonable initial costs of launching this system as well as training people, the industrial system and related occupational diseases
could be assessed more accurately. Finally, this could lessen
the financial burden of insurance and corporations and also reduces
the inconvenience of employees in the upcoming years.
2- Detecting patients with atopy during periodical job examinations
helps to regularly track any probable skin disorder in future.
References
-
[1]. Williams N. AMA guides to the evaluation of work ability and return to
work.
[2]. Rosenstock L, Cullen M, Brodkin C, Redlich C. Textbook of clinical occupational and environmental medicine.
[3]. LaDou J, Harrison R. Current occupational & environmental medicine. 2014.
[4]. Rom WN, Markowitz S. Environmental and Occupational Medicine. Philadelphia: Wolters Kluwer Health. 2011.
[5]. Occupational dermatitis in the catering and food industries.[http://www. hse.gov.uk/food/dermatitis.htm] [Nov 29, 2012] .
[6]. DermNet New Zealand: All about the skin. [http://www.dermnetnz.org/ topics/occupational-skin-diease] [2012].
[7]. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI food allergy and anaphylaxis guidelines: diagnosis and management of food allergy. Allergy. 2014 Aug;69(8):1008-25.
[8]. Wang J, Sampson HA. Food allergy. J. Clin. Investig. 2011 Mar 1;121(3):827-35.v [9]. Diepgen TL, Coenraads PJ. The epidemiology of occupational contact dermatitis. Int Arch Occup Environ Health. 1999 Nov;72(8):496-506.
[10]. Droste J, Vermeire P, Van Sprundel M, Bulat P, Braeckman L, Myny K, et al. Occupational exposure among bakery workers: impact on the occurrence of work-related symptoms as compared with allergic characteristics. J Occup Environ Med. 2005 May;47(5):458-65.Pubmed PMID: 15891524.
[11]. Diepgen TL, Scheidt R, Weisshaar E, John SM, Hieke K. Cost of illness from occupational hand eczema in Germany. Contact Derm. 2013 Aug;69(2):99-106.
[12]. Goldsmith L, Katz S, Gilchrest BA, Paller AS, Leffell DJ, Wolff K. Fitzpatrick�s Dermatology in General Medicine, Ed. McGrawHill Medical. 2012:2421-9.
[13]. Griffiths C, Barker J, Bleiker TO, Chalmers R, Creamer D, editors. Rook's textbook of dermatology. John Wiley & Sons; 2016 Feb 29.
[14]. Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014 Dec 1;5(4):175-80.
[15]. Fathi F, Jafarpoor M. Matching evaluation between occupational contact dermatitis and various jobs in Yazd in during 2007-2012. Acta Med Iran. 2013;51(11):793-8.Pubmed PMID: 24390950.
[16]. Steiner MF, Dick FD, Scaife AR, Semple S, Paudyal P, Ayres JG. High prevalence of skin symptoms among bakery workers. Occup Med. 2011 Jun 1;61(4):280-2.
[17]. Bauer A, Geier J, Elsner P. Type IV allergy in the food processing industry: sensitization profiles in bakers, cooks and butchers. Contact Derm. 2002 Apr;46(4):228-35.Pubmed PMID: 12081702.
[18]. Kurpiewska J, Liwkowicz J, Benczek K, Padlewska K. A survey of workrelated skin diseases in different occupations in Poland. Int J Occup Saf Ergon. 2011 Jan 1;17(2):207-14.
[19]. Peltonen L, Wickstr�m G, Vaahtoranta M. Occupational dermatoses in the food industry. Dermatosen in Beruf und Umwelt Occupation and environment. 1984;33(5):166-9.
[20]. Bauer A, Kelterer D, Stadeler M, Schneider W, Kleesz P, Wollina U, et al. The prevention of occupational hand dermatitis in bakers, confectioners and employees in the catering trades. Preliminary results of a skin prevention program. Contact Dermatitis. 2001 Feb;44(2):85-8.Pubmed PMID: 11205409.
[21]. Smith TA. Occupational skin conditions in the food industry. Occup. Med. 2000 Nov 1;50(8):597-8.
[22]. Teo S, Teik-Jin Goon A, Siang LH, Lin GS, Koh D. Occupational dermatoses in restaurant, catering and fast-food outlets in Singapore. Occup Med (Lond). 2009 Oct;59(7):466-71.Pubmed PMID: 19297338.
[23]. Mahler V. Occupational Contact Dermatitis: Chefs and Food Handlers. In: Johansen JD, Frosch PJ, Lepoittevin J-P, editors. Contact Dermatitis. Berlin, Heidelberg: Springer Berlin Heidelberg; 2011. p. 853-64.
[24]. Abbasi-Shavazi MJ, Inhorn MC, Razeghi-Nasrabad HB, Toloo G. The �Iranian ART Revolution� infertility, assisted reproductive technology, and third-party donation in the Islamic Republic of Iran. J. Middle East Women's Stud. 2008;4(2):1-28.





