Angioleiomyoma of Nasal Septum: Case Report and Literature Review
Varun V. Varadarajan*, Justice JM
Department of Otolaryngology, University of Florida, Gainesville, FL, USA.
*Corresponding Author
Varun V. Varadarajan MD,
Department of Otolaryngology, University of Florida,
Gainesville, FL, USA.
Tel: 352-273-5199
Fax: 352-392-6781
E-mail: varun.varadarajan@ent.ufl.edu
Received: July 27, 2016; Accepted: August 19, 2016; Published: August 22, 2016
Citation: Varun V. Varadarajan, Justice JM (2016) Angioleiomyoma of Nasal Septum: Case Report and Literature Review. Int J Clin Exp Otolaryngol. 2(3), 31-34. doi: dx.doi.org/10.19070/2572-732X-160006
Copyright: Varun V. Varadarajan© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Angioleiomyoma is a benign soft tissue tumor of smooth muscle origin with a vascular component and is an uncommon form of leiomyoma. Angioleiomyoma presenting in the nasal cavity is exceedingly rare and there are 68 reported cases in the literature worldwide. We present a case of angioleiomyoma of the nasal septum and review its diagnosis and treatment.
Study Design: Case report and Literature Review.
Methods: The medical records of a 69-year-old patient with an angioleiomyoma of the nasal septum were reviewed. The
PubMed database was searched for literature describing anglioleiomyoma of the nasal cavity using the key words “angioleiomyoma”
with “nasal cavity,” “nasal septum,” “nose,” or “sinus.”
Results: A 69-year-old female patient presented with progressive right-sided nasal obstruction and epistaxis. Office examination
revealed stigmata of recent bleeding and nasal endoscopy revealed a mass arising from the right nasal septum.
Computerized tomography with intravenous contrast revealed a 1.3 x 1.1 cm heterogeneously enhancing vascular lesion
arising from the right nasal septum. The patient was taken to the operating room for endoscopic resection.
Conclusion: Angioleiomyoma of the nasal septum is a rare and challenging clinical diagnosis that requires detailed histopathologic
examination. Literature review suggests a female predilection with possible hormonal influence.
2.Introduction
3.Case Presentation
4.Discussion
5.Conclusions
6.References
Keywords
Rhinology; Angioleiomyoma; Nose Neoplasms.
Introduction
Angioleiomyoma is a benign soft tissue tumor of smooth muscle origin with a vascular component and is a rare form of leiomyoma. Like other sinonasal mesenchymal tumors, angioleiomyomas are uncommon in the nasal cavity and there are 68 reported cases in the literature worldwide [1-22]. Angioleiomyoma presenting on the nasal cavity is exceedingly rare and the first reported case if sinonasal angioleiomyoma was by Maesaka in 1966 [2]. Literature review reveals 16 reported cases on the nasal septum [1, 4-8, 19, 20, 22-25]. We present a new case of angioleiomyoma of the nasal septum, review its diagnosis, clinical and pathologic characteristics, and management.
Case Presentation
A 69-year-old African American female was referred to our Otolaryngology clinic with the chief complaints of progressive right-sided nasal obstruction and epistaxis for one year in duration. She had a history of allergic rhinitis and also endorsed sneezing and clear rhinorrhea. The patient is post-menopausal and has a past medical history of hypertension, hyperlipidemia, chronic gastritis, multiple renal cysts, renal artery aneurysm, and hyperaldosteronism. She denied tobacco use. She has no history of head or nasal trauma, sinonasal surgery, or history of cancer.
Upon physical examination, anterior rhinoscopy revealed crusting and stigmata of recent bleeding and nasal endoscopy revealed a smooth, pink, vascular appearing mass arising from the right nasal septum was visualized. The mass was touching the right lateral wall and completely filled the superior aspect of the right nasal vestibule (See Figure 1). A computerized tomography scan with intravenous contrast revealed a 1.3 x 1.1 cm heterogeneously enhancing vascular lesion within the right anterior nasal cavity that appeared to arise from the nasal septum (Figure 2). Given
the benign appearance of the lesion, further imaging was not obtained.
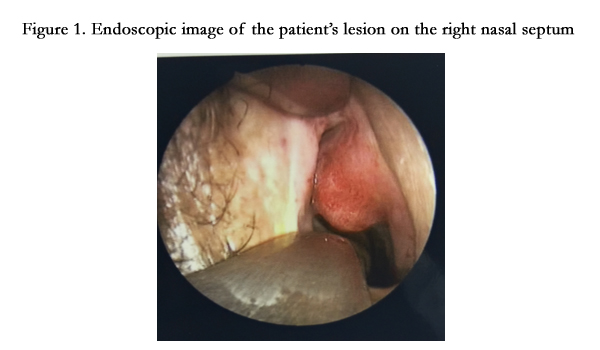
Figure 1. Endoscopic image of the patient’s lesion on the right nasal septum.
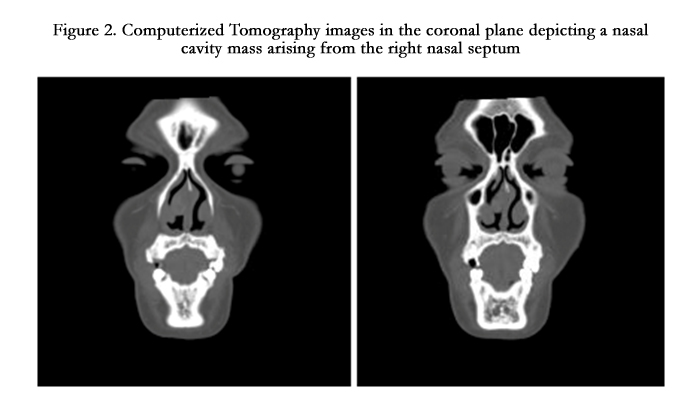
Figure 2. Computerized Tomography images in the coronal plane depicting a nasal cavity mass arising from the right nasal septum.
The patient was taken to the operating room for endoscopic resection. The mass was observed to extend to the superior aspect of the internal nasal valve without involvement of the upper lateral nasal cartilage. The mass was removed en bloc including a wide cuff of normal mucosa circumferentially around the mass before dissecting the mass from the nasal septal cartilage, preserving perichondrium, without disrupting the nasal valve, upper lateral cartilage, or right nasal ala. No septal perforation was noted intraoperatively or at 3 months post operatively. The specimen was sent for permanent pathology. The gross specimen was 3.0 x 2.0 x 1.2 cm in size and tan and pink in appearance with a smooth and glistening surface. H&E stain revealed a well-circumscribed tumor with proliferation of fascicles of smooth muscle cells and surrounding thick-walled vessels with narrow lumens (Figure 3). The endothelial cells lacked pleomorphism, mitosis, nuclear atypia, or necrosis. Immunohistochemistry was positive for SMA, which revealed the smooth muscle cell component, as well as ERG1 (nuclear stain), which highlighted the endothelial cells lining narrow vessel lumens (Figure 4).
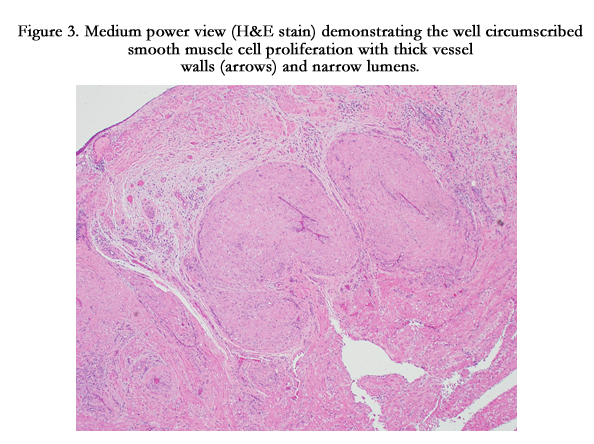
Figure 3. Medium power view (H&E stain) demonstrating the well circumscribed smooth muscle cell proliferation with thick vessel walls (arrows) and narrow lumens.
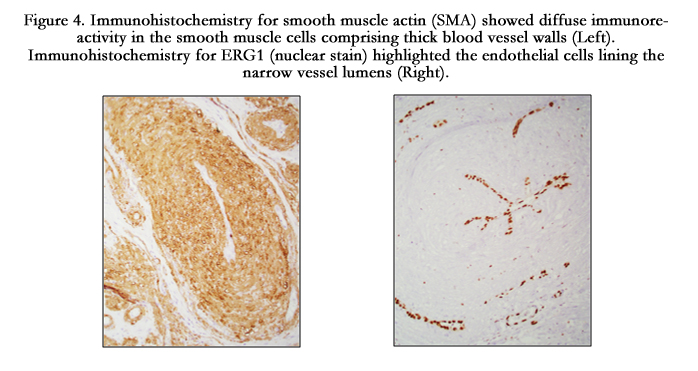
Figure 4. Immunohistochemistry for smooth muscle actin (SMA) showed diffuse immunoreactivity in the smooth muscle cells comprising thick blood vessel walls (Left). Immunohistochemistry for ERG1 (nuclear stain) highlighted the endothelial cells lining the narrow vessel lumens (Right).
Discussion
Sinonasal angioleiomyomas make up less than 1% of leiomyomas in the body [5, 10]. Roughly 10% of these tumors are located in the head and neck region and presenting sites include the nose, auricle, lips, and neck [1, 21]. This slow growing, benign tumor may present as a solitary mass that may or may not be painful. Other typical presenting symptoms may include nasal obstruction, epistaxis, facial pain, recurrent sinusitis, and can be associated with a septal deviation [1]. Angioleiomyoma is not often included in the clinician’s differential diagnosis of an obstructive nasal mass. The differential diagnosis includes both benign and malignant tumors of the nasal cavity including inverted papilloma, nasal angiofibroma, hemangioma, hemangiopericytoma, solitary fibrous tumor, desmoid fibromatosis, peripheral nerve sheath tumors, and sinonasal sarcomas including leiomyosarcoma and rhabdomyosarcoma [1, 22].
The rare nature of these tumors is attributed to the paucity of smooth muscle tissue in the region. Smooth muscle in the nasal cavity is present in blood vessel walls as well as the piloerector muscles of the anterior vestibule [26]. Angioleiomyoma of the nasal cavity appears to present more commonly on the turbinates and nasal vestibules presumably due to the presence of smooth muscle. The nasal septum is understandably an exceedingly rare location for this tumor.
The World Health Organization classifies leiomyomas into three histologic groups: leiomyoma, angioleiomyoma, and epithelioid leiomyoma [10, 26, 27]. Our patient’s specimen was classified as angioleiomyoma by histopathologic examination. The vascular component of this smooth muscle derived tumor may also be classified as solid, venous, or cavernous type based on histological findings [1, 27]; this was not specified in our patient. Immunohistology will reveal expression of alpha smooth muscle actin (SMA) and possibly h-caldesmon, muscle specific actin, desmin, S100, or myoglobin [1, 3].
Literature review reveals that the most common age range for presentation is between 40 and 60 years of age [3, 28, 29]. A female predilection has been suggested in the literature, with reports of a female:male ratio of 3.75:1 [3, 21, 29]. Marioni et al., suggest possible hormone dependence and report a case of a progesterone dependent sinonasal angioleiomyoma [29]. Heet al reported a case of nasal cavity angioleiomyoma that was partially immunoreactive to progesterone receptor [16]. This phenomenon may account for the female preponderance of reported cases [29]. Other risk factors, prognostic factors, and mortality data has yet to be elucidated given the rarity of these lesions.
The treatment of choice appears to be local excision, which may either be performed transnasally or endoscopically with macroscopic margins or by open approach; pre-operative embolization may be considered for large tumors with abundant vascular supply. KTP laser has been used for bloodless ablation [3, 22]. A lateral rhinotomy approach hasbeen described for a large tumor [24]. One case of a particularly extensive tumor in the nasal cavity required craniofacial resection [12].
Our literature review reveals 16 total cases of angioleiomyoma arising from the nasal septum [1, 4-8, 19, 20, 22-25]. This represents 23.5% of angioleiomyomas of the sinonasal cavities reported worldwide. In the English literature, 8 nasal septum angioleiomyomas were reportedly resected transnasally or endoscopically while 1 tumor was resected using an open (lateral rhinotomy) approach. The remainder of reports did not specify the surgical approach. There were no reports of patients requiring reconstruction or a second stage procedure. Recurrent sinonasal angioleiomyoma has been reported on the middle turbinate [3], however, no recurrent lesions have been reported on the nasal septum. Malignant transformation has yet to be reported in the literature for sinonasal angioleiomyomas. The current patient is doing well 3 months post operatively.
Conclusions
Angioleiomyoma of the nasal septum is an exceedingly rare tumor and is a challenge to clinically diagnose. There are 68 cases that have been reported in the English literature worldwide and 16 cases reported on the nasal septum. Diagnosis requires detailed histopathologic examination and the differential includes a variety of epithelial and mesenchymal derived tumors and malignancies. Definitive treatment can include endoscopic resection as well as laser ablation. The literature suggests a possible hormonal influence and a female predilection; however, definite risk factors and prognostic indicators have yet to be described. Angioleiomyoma is not commonly included in the differential diagnosis for an obstructive nasal mass and even less often for a mass of the nasal septum. Despite the rare nature of the tumor, case reports are accumulating and may provide further information regarding risk factors, immunoreactivity, recurrence rates, prognosis, and anatomic sites of presentation.
References
- A Agaimy, M Michal, LDR Thompson, M Michal (2015) Angioleiomyoma of the Sinonasal Tract: Analysis of 16 Cases and Review of the Literature, Head Neck Pathol. 9(4): 463-73.
- MF Maesaka A, Keyaki Y, Nakhashi T (1966) Nasal angioleiomyoma and leiomyosarcoma. Report of two cases. Otologia. 12(1): 42–7.
- AM Bhandarkar, B Ramaswamy, P Jaiprakash, N Chidambaranathan (2015) Recurrent angioleiomyoma of the middle turbinate, BMJ Case Rep. bcr2015210686.
- Bloom DC, Finley JC, Jr, Broberg TG, Cueva RA (2001) Leiomyoma of the nasal septum. Rhinology. 39(4): 233–235.
- Ardekian L, Samet N, Talmi YP, Roth Y, Bendet E, Kronenberg J (1996) Vascular leiomyoma of the nasal septum, Otolaryngol. - Head Neck Surg. 114(6): 798–800.
- MH Barr GD, More IA (1990) Leiomyoma of the nasal septum. J. Laryngol. Otol. 104: 891–3.
- Llorente JL, Suárez C, Seco M, Garcia A (1996) Leiomyoma of the nasal septum: report of a case and review of the literature. 110(1): 65-68.
- Timirlyaleev MKH (1973) Angioleiomyoma of the nasal septum. Vestnik Otorinolaringol 35: 106-110.
- H Daisley (1987) Leiomyoma of the nasal cavity. West Indian Med. J. 36(3):181–3.
- Campelo VE, Neves MC, Nakanishi M, Voegels RL (2008) Nasal cavity vascular leiomyoma: case report and literature review. Braz. J. Otorhinolaryngol. 74(1): 147–150.
- S Burkart, U Schoenenberger (2015) A Rare Differential Diagnosis of a Nasal Tumor: Case Report and Literature Review, Case Reports Otolaryngol. 2015: 4.
- Nicolai P, Redaelli de Zinis LO, Facchetti F, Maroldi R, Antonelli AR (1996) Craniofacial resection for vascular leiomyoma of the nasal cavity. Am. J. Otolaryngol. 17 (5) 340–4.
- L Varghese, S Mathew, K Vijayakumar (2015) Nasal Angioleiomyoma: An Unusual Cause of Epistaxis. Oman Med. J. 30 (4) 303–305.
- Vafiadis M, Kantas I, Panopoulou M, Sivridis E, Exarchakos G (2008) Vascular leiomyoma of the nasal vestibule. Case report and literature review. B-ENT. 4(2): 105–10.
- Melgarejo Moreno P1, Hellín Meseguer D, Sarroca Capell E (1997) [Angioleiomyoma of the inferior nasal turbinate. A case report and review of the literature]. Acta Otorrinolaringológica Española. 48(7): 571–3.
- J He, LN Zhao, ZN Jiang, SZ Zhang (2009) Angioleiomyoma of the nasal cavity: A rare cause of epistaxis, Otolaryngol. Head Neck Surg. 141(5): 663–664.
- J Zhao, H Zhang, J Zhang, Y Pi, M Xu (2015) [Angioleiomyoma with mature adipocytes of nasal vestibule: report of a case]. Zhonghua Bing Li Xue Za Zhi. 44(4) 288–9. http://www.ncbi.nlm.nih.gov/pubmed/25975919
- CH Yi, A Tabaee, B Wang (2015) An Elderly Woman With Left-Sided Acute Epistaxis. JAMA Otolaryngol. Head Neck Surg. 141 (11) 1019–20.
- CRR Navarro, AS Fonseca, JRL de Mattos, NA de Andrade (2010) Angioleiomyoma of the nasal septum. Braz. J. Otorhinolaryngol. 76 (5): 675.
- R Singh, P Hazarika, R Balakrishnan, N Gangwar, P Pujary (2008) Leiomyoma of the nasal septum., Indian J. Cancer. 45 (4): 173–5.
- R Meher, S Varshney (2007) Leiomyoma of the nose. Singapore Med. J. 48(10) 275–276.
- MM Arruda, DY Monteiro, AM Fernandes, V Menegatti, E Thomazzi, RA Hubner, et al., (2014) Angioleiomyoma of the nasal cavity. Int. Arch. Otorhinolaryngol. 18 (4) 409–411.
- Wang CP, Chang YL, Sheen TS (2004) Vascular leiomyoma of the head and neck. Laryngoscope. 114 (4) 661–5.
- GN Purohit, N Agarwal, R Agarwal (2011) Leiomyoma arising from septum of nose. Indian J. Otolaryngol. Head Neck Surg. 63(1) 64–7.
- TM Yoon, HC Yang, YD Choi, DH Lee, JK Lee, SC Lim (2013) Vascular leiomyoma in the head and neck region: 11 years experience in one institution. Clin. Exp. Otorhinolaryngol. 6(3) 171–175.
- Murono S, Ohmura T, Sugimori S, Furukawa M (1998) Vascular leiomyoma with abundant adipose cells of the nasal cavity. Am. J. Otolaryngol. 19(1)50–53.
- QB Hisaoka M, Angioleiomyoma., in: M.F. Fletcher CDM, Bridge JA, Hogendoorn PCW (Ed.) World Heal. Organ. Classif. Tumours Soft Tissue Bone., 4th editio, IARC Press, Lyon, 2013: pp. 120–121.
- T Hachisuga (1984) Angioleiomyoma. A clinicopathologic reappraisal of 562 cases. Cancer. 54(1): 126–130.
- G Marioni, R Marchese-Ragona, S Fernandez, J Bruzon, F Marino, A Staffieri (2002) Progesterone receptor expression in angioleiomyoma of the nasal cavity. Acta Otolaryngol. 122(4): 408–412.





