Aesthethic Complications of Nasal Septum Resection
KB Lipski*, DA Sidorenkov, GA Aganesov, AA Malakhov
Department of Plastic Surgery, I.M. Sechenov First Moscow State Medical University, Trubetskaya Street, Moscow, Russia.
*Corresponding Author
K.B. Lipski,
Department of Plastic Surgery, I.M. Sechenov First Moscow State Medical University,
Moscow 119991, Russian.
E-mail: klipski@mail.ru
Received: September 13, 2016; Accepted: October 12, 2016; Published: October 13, 2016
Citation: KB Lipski, DA Sidorenkov, GA Aganesov, AA Malakhov (2016) Aesthethic Complications of Nasal Septum Resection. Int J Clin Exp Otolaryngol. 2(5), 42-47. doi: dx.doi.org/10.19070/2572-732X-160008
Copyright: KB Lipski© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Violation of nasal breathing mostly related to nasal septum deformation, which is an indication to perform septoplasty. This article represents our observations about the possible cause of aesthetic complications after nasal septum resection; the technique we us for prevention of such complications, clinical cases and treatment results.
2.Introduction
3.Materials and Methods
4.Results
4.1.Case No 1
4.2.Case No 2
5.Conclusions
6.References
Keywords
Secondary Rhinoplasty; Septoplasty; Nasal Septum; Submucosal Resection; Septum Support.
Introduction
The first documented attempts to impact the deviated septum appeared back in 1757. Techniques gradually developed over time. First surgical attempt to influence a deviated septum was undertaken by Adams [1] who started to practice fracturing and splinting the septum. Ingals [15] in 1881 began to use a more radical technique. He removed small triangles of the curved portion of the cartilaginous septum including a mucosal flap and called his technique - "window resection." Krieg (1889) [14] and Boenninghaus (1890) [14] improved this technique by resecting the entire curved portion of the septal cartilage. In case of deeper deviations, resection included a part of the vomer and the perpendicular plate of the ethmoid bone. In the 20th century Freer (1902) [11] and Killian (1904) [17] had offered a new approach - submucosal resection of the deviated septum. It formed the basis of all modern techniques. The era of modern septoplasty originates in the 1940s. Cottle (1952) [5], Goldman (1956) [12] and Smith (1957) [24] have revealed the imperfections of the submucosal resection method and suggested a more conservative removal of bony and cartilaginous structures of the nasal septum. Later Gubisch (1995) [13] updated an extracorporeal septoplasty technique that was invented in 1950s. It included a few stages - extraction, remodeling, renovation and implantation of the septum. Dr. Gubisch suggested a mandatory lock of the septum to the nasal process of maxilla and triangular cartilages.
The most frequent indication for septoplasty is a violation of nasal breathing that usually associates with a deviated septum. According to a literature, the frequency of the nasal septum deformation is sufficiently large. Every adult in 96.5 % of cases has a septal deviation in a varying degree.
Nowadays there are several fundamental surgical techniques and a solid number of its modifications to correct the deviated septum are based on Killian and Voyachek operations.
According to statistics by foreign authors, different aesthetic complications after a septoplasty are observed in 22 % of cases. [9, 20, 21, 27, 28-30] Eighty percent of doctors do not consider it necessary to discuss the possible aesthetic complications after septoplasty with their patients and do not include this item in the written consent [6, 18].
Historically formed the opinion that leaving 1 cm width L-shaped strut after a submucosal resection of altered cartilaginous septum does not lead to a weakening or has little effect on the supporting function of the nose structures.
Recent data from scientific sources disprove this theory and often suggest otherwise [3, 23]. In particular Mowlavi (2006) et al., [26] studied and compared eleven cadaveric materials to calculate mean thickness of the septum along its entire length. Caudal margin of the septum turned out the subtlest part in all specimens.
(Figure 1. Septum thickness ranging from 0.9 mm to 1.2 mm.within one centimeter in caudal region).
Under the influence of various forces: scarring, skin contracture and etc. the remaining dorsal and caudal part of the septum is not able to provide adequate support to the structures of middle and lower third of the nose. Subsequently it can lead to such aesthetic complications as: saddle deformity, loss of nasal tip projection, columellar retraction, the nasal tip and dorsum deviation and secondary nasal breathing violation [16, 30].
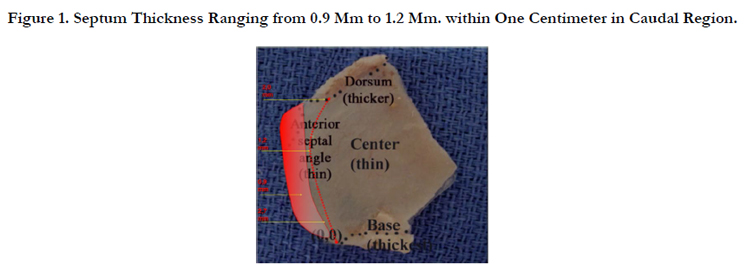
Figure 1. Septum Thickness Ranging from 0.9 Mm to 1.2 Mm. within One Centimeter in Caudal Region.
Materials and Methods
Nowadays conservative resection and preservation of septal cartilage is the main tendency in septoplasty. However most of printed sources agree on one thing that the concept remains unchanged since Killian. The main feature is the removal of abnormal areas of the cartilage leaving a strong cartilaginous support that consists of 1 cm thick strips of the caudal and dorsal edges of quadrangular cartilage plate [2, 7, 8, 10-21].
We believe that one of the fundamental principles of modern septoplasty should be, a prevention of unfavorable aesthetic consequences of this operation. So we made a research how to leave a stronger L-strut after resecting a distorted part of the septum.
For this purpose, the boundary problem on a wedge-shaped cutout in the plate was considered.
The axial forces act onto the plate (two-dimensional stress-strain state). The angle varies in interval [Pi/3,Pi/2]. The plate material is viscoelastic one. The load at the cut boundary we consider as uniformly distributed and symmetric. The maximum of the stress-strain state occurs along the X axis. The presence of the two cut lines (the formation of wedge-shaped incision) leads to the appearance of so called stress concentration points in place where they interface and border areas. The problem considered in the initial period of time, so as to further the negative effect of stress concentration vanishes because of the properties of a viscoelastic medium. The graphical diagram of this problem is represented in Figure 2. (F - forces forming stress concentration points (arrows) at conjugation and border areas).
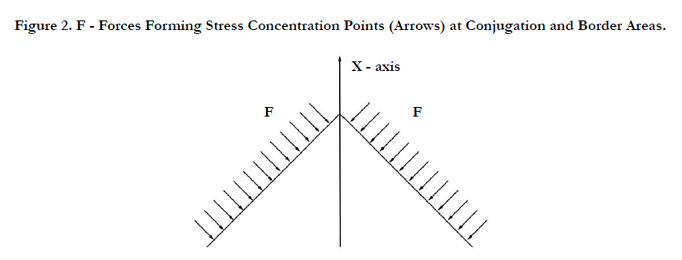
Figure 2. F - Forces Forming Stress Concentration Points (Arrows) at Conjugation and Border Areas.
In the present problem the definition of the stress-strain state in the vicinity of an angle. The problem of the angular opening is of significant practical importance in various technological fields. However, the existing criteria do not lead to a complete clarification of all the aspects arising in problems about the angular incision and obtaining exact analytical solutions.
For a linear crack in an elastic field a quantitative measure features is the stress intensity factor, which exhaustively characterizes the stress field near the crack. Knowing the stress intensity factor, we can say whether the condition of the body (consisting of mostly elastic material) is critical. The problem of finding the stress intensity factor for small cracks in bodies of finite size have been well studied.
For angle incision it is much more complicated: the coefficient of the singularity depends on the angle of the cut and only in the limit coincides with the stress intensity factor, when the neck angle becomes to a bilateral cut (forming a crack). In the case of a complex stressed state for angular incision the stress field has two singular components, so the question remains, what is meant by the stress intensity factor in this case. The situation is exacerbated by the fact that the singularity coefficients are not constants of the material. They depend on the opening of an angle and therefore cannot be determined experimentally.
To describe the stress-strain state in the vicinity of the cut a singular component of the stress field must be extracted, that requires the use of following numerical methods.
On the corner points of the polygonal holes the stress concentration is observed, as is known, to solve these problems, methods of finite differences, finite elements, boundary elements, with various modifications are applied. It let us to obtain more accurate description of the stress distribution in the border of an angular point. For calculation of stress-strain state of the considered problem we applied the finite element method (FEM) using the triangular finite elements of second order approximation. The application of such elements allowed us to increase the accuracy of determination of stresses in the vicinity of the corner points, when the stress field has an integrable singularity. For the numerical solution of the problem we will use the ANSYS package which has received the greatest application in practice of engineering calculations using the FEM with irregular splitting of items. The number of elements where 5000. As described above in the angular points there is a stress concentration, therefore, in solving such problems it is great important the good choice of finite element approximation. Splitting into small enough finite elements leads to a significant deviation of the approximate solution from the exact one on the cut boundary. Therefore, it is necessary to thicken the mesh in regions of high gradients of stresses.
For the estimation of the accuracy degree the obtained solution with the help of the finite element method, was compared with the exact solution for an isotropic plate with a circular hole (Kirsch problem). The maximum deviation of the approximate solution comparing with the exact solution did not exceed 6%. The results of numerical calculations show the presence of areas of stress concentration near the corner point, which in turn may lead to deformation, giving rise to the formation of cracks and fractures. Distancing from a given point (15% of the diameter of the cut out) stresses have linear distribution, this coincidence with the solution obtained by an analytical method for circular section. Also we should note the formation of the stress forming at border areas of the cutout, which may cause the violation of the integrity of the medium and formation of micro cracks and deformation defects.
A numerical calculation confirms that the increase in the curvature of the contour of the cutout compared to circular outline contour increases the concentration of stresses, the most significant in corner points of the border areas. However, the stress concentration fades out distancing from the border.
By shifting the obtained mathematical calculations to practice, we can state the following. Traditionally submucosal resection of the septum is performed leaving an L-strut. This strut is represented by two stripes of cartilage usually articulated at right angle, forming a notch. (Figure 3. Submucous resection of the septum. Wedge-shape cutout. Cutting lines are marked with red arrows. Cartilaginous septum is removed (black arrow)).
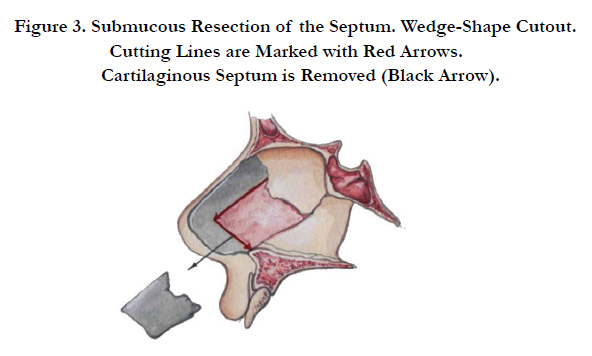
Figure 3. Submucous Resection of the Septum. Wedge-Shape Cutout. Cutting Lines are Marked with Red Arrows. Cartilaginous Septum is Removed (Black Arrow).
The presence of two cut lines leads to the appearance of stress concentration points, which is enhancing by the action of external forces and is mostly pronounced in lines conjugation and border areas. (Figure 4. Stress concentration at the junction of two cut lines. Cartilaginous septum is removed (black arrow). Blue arrows indicate the external forces that increasingly grow approaching the tip of the nose. Red circles denote the points of stress concentration, which reaches its maximum at the point of cut conjugation.) This promotes the formation of cracks and fractures that may eventually lead to deformation of the entire structure.
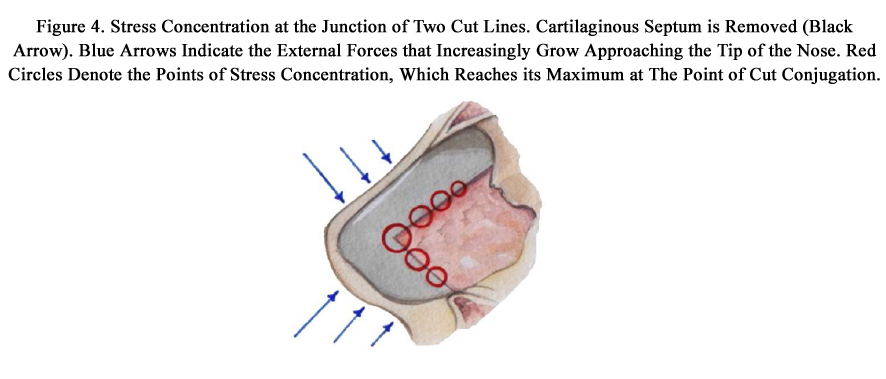
Figure 4. Stress Concentration at the Junction of Two Cut Lines. Cartilaginous Septum is Removed (Black Arrow). Blue Arrows Indicate the External Forces that Increasingly Grow Approaching the Tip of the Nose. Red Circles Denote the Points of Stress Concentration, Which Reaches its Maximum at The Point of Cut Conjugation.
We can exclude the presence angular points by making a continuous rounded (semicircular) cutting line thereby distributing stress evenly over the length of the cutout. (Figure 5. Semicircular incision (red arrow). Uniform stress distribution along incision (red circles). Blue arrows indicate the external forces that increasingly grow approaching the tip of the nose).
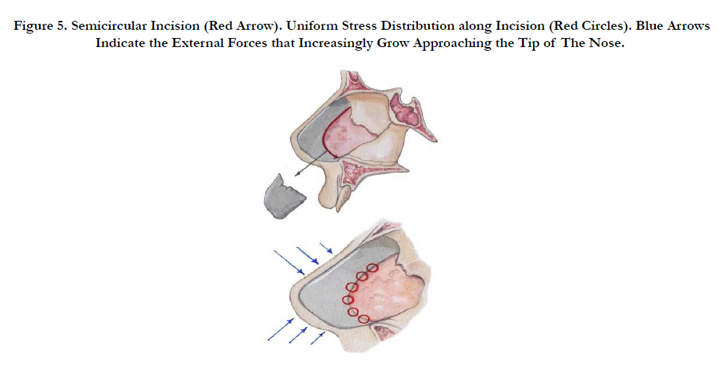
Figure 5. Semicircular Incision (Red Arrow). Uniform Stress Distribution along Incision (Red Circles). Blue Arrows Indicate the External Forces that Increasingly Grow Approaching the Tip of The Nose.
Semicircular cut leaves more intact cartilage that also prevents future deformation of the septum. The stress force dissipates evenly over the entire length of the cutout preventing the formation of maximum stress area, which can lead to the destruction of the cartilage structure.
Examining the cross section in the area of maximum stress, i.e. at the point of articulation of the cut lines, we can observe that as to semicircular cut - sectional area is proportional to the length of the green segment, but in case of a wedge-shaped cut – section area is proportional to the length of the red segment. Accordingly, a cross-sectional area is smaller in the red segment, thus the stress force and the probability of failure during the equal external impact is higher. (Figure 6. Cross sectional area for different cutouts. Green and red segments respectively indicate that the cross-sectional area in case of semicircular cut is greater than in the wedge-shape cutout. Blue arrows indicate the external forces acting on the septum).
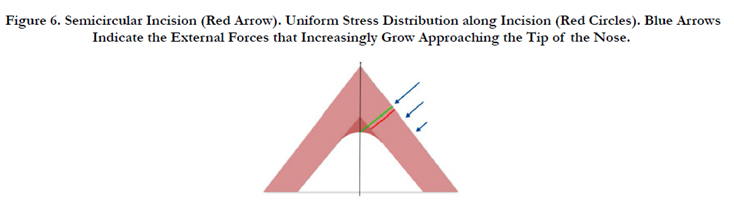
Figure 6. Semicircular Incision (Red Arrow). Uniform Stress Distribution along Incision (Red Circles). Blue Arrows Indicate the External Forces that Increasingly Grow Approaching the Tip of the Nose.
Results
During 2013 have had 37 secondary rhinoseptoplasty cases. In 30 cases we observed a loss of support ability of the septal cartilage that was associated with interference on the nasal septum. 40% of these patients have had septoplasty performed by otorhinolaryngologists, the remaining patients have had rhinoseptoplasty performed elsewhere. In all these cases, we performed a septum reconstruction. In our practice we always use the method of extracorporeal septoplasty by Wolfgang Gubisch [13].
Patient K. '54. (Figure 7. Patient K. '54. Before. Saddle deformity and columellar retraction). In the age of eighteen a septal cartilage resection was performed because of nasal breathing problems. She turned to our clinic with complaints of difficulty in nasal breathing and retraction of the nasal dorsum. In our opinion it was due to lack of support ability of septal cartilage. During the revision we discovered a septum fragment that was not be able to provide full support for the structures of the external nose. (Figure 8. The remaining part of the septum after it’s resection.). We performed the nasal septum reconstruction using ear cartilage grafts with positive functional and aesthetic results in follow up period. (Figure 9. Patient K. before and 12 month follow up period after the septum reconstruction with concha cartilage).
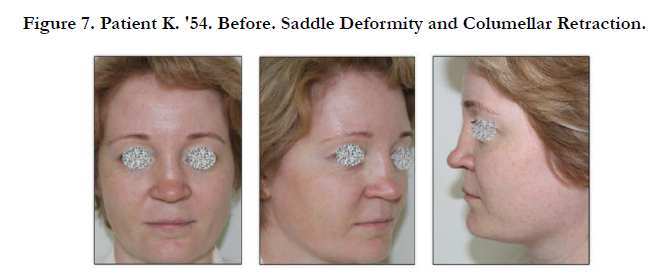

Figure 7. Patient K. '54. Before. Saddle Deformity and Columellar Retraction.
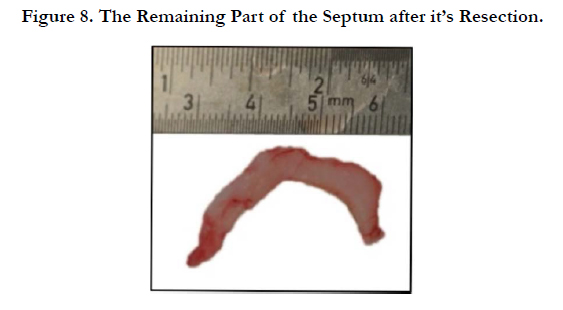
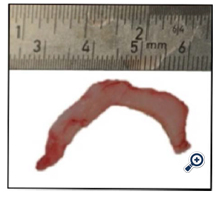
Figure 8. The Remaining Part of the Septum after it’s Resection.
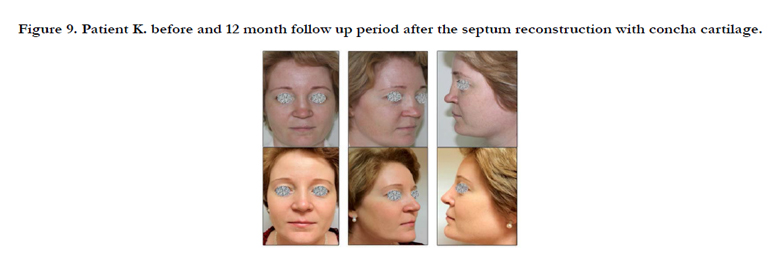

Figure 9. Patient K. before and 12 month follow up period after the septum reconstruction with concha cartilage.
Patient G. ‘23. (Figure 10. Patient K. ’24. Before. Saddle deformity, nasal dorsum and tip deviation to the right.). In the age of eighteen-month she got nose trauma and had an operation. After the surgery she noticed worsening of nasal breathing, dorsum retraction, tip deviation to the right. We performed nasal septum reconstruction with fixation to the nasal spine and upper lateral cartilage. (Figure 11. Fixation of the septum to the nasal spine). Which resulted in favorable functional and aesthetic results. (Figure 12. Patient. G. Before and 12 moth after the septum reconstruction).
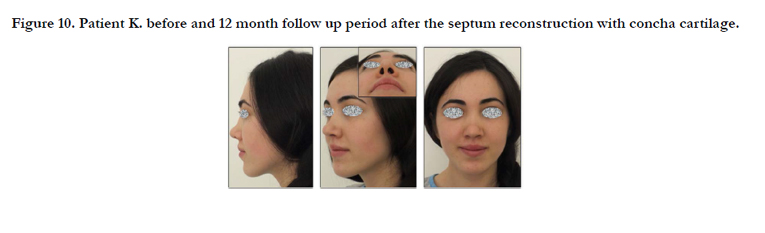

Figure 10. Patient K. before and 12 month follow up period after the septum reconstruction with concha cartilage.


Figure 11. Patient K. Before and 12 Month Follow Up Period after the Septum Reconstruction with Concha Cartilage.
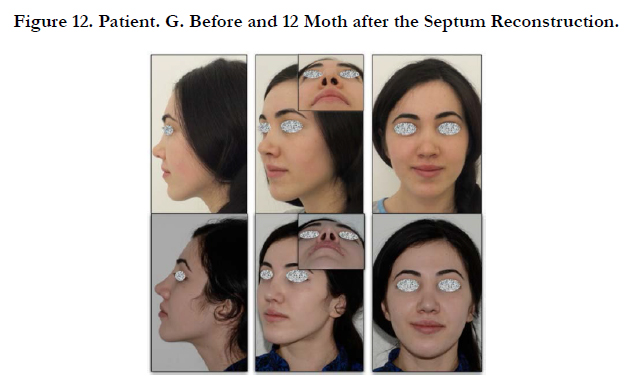

Figure 12. Patient. G. Before and 12 Moth after the Septum Reconstruction.
Conclusions
On the basis of the conducted research it can be concluded that the most solid will be cut with the contour, ensuring the constancy of the contour of stresses.
Making a semicircular cut contributes to the uniform distribution of the forces acting on the septum. Numerical results confirm the positive effect given by the rounding of the cut.
It should also be noted that the proposed methodology for rounding the cut has a proven positive effect when used in the problem on the lowing of the stress concentrations at the mechanisms, cuts in building structures and the development of rocks, where these problems are typical.
Thus, it is confirmed that the proposed solution conducts to stabilization of the stress-strain state at the cut out and it’s border areas that leads to a significant reduction in the risk of cracking and the occurrence of fractures, that, in our opinion, reduces the risk of possible aesthetic complications associated with violation of the septum support ability.
References
- Adams W (1875) The treatment of the broken nose by forcible straightening and mechanical Rententive apparatus. BMJ. 2(770): 421-422.
- Anand K, Devaiah, Bounmany Kyle Keojampa (2009) Surgery of the nasal septum . Rhinology and facial plastic surgery. 181-185.
- Adams WP Jr, Rohrich RJ, Hollier LH, Minoli J, Thornton LK et al., (1999) Anatomic basis and clinical implications for nasal tip support in open versus closed rhinoplasty. Plast Reconstr Surg. 103(1): 255–264.
- Bernstein L (1973) Submucous operations on the nasal septum. Otolaryngol Clin North Am. 6(3): 675-692.
- Cottle MH (1958) The maxilla-premaxilla approach to extensive nasal septum surgery. Arch Otolaryngol Head Neck Surg. 68(3): 301-313.
- Daws PJD (1994) Informed consent: questionnaire survey of British Otolaryngologists. Clin Otolaryngol Allied Sci. 19(5): 388–393.
- Dhingra PL (2007) Diseases of ear, nose and throat. (4th Edn). 140-425.
- Dingman RO, Natvig P (1977) The deviated nose. Clin Plast Surg. 4(1): 145-152.
- Dommerby H, Rasmussen OR, Rastborg J (1985) Long-term results of septoplastic operations. Otorhinolaryngol. 47(3): 151-157.
- Edwards N. Septoplasty (1975) Septoplasty. Rational surgery of the nasal septum. J Laryngol Otol. 89(9): 875-897.
- Freer OT (1902) The correction of deflections of the nasal septum with minimum of traumatization. JAMA. 38(10): 636-642.
- Goldman IB (1956) New techniques in the surgery of the deviated nasal septum. Arch Otolaryngol. 64(3): 183-189.
- Gubisch W (1995) The extracorporeal septum plasty: a technique to correct difficult nasal deformities. Plast Reconstr Surg. 95(4): 672-682.
- Hinderer KH (1971) History of septoplasty. Fundamentals of anatomy and surgery of the nose. Birmingham, Alabama: Aesculapius.
- Ingals EF (1882) Deflections of the nasal septum. Transactions of the American Laryngology Association. 4: 61-69.
- Johnson CM, Toriumi DA (1990) Case Approach to Open Structure Rhinoplasty. (1st Edn), Philadelphia: W.B. Saunders .
- Kilian G (1904) Die submucose Fenster Resektion der Nasescheidewand. Arch Laryngol Rhinol. 19(16): 362-387.
- Maran AGD (1990) Informed consent in head and neck surgery. Clin Otolaryngol Allied Sci. 15(4): 293– 298.https://www.ncbi.nlm.nih.gov/pubmed/2225495
- Papel MD ( 2007) Facial plastic and reconstructive surgery. Otolaryngology. 106(1): 1-9.
- Peacock MR (1981) Submucous resection of the nasal septum. J Laryngol Otol. 95: 341-356.
- Phillipps JJ (1991) The cosmetic effects of submucous resection. Clin Otolaryngol Allied Sci. 16(2): 179-181.
- Planas J (1977) The twisted nose. Clin Plast Surg. 4(1): 55.
- Daudia A , Sithole J, Mortimore S, Alkhaddour U (2006) Prospective objective study of the cosmetic sequelae of nasal septal surgery. Acta Otolaryngol. 126: 1201–1205.
- Tardy ME (1982) Reconstructive surgery of the deviated septum and nose. Richards Manufacturing Co Inc, US.
- Roy B. Sessions, Thomas Troost (2005) The nasal septum. Otolaryngology- Head and Neck Surgery. Mosby. 948–1001.
- Mowlawi A (2006) Septal cartilage defined: implications for nasal dynamics and rhynoplasty. Plast Reconstr Surg. 117(7): 2171-2174.
- Stocksted P (1969) Longterm results, following plastic septum surgery. Rhinol. 7: 53-61.
- Thomas JN (1978) S.M.R.--a two-year follow-up survey. J Laryngol Otol 92(8): 661-666.
- Tzadik A, Gilbert SE, Sade J (1988) Complications of submucous resection of the nasal septum. Arch Otolaryngol. 245(2): 74-76.
- Vuyk HD, Langenhuijsen KJ (1997) Aesthetic sequelae of septoplasty. Clin Otolaryngol Allied Sci. 22: 226-232.





