PPAR α/γ Agonist in Management of Diabetic Dyslipidemia: A Review
Vaishnav RA1*, Mistry CB2, Shah MH3
1 Clinical Research Director, Harmony Clinic and Research Centre and Vadodara Stroke Clinic 5, Vihar Society - Akota, Vadodara, Gujarat, India.
2 Pharmacologist, Department of Pharmacology, Medical College Baroda, The M.S. University of Baroda, Sayajigunj, Vadodara, Gujarat, India.
3 Consultant Endocrinologist, Harmony Clinic and Research Centre, Vadodara, Gujarat, India.
*Corresponding Author
Dr. Radhika A. Vaishnav, Ph.D,
Clinical Research Director,
Harmony Clinic and Research Centre and Vadodara
Stroke Clinic 5, Vihar Society - Akota, Vadodara, Gujarat,
Post Code : 390021, India.
E-mail: radhikavaishnav@gmail.com
Article Type: Review Article
Received: March 11, 2015; Accepted: April 15, 2015; Published: April 17, 2015
Citation: Vaishnav RA, Mistry CB, Shah MH (2015) PPAR α/γ Agonist in Management of Diabetic Dyslipidemia: A Review. Int J Clin Pharmacol Toxicol, 4(1) 143-149. doi: dx.doi.org/10.19070/2167-910X-1500026
Copyright: Vaishnav RA© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Cardiovascular diseases are major contributors of mortality and morbidity in patients with type 2 diabetes mellitus (T2DM), while dyslipidemia and hyperglycemia are key modifiable risk factors to prevent coronary artery disease (CAD).
Although healthy diet, regular physical activity and maintaining a normal body weight are advised, patients generally require single or multiple drugs to treat T2DM. Moreover, patients with T2DM are prone to atherogenic diabetic dyslipidemia (ADD), which is characterized by elevated triglyceride, small dense LDL particles and low High-density lipoprotein (HDL) cholesterol.
Even though low-density lipoprotein cholesterol (LDL) remains the primary target of therapy, non-high density lipoprotein (non-HDL) cholesterol is as an important parameter to be considered in clinical practice. Unfortunately, high-dose statin therapy is not advised for long term, as it can increase risk of new onset T2DM. On the other hand, glitazars are newer molecules having dual peroxisome proliferator-activated receptors (PPAR) α/γ agonistic action that can improve lipid profile with improvement of insulin sensitivity.
In conclusion, the overall safety of saroglitazar is acceptable due to minimal side effects, but improvement of β cell function, effect on insulin sensitivity by analysis of insulin resistance index by using the homeostatic model assessment (HOMAIR) and long term cardiovascular benefits like atherosclerotic plaque stabilization or regression need to be confirmed.
2.Introduction
3.Global Scenario of Diabetes and Diabetic Dyslipidemia
4.Diabetic dyslipidemia: A Modifiable Risk Factor for Cardiovascular Disease
5.Management of Diabetic Dyslipidemia
5.1.Definition of Diabetic Dyslipidemia
5.2.Mechanism of Dyslipidemia in Patients with type 2 Diabetes Mellitus
5.3.Diabetic Dyslipidemia: An Established Risk Factor for Coronary artery Disease
5.4.Therapeutic approach for Diabetic Dyslipidemia
6.Treatment of diabetic dyslipidemia by PPAR α/ γ agonists
6.1.Peroxisome proliferator activated receptors (PPAR) α, β/δ and γ
6.2.PPAR α / γ agonist: Glitazars
6.3.Advantages of glitazar
6.4.History and development of Glitazar
6.5.Limitations of fibrate and thiazolidinedione (TZD) combination
6.6.Safer glitazar: Saroglitazar
6.7.Safety and Efficacy of Saroglitazar
7.Comparative Long-term Outcome Study of Saroglitazar
8.Conclusion
9.References
Keywords
Atherogenic Diabetic Dyslipidemia (ADD); Cardiovascular Diseases (CVD); Insulin Resistance; Low-Density Lipoprotein Cholesterol (LDL); Peroxisome Proliferator - Activated Receptors (PPAR); Triglyceride (TG); Safety.
Introduction
Cardiovascular diseases (CVD) are the major contributors of mortality and morbidity in both industrialized countries and emerging nations, and 80% of the CVD deaths occur in low and middle income countries. According to the WHO’s world health statistics, it was reported that around 17.3 million CVD deaths globally occurred in the year 2008, with an anticipated increase to annual death of 23.3 million by 2030 [1]. Furthermore, diabetes and dyslipidemia are two important risk factors that should be controlled as the presence of two factors concomitantly increases CVD risk by 3-4 folds [2, 3].
Global Scenario of Diabetes and Diabetic Dyslipidemia
According to data of the World Health Organization (WHO), 347 million people worldwide have diabetes and more than 80% of diabetes deaths occur in low-and middle-income countries [4]. On the other hand, statistics of WHO projects that death due to diabetes will double between 2005 and 2030, and diabetes will be the 7th leading cause of death in 2030. Healthy diet, regular physical activity, maintaining a normal body weight can prevent or delay the onset of type 2 diabetes [5].
Similarly, Indian Council of Medical Research-India Diabetes (ICMR–INDIAB) study was carried out to provide accurate and comprehensive state and national level data on prevalence of diabetes and dyslipidemia in Indian population by following National Cholesterol Education Program (NCEP) guideline [6].
As per ICMR–INDIAB study, it was concluded that, 13.9% had hypercholesterolemia, 29.5% had hypertriglyceridemia, 72.3% had low HDL-C, 11.8% had high LDL-C levels and 79% had abnormalities in one of the lipid parameters. Moreover, urban residents had the highest prevalence of lipid abnormalities compared to rural residents [7].
In addition to above findings, low HDL-C was the most common lipid abnormality (72.3%), which was present as an isolated abnormality. On the other hand, common significant risk factors for dyslipidemia were obesity, diabetes and hyperglycemia. After all the prevalence of dyslipidemia is high in India, which calls for urgent lifestyle intervention strategies to prevent and manage this important cardiovascular risk factor [7].
Diabetic dyslipidemia: A Modifiable Risk Factor for Cardiovascular Disease
Over the period of time, diabetes can damage blood vessels of the heart, brain, eyes, kidneys, and nerves; consequently it can increase the risk of heart disease, stroke, retinopathy or neuropathy. Similarly, it was noted that 50% of people with diabetes die of CVD [8]. Moreover, diabetes doubles the overall risk of dying compared to their peers without diabetes [9-11]. On the other hand, comprehensive management of modifiable CVD risk factors can be done by controlling both glycemic and lipid parameters [12].
Management of Diabetic Dyslipidemia
The term diabetic dyslipidemia essentially refers to atherogenic dyslipidemia occurring in patients with type 2 diabetes, which is characterized by elevated triglyceride, small dense LDL particles, and low HDL-cholesterol concentrations. Moreover, diabetic dyslipidemia is considered as one component of the metabolic syndrome, which can be treated by overcoming insulin resistance [13].
In patients with type 2 diabetes mellitus, the number of LDL particles are usually greater than those reflected by LDL-cholesterol levels, because LDL particles are small and partially depleted of cholesterol. Moreover, the combined adverse atherogenic effect of elevated LDL, triglyceride and other risk factors of the metabolic syndrome exacerbates atherosclerosis due to the significant increase in small dense LDL cholesterol in patients with type 2 diabetes mellitus [13].
In the same way, insulin resistance at the level of adipocyte lead to increased free fatty acid efflux, which is central to the pathogenesis of atherogenic diabetic dyslipidemia (ADD) and this results in increased very low-density lipoprotein (VLDL) cholesterol from the liver facilitated by increased synthesis of apolipoprotein B (Apo B). As a result, there is development of ADD in a patient with type 2 diabetes mellitus (T2DM) that is characterized by a triad of high triglycerides (TG), low high-density lipoprotein (HDL) cholesterol and elevated small, dense low-density lipoprotein (LDL) particles [14].
As shown in Figure 1, cholesterol ester transfer protein plays arole in transferring triglycerides from VLDL particles to HDL and LDL, which result in increased Apo A1 containing small dense HDL and Apo B containing small dense LDL particles. The triglyceride-enriched HDL is subsequently hydrolyzed by hepatic lipase or lipoprotein lipase resulting in low HDL and Apo A-I, which is filtered by the renal glomeruli for degradation in renal tubular cells [15].
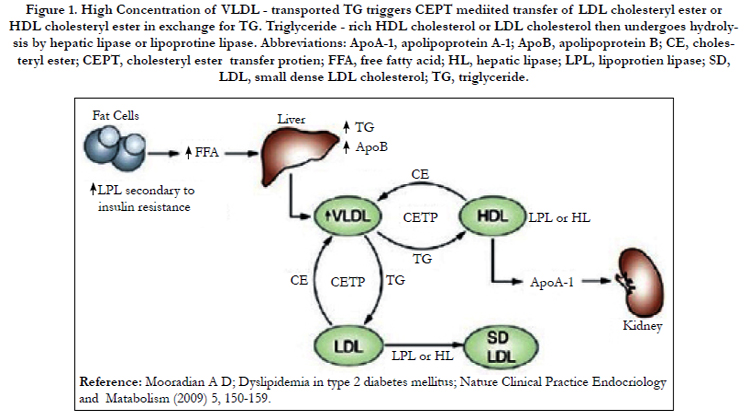

Figure 1. High Concentration of VLDL - transported TG triggers CEPT mediited transfer of LDL cholesteryl ester or HDL cholesteryl ester in exchange for TG. Triglyceride - rich HDL cholesterol or LDL cholesterol then undergoes hydrolysis by hepatic lipase or lipoprotine lipase. Abbreviations: ApoA-1, apolipoprotein A-1; ApoB, apolipoprotein B; CE, cholesteryl ester; CEPT, cholesteryl ester transfer protien; FFA, free fatty acid; HL, hepatic lipase; LPL, lipoprotien lipase; SD, LDL, small dense LDL cholesterol; TG, triglyceride.
In clinical practice, total cardiovascular disease risk can be assessed by Framingham Risk Score (FRS), which is modified according to family history of premature coronary artery disease (CAD) [16].
On the other hand, low-density lipoprotein cholesterol remains the primary target of therapy, but in clinical practice, non-HDL cholesterol need to be emphasized as an atherogenic component. If lipid management is not done properly to prevent progression of atherosclerotic vascular blockage, angioplasty, stent placement or coronary artery bypass grafting can be required to treat ischemic heart disease (IHD) [17].
On the other hand, one meta-analysis was executed by compiling eight randomized controlled trails of statin named Simvastatin Survival Study (4S), Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS), Long-term Intervention with Pravastatin in Ischemic Disease (LIPID), Collaborative Atorvastatin Diabetes Study (CARDS), Treating to New Targets (TNT), Incremental Decrease in Clinical Endpoints Through Aggressive Lipid Lowering (IDEAL), Stroke Prevention by Aggressive Reduction of Cholesterol Levels (SPARCL) and Justification for the Use of Statins in Prevention (JUPITER) trials.
Overall analysis of these 38,153 patients’ data, it was unveiled that for one standard deviation (SD) increase in LDL, non-HDL and Apo-B, there was an increase in CV risk by 13%, 16% and 14% respectively. Furthermore, there is growing evidence which supports the control of non HDL - cholesterol and high triglyceride for overall CVD risk reduction [17-19].
According to recent American College of Cardiology/American Heart Association (ACC/AHA 2013) guideline for the management of diabetic dyslipidemia, following four groups of patients were recommended for moderate to high intensity statins for prevention of atherosclerotic cardiovascular disease (ASCVD).
- Patients with clinical ASCVD.
- Primary elevations of LDL–Cholesterol (LDL-C) >190mg/dL.
- Patients with diabetes aged 40 to 75 years with LDL– C 70 to189mg/dL and without clinical ASCVD.
- Patients without clinical ASCVD or diabetes with LDL–C 70 to 189mg/dL and estimated 10-year ASCVD risk >7.5%[13].
Similarly, the American Association of Clinical Endocrinologists guideline (AACE-2013) had suggested that along with statin, nonstatin agent may be required to bring down the uncontrolled lipid parameters to the acceptable level [20].
In addition to the above guidelines, the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults - Adult Treatment Panel III (NCEP ATP III) guideline had suggested that therapeutic lifestyle changes (TLC) should be suggested to the patient and should be subsequently managed by intensifying statin therapy and other non-statin medications. Moreover, after achieving the primary goal of LDL, if TG is not below 200mg/dL, non HDL should be considered as a secondary goal [13, 20].
Similarly, European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) guidelines for the management of dyslipidemia emphasize on giving priority to the management of triglyceride (TG). After all TG is an established risk factor of CAD and fasting TG level less than 150mg/dL (< 1.7 mmol/L) is desirable [21].
On the whole, all these guidelines suggest that in subjects with high total CVD risk, after the primary goal of LDL management is achieved, TG lowering therapy should be initiated if TG levels are > 200mg/dL in patients who cannot lower them by lifestyle measures alone. Hence, the use of statins as the primary drug in diabetic dyslipidemia is valid and several guidelines emphasize the comprehensive management of overall lipid parameters like non- HDL and TG [13, 22].
The American Diabetes Association recommends an LDLcholesterol goal of less than 100mg/dL in most diabetic patients [22]. Besides this, the ADA recommends a combination of LDLlowering therapy with therapeutic lifestyle changes (TLC) to lower LDL levels to control atherogenic dyslipidemia and the addition of fibrate will be required to an LDL-lowering therapy, if LDL-C is not controlled. After all, the benefit of improvement of lipid profile by combining fibrate group of drug with an LDL-lowering agent like statin, need to be superior than risk of severe myopathy [13].
Statins have the advantage of lowering VLDL cholesterol as well as LDL cholesterol; thus they can assist in managing non-HDLcholesterol goal when triglyceride levels are ≥ 200mg/dL. Moreover, fibrates can benefit by reduction in CHD risk and it can be used in patients with high TG not controlled by monotherapy with statin [13, 21].
After all, combination of statin with fibrate is advisable in patients with diabetes who have atherogenic dyslipidemia but it can precipitate myopathy and myalgia. On the contrast, in a pooled analysis of data from the five statin trials with 32,752 participants without diabetes at baseline, 2749 developed diabetes. On subsequent analysis in this study, it was detected that intensive-dose statin therapy was associated with an increased risk of new-onset diabetes compared with moderate-dose statin therapy [23].
In addition to fibrate and statin, nicotinic acid also has a favorable effect on diabetic dyslipidemia, but recent clinical trials in patients with diabetes have suggested that low doses of nicotinic acid accompanied by only modest improvement in glucose control with no changes in glycated hemoglobin (HbA1c). Unfortunately, nicotinic acid therapy can increase insulin resistance and clinical experience has shown that in rare instances, diabetic dyslipidemia may worsen by nicotinic acid therapy [13].
Treatment of diabetic dyslipidemia by PPAR α/ γ agonists
PPAR-α, PPAR- γ and PPAR-β/δ are transcription factors that regulate gene transcription by binding to specific DNA response elements upon ligand activation and heterodimerization with the 9-cis retinoic acid receptor. As a result of selective activation of ligand, different receptor conformations are adopted, leading to different co-activator recruitment and subsequent effects on gene expression. Even though all the PPAR agonists are from the same pharmaceutical class, their biological activity varies widely based on selective alpha or gamma modulation [24, 25].
As shown in Figure 2, PPAR-α regulates expression of genes encoding enzymes and transport proteins controlling lipid metabolism and is expressed predominantly in tissues with a high capacity for fatty acid oxidation like liver, heart, skeletal muscle, brown fat, and kidney [26].
Activation of PPAR-α receptors leads to:
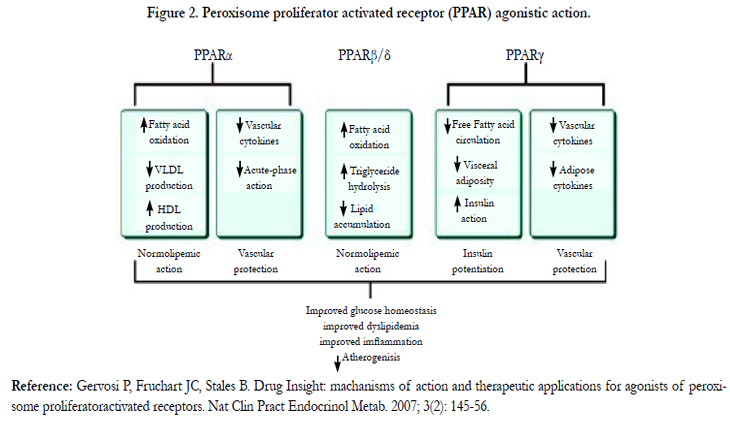
Figure 2. Peroxisome proliferator activated receptor (PPAR) agonistic action
- Fatty acid (FA) oxidation and cellular FA uptake in liver and heart.
- Improves lipoprotein metabolism, reducing VLDL-C and enhancing the catabolism of TG-rich lipoprotein particles.
- Modulates the expression of HDL-C apolipoprotein genes for Apo AI and Apo AII.
- Enhances reverse cholesterol transport via direct effects on macrophage cholesterol efflux transporters ATP binding cassette transporter A1 (ABCA1) and scavenger receptor BI (SR-B1).
- Improves glucose homeostasis by insulin sensitizing action.
- Recent studies showed that PPAR-α can improve pancreatic β cell function [26-28] (Figure 2).
On the other hand, PPAR-γ is mostly expressed in adipose tissue, but it is also present in inflammatory cells (e.g. monocytes, macrophages), mucosa of the colon and cecum, the placenta, and lowest in skeletal muscle and liver. PPARγ not only promotes pre-adipocyte differentiation, but also induces adiponectin expression, which increases fatty acid oxidation by activation of the AMP-activated protein kinase pathway and down regulates the expression of genes encoding resistin and tumor necrosis factor together contributing to reduced insulin resistance [29].
The major actions of PPAR- γ activation are:
- Pre-adipocyte differentiation.
- Stimulation of the storage of FAs in adipocytes.
- Improvement of insulin sensitivity by increased storage of FAs into adipose tissue resulting in decreased plasma FA concentration and relieving lipotoxicity in skeletal muscle, liver and pancreas.
- In addition, PPAR- γ can increase insulin sensitivity by regulating adipocyte hormones, cytokines and proteins that are involved in IR. Similarly, it down regulates the expression of genes encoding resistin and tumor necrosis factor, whereas it induces adiponectin expression, which increases FA oxidation by activation of the AMP-activated protein kinase pathway [30, 31] (Figure 2).
Glitazars are dual peroxisome proliferator-activated receptors (PPAR) α/γ agonists that can improve the lipid profile and glycemic parameters by insulin sensitizing action, similar to a combination of a fibrate and a thiazolidinedione (TZD) [23]. Glitazars have PPARα agonistic action, similar to fibrates that can lower plasma triglycerides and increase HDL-C. Moreover, due to their PPARγ agonistic action like TZDs, they can increase insulin sensitivity and improve glycemic control [32, 33].
Glitazar can reduce cardiovascular risk factors of type 2 diabetes by providing dual management of dyslipidemia and hyperglycemia. Furthermore, it can improve compliance of patients by reducing the pill burden for treatment of type 2 diabetes mellitus [33].
In the past, several PPAR agonists like glitazars, TZD and non- TZD molecules were developed, but all molecules were not successful as some had caused an elevation in creatinine, cardiovascular toxicity or bladder tumors during preclinical or clinical study. Consequently, previous glitazar with potent PPAR α/γ agonism, were approved for clinical trials, but all were discontinued due to safety concerns at preclinical or clinical stage [33, 34].
On the whole, depending on their molecular structure, glitazar exert dual action with varying degrees of PPAR α and PPAR γ activism as shown in Figure 3. Although these tested molecules resulted in adverse events, these have been compound specific and of diverse origin e.g. increase in adipose tissue, urothelial, renal, or cardiac toxicity with different glitazars. In spite of failure of older glitazars, there was a rising hope of a potential drug that could be free from these side effects and yet have a positive effect on insulin sensitivity for correction of diabetic dyslipidaemia (Table 1).
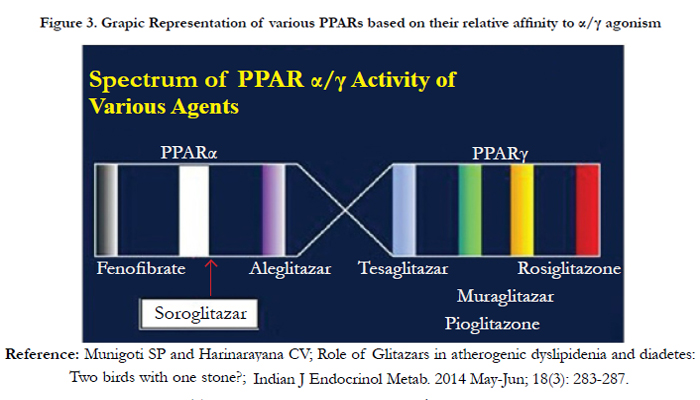
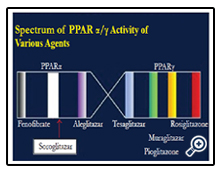
Figure 3. Grapic Representation of various PPARs based on their relative affinity to α/γ agonism
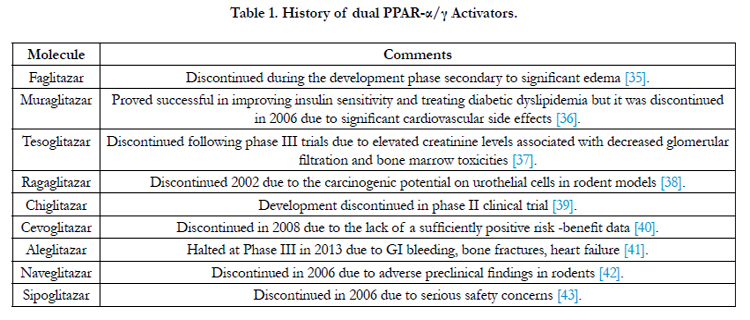

Table 1. History of dual PPAR-α/γ Activators.
The combination of fibrate and TZD therapy is theoretically appealing, but the practice of this approach has been more problematic because fibrates carry a risk of increase in creatinine level and possible myopathy with the statin, while TZDs are prone to cause osteoporosis, fluid retention with possible risk of heart failure [13, 22].
Saroglitazar is a molecule with dual PPAR α/γ agonism, having a balance of binding such that the therapeutic dose range gives optimal biological effects of both PPARα and PPARγ-mediated actions [34].
The phase I study of saroglitazar was a randomized, double-blind, placebo-controlled, single-center study to evaluate the pharmacokinetics, safety and tolerability of saroglitazar under fasting conditions in healthy subjects. Saroglitazar was well absorbed after oral administration with linear pharmacokinetics and it was not excreted in urine, indicating that it has a non-renal route of elimination [44]. Moreover, preclinical studies have shown that saroglitazar is mainly eliminated by the hepatobiliary route and it was found safe and well tolerated up to a 128 mg oral dose with a proposed therapeutic dose of 4mg [44].
On the other hand, phase III clinical trial included prospective randomized safety and efficacy study of saroglitazar named PRESS V and PRESS VI.
According to PRESS V clinical trial, a multi-centric, double blind study was carried out for 12 weeks to evaluate the safety and efficacy of 2mg and 4mg of saroglitazar compared to 45mg of pioglitazone in patients with diabetic dyslipidemia. In this study, subjects with T2DM and dyslipidemia, which not controlled by the lifestyle modifications and TG > 200 to 400mg/dl were recruited, and total 122 subjects were enrolled in the study, and after a run in period of 2 weeks, treatment was given for 24 weeks and further 24 weeks followed up was carried out. At the end of 24 weeks, up to 45% reduction in triglyceride was observed in 4 mg saroglitazar arm, which was significant compared to baseline and to pioglitazone arm [45].
In addition to TG reduction, significant reduction of lipid parameters like LDL-cholesterol, VLDL-cholesterol, total cholesterol, Apo-B with significant reduction in glycemic parameters was observed in saroglitazar arm compared to pioglitazone arm. Conversely, there was no increase in inflammatory markers, muscletoxicity, weight gain or impairment of renal or liver function in the saroglitazar arm [47, 48].
According to PRESS VI clinical trial, a prospective, multicenter, double-blind, placebo controlled, three arm study was carried out for 16 weeks in subjects with hypertriglyceridemia (>200 and <500mg/dL) with T2DM not controlled with atorvastatin 10mg. In short, the study consisted of a run in period of 4 weeks with lifestyle modification followed by 12 weeks of treatment with saroglitazar 2mg or 4mg versus placebo [45].
Overall 302 subjects were randomized to receive one of the treatments, saroglitazar 2mg (n = 101) or saroglitazar 4mg (n = 99), or matching placebo (n = 102). At the end of 12 weeks, subjects treated with saroglitazar 2mg and 4mg tablets had shown significant reduction in mean plasma TG levels by around 46.7% compared to placebo [45].
Moreover, saroglitazar 2mg had shown a significant decrease in levels of non-HDL- cholesterol, very LDL-cholesterol, total cholesterol, and fasting plasma glucose. Additionally, saroglitazar 4 mg also significantly reduced LDL-c and Apo-B levels [44, 45].
After all, as per the data from clinical trials of saroglitazar, serious adverse events (AE) were not reported and all the reported adverse events were mild to moderate in intensity like gastritis, dyspepsia or pyrexia, which were not treatment emergent, and none required any treatment for their resolution [47].
There was no consistent pattern or dose dependency observed in the AEs and no clinically relevant trend or change was observed in clinical laboratory, urinalysis or electrocardiogram (ECG). During the follow up period, major cardiovascular event was not reported and saroglitazar was found safe and well tolerated by patients [46].
After overall analysis of all clinical trials, saroglitazar was found effective for treatment of atherogenic diabetic dyslipidemia having the property of normalizing lipid profile and glycemic parameter [32, 48].
Comparative Long-term Outcome Study of Saroglitazar
In spite of proven therapeutic benefits, large outcome study of saroglitazar showing long term therapeutic efficacy and safety is required. Comparative study about the improvement of Β cell function and insulin sensitivity by study of insulin resistance index (HOMA-IR) can guide about superiority of saroglitazar over other insulin sensitizer drug. Furthermore, clinical trials with the primary aim of atherosclerotic plaque stabilization or plaque regression, pleotropic benefit and data on long term mortality benefits are required before labelling it as one of the safest therapeutic options for treatment of diabetic dyslipidemia [48].
Conclusion
In short, the management of type 2 diabetes mellitus and dyslipidemia is approached with therapeutic lifestyle changes followed by addition of pharmacotherapy with statin with or without fibrate. Furthermore, new therapy has enabled effective yet safe treatment of diabetes dyslipidemia, allowing a potential decrease in risk for cardiovascular disease.
Consequently, one such new drug - saroglitazar, a dual PPAR α/γ agonist has been developed, which can manage both lipid and glycemic parameters. Moreover, saroglitazar is acceptable to patients due to minimal side effects with reduction of pill burden due to dual benefits, but improvement of β cell function and insulin sensitivity by study of insulin resistance index (HOMA-IR) and long term cardiovascular benefits need to be established.
References
- WHO (2014) Cardiovascular Diseases. www.who.int/mediacentre/factsheets/fs317/en/.
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, et al. (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. The Lancet.364 (9438): 937-952.
- Stamler J, Vaccaro O, Neaton J, Wentworth D (1993) Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes care 16 (2): 434-444.
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, et al. (2011) National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet 378 (9785): 31–40.
- Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 3 (11): e442.
- Rose GA, Blackburn H, Gillum RF, Prineas RJ (1982) Cardiovascular survey methods (3rd Edtn). World Health Organization, Geneva. 124–143. whqlibdoc.who.int/publications/2004/9241545763_eng.pdf.
- Joshi SR, Mohan R, Deepa M (2014) Prevalence of Dyslipidemia in Urbanand Rural India: The ICMR–INDIAB Study. PLoS One 9(5): 1-9.
- Morrish NJ, Wang SL, Stevens LK, Fuller JH, Keen H (2001) Mortality and causes of death in the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia 44(2):S14–S21.
- (1999) Diagnosis and classification of diabetes mellitus. World Health Organization,Geneva. whqlibdoc.who.int/hq/1999/who_ncd_ncs_99.2.pdf.
- Roglic G, Unwin N, Bennett PH, Mathers C, Tuomilehto J, et al. (2005) The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care 28(9): 2130–2135.
- (2014) WHO Fact Sheet of Diabetes. www.who.int/diabetes/en.
- Parikh R, Joshi S, Menon P, Shah N (2010) Prevalence and pattern of diabetic dyslipidemia in Indian type 2 diabetic patients. Diabetes & Metabolic Syndrome. Clinical Research & Reviews 4 (1): 10-12.
- (2002) National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation 106 (25): 3143-3421.
- Lewis GF (1997) Fatty acid regulation of very low density lipoprotein production. Curr Opin Lipidol 8:146-53.
- Bruce C, Chouinard RA, Tall AR (1998) Plasma lipid transfer proteins, high-density lipoproteins and reverse cholesterol transport. Annu Rev Nutr 18: 297-330.
- Robinson J (2012) What Is the Role of Advanced Lipoprotein Analysis in Practice?. J Am Coll Cardiol 60(25): 2607-2615.
- Nordestgaard BG, Varbo A (2014) Triglycerides and cardiovascular disease. Lancet 384(9943): 626-35.
- Group T (2010) Effects of combination lipid therapy in type 2 diabetes mellitus. The New England Journal of Medicine 362(17): 1563-67.
- Downs J, Clearfield M, Weis S, Whitney E, Shapiro D, et al. (1998) Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA 279(20):1615-1622.
- (2013) AACE Guideline. www.aace.com/publications/guidelines.
- Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, et al. (2011) ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). European Heart Journal 32: 1769–1818.
- Solano M, Goldberg R (2006) Lipid Management in Type 2 Diabetes. Clinical Diabetes 24(1): 27-32.
- Lalloyer F, Staels B (2010) Fibrates, glitazones, and peroxisome proliferatoractivated receptors. Arterioscler Thromb Vasc Biol 30(5): 894–899.
- Duez H, Lefebvre B, Poulain P, Torra IP, Peruvault F, et al. (2005) Regulation of human apoA-1 by gemfibrozil and fenofibrate through selective peroxisome proliferator-activated receptor alpha modulation. Arterioscler Thromb Vasc Biol 25: 585-91.
- Camp HS, Li O, Wise SC, Hong YH, Frankowski CL, et al. (2000) Differential activation of peroxisome proliferator-activated receptor gamma by troglitazone and rosiglitazone. Diabetes 49: 539-47.
- Lalloyer F, Vandewalle B, Percevault F (2006) PPARa improves pancreatic adaptation to insulin resistance in obese mice and reduces lipotoxicity in human islets. Diabetes 55(6): 1605-13.
- Ravnskjaer K, Boergesen M, Rubi B (2005) Peroxisome proliferator activated receptor-a (PPARa) potentiates, whereas PPARg attenuates, glucosestimulated insulin secretion in pancreatic beta-cells. Endocrinology 146(8):3266-76.
- Staels B, Fruchart JC (2005) Therapeutic roles of peroxisome proliferatoractivated receptor agonists. Diabetes 54(8): 2460-70.
- Lefebvre P, Chinetti G, Fruchart JC, Staels B (2006) Sorting out the roles of PPAR alpha in energy metabolism and vascular homeostasis. J Clin Invest 116: 571-80.
- Lee CH, Olson P, Evans RM (2003) Minireview: lipid metabolism, metabolic diseases, and peroxisome proliferator-activated receptors. Endocrinology 144(6): 2201-7.
- Feige JN, Gelman L, Michalik L (2006) From molecular action to physiological outputs: peroxisome proliferator-activated receptors are nuclear receptors at the crossroads of key cellular functions. Prog Lipid Res 45(2):120-59.
- Conlon D (2006) Goodbye glitazars?. British Journal of Diabetes & Vascular Disease 6(3) 135-137.
- Aggarwal A (2014) Saroglitazar: India's answer to diabetic Dyslipidemia. International Journal of Pharmacology and Clinical Sciences. 3(1): 7-14.
- Bailey CJ (2004) New drugs for the treatment of diabetes mellitus. (3rd edtn) In International Textbook of Diabetes Mellitus, Wiley, Chichester.951-79.
- Henke BR, Blanchard SG, Brackeen MF, Brown KK, Cobb JE, et al. (1998) N-(2-Benzoylphenyl)-L-tyrosine PPARgamma agonists. Discovery of a novel series of potent antihyperglycemic and antihyperlipidemic agents. J Med Chem 41: 5020–36.
- Kendall DM, Rubin CJ, Mohideen P, Ledeine JM, Belderet R, et al. ( 2006) Improvement in glycemic control, triglycerides, and HDL cholesterol levels with muraglitazar, a dual (alpha/gamma) peroxisome proliferator-activated receptor activator, in patients with type 2 diabetes inadequately controlled with metformin monotherapy: A double blind, randomized, pioglitazonecomparative study. Diabetes Care. 29:1016–23.
- Fagerberg B, Edwards S, Halmos T, Lopatynsky J, Schuster H, et al. (2005) Tesaglitazar, a novel dual peroxisome proliferator-activated receptor alpha/gamma agonist, dose-dependently improves the metabolic abnormalities associated with insulin resistance in a non-diabetic population. Diabetologia. 48:1716–25.
- Egerod FL, Nielsen HS, Iversen L, Thorup I, Storgaard T, et al. (2005) Biomarkers for early effects of carcinogenic dual-acting PPAR agonists in rat urinary bladder urothelium in vivo. Biomarkars 10: 295–309.
- Li PP, Shan S, Chen YT, Ning ZQ, Sun SJ, et al. (2006) The PPAR α/γ dual agonist chiglitazar improves insulin resistance and dyslipidemia in MSG obese rats. Br J Pharmacol 148:610-8
- Chen H, Dardik B, Qiu L, Ren X, Caplan SL, et al. (2010) Cevoglitazar, a novel peroxisome proliferator-activated receptor alpha/gamma dual agonist, potently reduces food intake and body weight in obese mice and cynomolgus monkeys. Endocrinology 151:3115-24.
- Younk LM, Uhl L, Davis SN (2011) Pharmacokinetics, efficacy and safety of aleglitazar for the treatment of type 2 diabetes with high cardiovascular risk. Expert Opin Drug Metab Toxicol 6:753-63.
- Yi P, Hadden CE, Annes WF, Jackson DA, Peterson BC, et al. (2007) The disposition and metabolism of naveglitazar, a peroxisome proliferator-activated receptor alpha-gamma dual, gamma-dominant agonist in mice, rats, and monkeys. Drug Metab Dispos 35:51-61.
- Nishihara M, Sudo M, Kamiguchi H, Kawaguchi N, Maeshiba Y, et al. (2012) Metabolic fate of sipoglitazar, a novel oral PPAR agonist with activities for PPAR -γ, -α and -δ, in rats and monkeys and comparison with humans in vitro. Drug Metab Pharmacokinet 27:223-31.
- Jani RH, Kansagra K, Jain MR, Patel H (2013) Pharmacokinetics, Safety, and Tolerability of Saroglitazar (ZYH1), a Predominantly PPARalpha Agonist with Moderate PPARgamma Agonist Activity in Healthy Human Subjects. Clin Drug Investig 33(11): 809-16.
- Jani RH, Pai V, Jha P, Jariwala G, Mukhopadhyay S, et al. (2013) A Multicenter, Prospective, Randomized, Double-Blind Study to Evaluate the Safety and Efficacy of Saroglitazar 2 and 4 mg Compared with Placebo in Type 2 Diabetes Mellitus Patients Having Hypertriglyceridemia Not Controlled with Atorvastatin Therapy (PRESS VI). Diabetes Technol Ther 16 (2): 63- 71.
- Pai V, Paneerselvam A, Mukhopadhyay S, Patel P (2014) A Multicenter, Prospective, Randomized, Double-blind Study to Evaluate the Safety and Efficacy of Saroglitazar 2 and 4 mg Compared to Pioglitazone 45 mg in Diabetic Dyslipidemia (PRESS V). J Diabetes Sci Technol 8 (1): 132-141.
- Joshi S R (2015) Saroglitazar for the treatment of dyslipidemia in diabetic patients; Expert Opinion on Pharmacotherapy 16(4): 597-606.
- Liu ZM, Hu M, Chan P, Tomlinson B (2015) Early investigational drugs targeting PPAR-α for the treatment of metabolic disease. Expert Opin Investig Drugs 24(5): 611-21.





