Patient-Centered Outcomes Research In Advanced Stage Lung Cancer: Study Design and Population
KM Islam1*, MD, PhD; M Copur, MD, FACP2; Addison Tolentino, MD3; Irfan Vaziri, MD4; June Ryan, BS, MPA5; Ann Fetrick, RN,PhD6; Apar Ganti, MD, FACP7,8
1 University of Nebraska Medical Center (UNMC) College of Public Health (COPH), Department of Epidemiology, Omaha, Nebraska
2 Saint Francis Cancer Treatment Center of Grand Island, Nebraska
3 Avera Cancer Institute of Sioux Falls, South Dakota
4 Callahan Cancer Center of North Platte, Nebraska
5 Nebraska Cancer Coalition
6 UNMC, COPH, Department of Health Services Research, Administration, and Policy
7 Veterans Healthcare Administration, Nebraska-Western Iowa Health Care System
8UNMC, Division of Oncology and Hematology, Omaha, Nebraska.
*Corresponding Author
KM Islam,
984395 Nebraska Medical Center,
Omaha, NE, USA.
Tel: +1 402 559 8283; Fax: +1 402 559 7259
E-mail: kmislam@unmc.edu
Article Type: Research Article
Received: March 07, 2014; Accepted: April 12, 2014; Published: April 14, 2014
Citation: KM Islam et al (2014) Patient-Centered Outcomes Research In Advanced Stage Lung Cancer: Study Design and Population. Int J Cancer Stud Res. 3(1), 31-35. doi: dx.doi.org/10.19070/2167-9118-140005.
Copyright: KM Islam© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background:
In 2013, researchers at the University of Nebraska Medical Center (UNMC) received funding from the Patient-Centered Outcomes Research Institute to establish a study that outlines treatment options for patients who have stage IV lung cancer. With collaborators at 4 cancer centers, UNMC researchers will compare treatment preferences among these patients when available drugs offer the same survival but different side effects. Patient preferences identified in this study can be used to inform clinical practice. This paper describes proposed study methods and population for this patient-centered outcomes research (PCOR) and highlights their significance for PCOR in lung cancer. Lung cancer is the leading cause of cancer-related deaths in the United States. Treating physicians have traditionally measured treatment success for stage IV non-small cell lung cancer (NSCLC) in terms of survival. It is not known whether individual patients also see success in terms of survival. There is no evidence to suggest that patient preferences regarding adverse treatment effects are systematically considered when choosing a treatment regimen for stage IV NSCLC. Not much is known about patient perspectives on the trade-offs between possible additional survival and possible side effects related to a treatment regimen.
Study design:
We will conduct a multicenter mixed method study design, which includes focus groups, and cross-sectional, prospective, and randomized experimental designs, to answer PCOR questions.
Study population: Baseline data from participating cancer centers were obtained to determine sample size. On the basis of this data, we expect a study population of lung cancer patients that is 48% female and 52% male, with average age about 70 years. We also expect the population to be about 50% rural and 50% urban.
Conclusion:
A complex design may be necessary for a PCOR study to reflect patients’ preferences. Analysis of existing data from participating cancer centers is essential to understand the characteristics of the lung cancer patient pool for study and to estimate an accurate study sample.
2.Introduction
3.Background
4.Study Design
5.Study Population
6.Discussion
7.Conflict of Interest and Sources of Funding
8.Acknowledgments
9.References
Keywords
Patient-Centered; Outcomes; Lung Cancer; Study Design; & Population.
Introduction
In 2013, researchers at the University of Nebraska Medical Center (UNMC) received funding from the Patient-Centered Outcomes Research Institute to establish a protocol that outlines treatment options for patients who have stage IV lung cancer. With collaborators at 3 other cancer centers, UNMC researchers will compare treatment preferences among different patient groups when available drugs offer the same survival but different side effects. Patient preferences identified in this study can be used to inform clinical practice. This paper describes study methods and population selection for this patient-centered outcomes research (PCOR) on stage IV lung cancer patients and the possible significance of this research for other disease states.
PCOR provides information about the best available evidence to help patients and their health care providers make more informed decisions. This research is intended to give patients a better understanding of the prevention, treatment, and care options available and the science that supports those options, and to encourage physicians and other clinicians to adopt a more patient-centered approach to treatment [1].
PCOR projects require patient voices to be heard in discussions with their physicians in determining the value of treatment options. The goal of a PCOR study is to give patients and their family members the information they need to answer patient-focused questions such as “Given my personal characteristics, conditions, and preferences, what should I expect will happen to me?” or “What are my options and what are the benefits and harms of those options?”
Conducting a rigorous PCOR study is challenging. In this type of research, the trade-offs between practical issues and internally valid designs must be weighed. These trade-offs can be resolved by questioning the validity of the study design or the accuracy of inferences drawn. There is no simple formula for determining external validity. Researchers must make judgments regarding whether the findings would be applicable in other populations. These judgments can always be challenged, and researchers may have to defend the study’s validity. Concern about the external validity of the results of PCOR studies is warranted, because such studies focus on a very specific patient population’s preferences and choices. The research raises the question, “can the results of a PCOR be applied across different populations, in different settings, and in other periods of time?” We propose that the outcomes of our study will be translatable to disease conditions other than late stage lung cancer and will provide support for this proposition later in this paper.
In the United States, lung cancer is the leading cause of cancerrelated deaths [2]. In Nebraska, from 2006 to 2010, half (50%) of lung cancer patients were diagnosed at an advanced stage of disease. During this same period, 5,979 Nebraskans were diagnosed with lung cancer, and 4,537 died from it [3]. Nationally, about 228,190 new cases of lung cancer and 159,480 deaths were expected in 2013. Lung cancer is a major source of health care costs [4, 5]. Stage of disease at diagnosis strongly affects the prognosis for cancer patients. The most recent national data show that the 5-year survival rate for lung cancers diagnosed at a local stage is 53.5%, compared to only 3.9% for distant stage cases. Over 50% of stage IV lung cancer patients die within one year of diagnosis [6].
We selected lung cancer for our PCOR focus because of the number of persons who experience this form of cancer and because so many (50%) are diagnosed at late stage, e.g., stage III or IV. Further, we decided to limit our study to patients diagnosed with non-small cell lung cancer (NSCLC) for two reasons. First, small cell lung cancer is often diagnosed only days prior to death, when no treatment options are available, and second, NSCLC lung cancer is typically treated with a small number of chemotherapy regimens with outcomes that have not been well studied.
Treatment success for stage IV NSCLC has traditionally been measured in terms of survival. However, it is not known whether individual patients also see success in terms of survival. Not much is known about patient perspectives on the trade-offs between possible additional survival and possible side effects related to a treatment regimen.
Traditional treatment goals are to prolong survival and control disease-related symptoms. There are a limited number of commonly used chemotherapy combinations for the treatment of stage IV NSCLC. These drug regimens lead to a similar improvement in survival, but have different toxicity profiles [7]. Thus, toxicity profiles are important determinants of treatment choices and treatment success [8].
As with many other medical conditions, patients’ preferences regarding adverse effects of treatment are not systematically considered when choosing a treatment for stage IV NSCLC. In assessing patient preference, we expect to look at such factors as patient perceptions about how much time patients have left to live, major changes in life style, impact of the cancer on family and friends, functional status, pain, nausea, and other known adverse effects of chemotherapy. There is no clinical guide for patients or physicians on how to integrate patient preferences regarding adverse effects into treatment decisions, although it is well known that most cancer patients prefer an active or a shared role in decision making [9, 10]. Our study will investigate whether oncologists, when given patient-specific information, will incorporate that information into treatment planning, or, ideally, will ask individual patients their preference regarding adverse effects of chemotherapy prior to developing a treatment plan.
We proposed a PCOR study among patients with stage IV NSCLC to answer these questions:
(1) In cases of advanced lung cancer, how do patients define treatment success?
(2) Among possible side effects of treatments with about equal prognosis/outcomes, which side effects would patients most like to avoid?
(3) Is a single summary score obtained from a list of patient’s preferred adverse events to predict a reallife scenario?
(4) Will oncologists take patient preferences into account when selecting chemotherapy treatment?
The purpose of this paper is to describe the study methods and population of this PCOR study and to highlight their significance for patientcentered outcomes research in lung cancer, and for other diseases.
For this study of lung cancer patients and their caregivers, we selected a multicenter mixed method design, which includes focus groups, and cross-sectional, prospective, and randomized experimental designs to answering the research questions. The multicenter, mixed method design will allow us to capture the necessary data for all three specific aims and will allow for rapid patient recruitment. All participants will be consecutively recruited from four cancer treatment centers across Eastern and Central Nebraska and Southern South Dakota.
Data for this clinic-based study will be collected directly, offering several advantages over indirect data collection. We expect overall higher patient participation with face-to-face data collection, particularly given that stage IV lung cancer patients are typically age 70 years and older. In addition, nurse coordinators will be able to immediately review patients’ responses, while patients are still in the clinic, and obtain missing questionnaire items if necessary. Furthermore, this clinic-based study allows for objective measurement of clinical variables, such as actual treatment received and medical adverse effects experienced. These objective measurements would not be feasible in population-based, phone-based, or mail-in designs. With this design, we can also assess changes in treatment choices when physicians are provided with patientcentered adverse effects (PCAE) preferences.
Although focus groups will not examine any specific research questions, they play a very important role in this study. Engaging patients, their caregivers, and patients’ advocates at early stages of the study can improve study design, execution, and translation, and patient satisfaction [9]. We plan to conduct four focus groups at two different locations. At each location, we will conduct one focus group with patients and their family members and patient advocates, and one focus group with cancer center clinicians. Each group will include a maximum of 10 participants to promote participation by all. A trained focus group facilitator will conduct the focus groups; two non-participating note takers and two tape recorders will capture participants’ comments. Each focus group will last about 90 minutes, and lunch or snacks and beverages will be provided to the participants. Focus group recordings and notes will be transcribed by two different people and then compared for accuracy and consistency. The PI and a student will determine thematic content of the focus groups. To make this study more patient-centered, focus group participants will review and comment on all data collection forms to refine the length and time required to complete the data collection tools. We will seek input from patients and their caregivers on socio-demographic questions, particularly their preferences regarding answering personal or sensitive questions, especially those related to family income. More importantly, we will seek suggestions from focus group participants on which non-medical adverse effects, such as hair loss, brittle nails, increased pain, etc., should be included in this study. During focus groups, we will also seek patients’ and caregivers’ input on recruitment of study participants, dissemination of the study findings, and ways to keep patients engaged throughout the study. We believe that patients can play an active and engaged role in research, becoming partners rather than participants. Our study methodology is collaboratively developed and patient-centered, an important consideration for patients and caregivers both in this lung cancer study and in other cancer studies.
To evaluate the first research question, we will utilize a crosssectional study in which we will simultaneously analyze information on the outcome variable (patient-centered definition of treatment “success”) and its relationship to patient characteristics.
We will deploy a prospective cohort study for the examination of the second research question because we will analyze changes in PCAE preferences over time, comparing multiple exposures (patient characteristics, real-life adverse effects experienced during chemotherapy, and drugs received for treatment). For the third research question, we will compare summary scores from a list of adverse effects to a real-life drug choice. Both summary score and real-life drug choice information will be collected at the same point in time using a cross-sectional study design. For the fourth research question, we will determine whether a physician’s knowledge of a patient’s preferred PCAE affects the physician’s treatment decisions. To answer this question, we will utilize a two-arm, physician-blinded, randomized, controlled design.
Limited data are available on stage IV NSCLC patients in Nebraska and South Dakota. We collected cross-sectional data from four participating cancer centers’ annual reports to justify our ability to enroll the required sample size and understand the basic demographics of the study population. These background data clearly demonstrated the potential pool of patients for recruitment and described the representativeness of a sample.
Using prior year data, we estimated that 384 new patients would be seen at the four sites over a period of two years. We calculated study power based on the expected final sample size available to test our hypotheses at specific time points of interest, after accounting for refusals, loss to follow-up, withdrawals, or other reasons for not completing the study. Table1 demonstrates the representativeness of the lung cancer patients from the participating cancer centers to the states’ total number of lung cancer patients for both Nebraska and South Dakota [12, 13, 14].
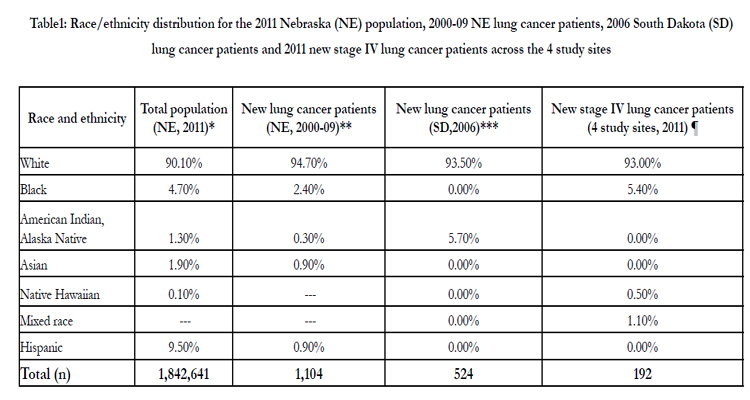

Table1: Race/ethnicity distribution for the 2011 Nebraska (NE) population, 2000-09 NE lung cancer patients, 2006 South Dakota (SD) lung cancer patients and 2011 new stage IV lung cancer patients across the 4 study sites.
*Source: US Census Bureau (http://quickfacts. census.gov/qfd/states/31000.html)[10].
** Source: Nebraska HHS13 Data for 2010-11 to be released [11].
***Source: South Dakota Health Department. More recent data have not been released [12].
¶Source: study sites in Nebraska (UNMC, Callahan, St. Francis) and South Dakota (Avera)
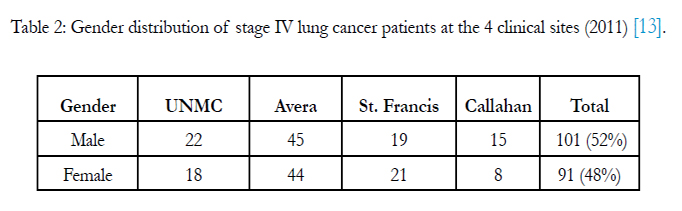
Table 2: Gender distribution of stage IV lung cancer patients at the 4 clinical sites (2011) [13].
The average age of lung cancer patients seen by the participating clinics was about 70 years. The average patient age at the cancer centers is similar to the national and state (Nebraska and South Dakota) averages (Figure1). Race and ethnicity of treated patients in the four cancer centers mirrored that of total populations for both Nebraska and South Dakota (Table1). About 50% of diagnosed lung cancer patients reported rural residence, again reflecting the demographics of the two states. Based on preliminary data, we expect that about 48% of our patient population will be female and 52% male, which is consistent with national and state percentages of lung cancer patients (Table 2) [15].
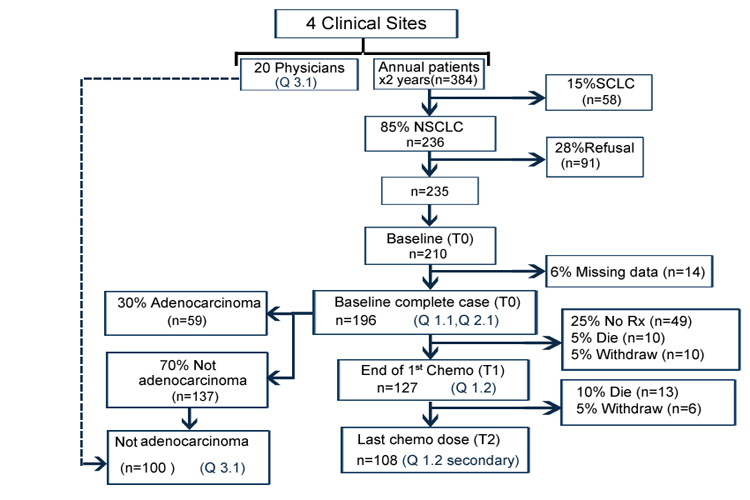
Figure 1: Study participants and visits, which is based on the preliminary data from the participating cancer centers.
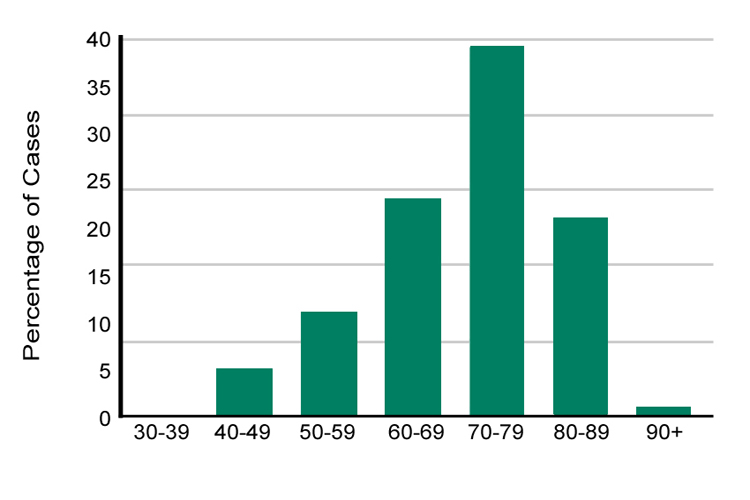
Figure 2: Age at diagnosis of lung cancer patients, Avera Cancer Institute site, 2001-2008 [Avera Cancer Institute, 2009]
Existing data from the participating cancer centers showed the representativeness of the population demographics of the lung cancer patients in Nebraska and South Dakota. Our study sample represents age, gender, and race distribution similar to that of the states’ total stage IV lung cancer patients.
Although we expect higher participation and lower study procedure-related attrition than is commonly seen in more invasive protocols, there will be a potential for missing and lost-to-follow-up data in our study over a three-year period. Based on the four cancer centers’ experiences with past clinical research, we do not anticipate more than 5% missing data at baseline and no more than a 28% refusal rate (These factors are critical in sample size calculations.) Generalizability of the study findings is another important aspect of the clinical research. To maximize generalizability, we have carefully limited the exclusion criteria for this study. Patients who will not undergo chemotherapy will be excluded because our study research questions require that patients experience real-life treatment and treatment-related adverse effects. We excluded adenocarcinoma patients because almost all of these patients are treated with only one drug regimen (pemetrexed combination) due to its substantially lower toxicity profile and slightly higher efficacy compared to other options. Review of the historical data from the participating cancer centers informed us about the available lung cancer patient pool for study participation, estimating accurate samples, calculating statistical power, and providing confidence on the generalizability of the study findings. Moreover, data showed that we will have enough power for subgroup analysis on gender, age, race, and residence status (rural/urban).
Choosing an appropriate design and relevant sample population for any epidemiological study is important for both internal and external validity. The study design allows us to translate the research questions into operational questions. Adapting an inappropriate study design can raise a question of internal validity; on the other hand, selecting inappropriate study participants can impact external validity. The study design that we selected could readily be applied to studying other cancers and chronic diseases in general. The uniqueness of our stage IV lung cancer study is that there are a limited number of chemotherapeutic treatments that have demonstrated differences in side effects. We did not investigate in any detail the treatment options for other cancers or chronic diseases such as diabetes or heart disease; however, the literature and our own experience suggest that patients would prefer being asked about their treatment preferences for many medical conditions. We anticipate that our study outcomes will provide useful information about patient-centered treatment for lung cancer and for other diagnoses.
Conflict of Interest and Sources of Funding
This project was supported in part by the Patient-Centered Outcomes Research Institute (PCORI) Contract #CE-12-11-4351.The contents are solely the responsibility of the authors and donot necessarily represent the official views of PCORI.
We acknowledge Lorena Baccaglini, PhD; UNMC COPH, Department of Epidemiology, and Jim Anderson, PhD; UNMC COPH Department of Biostatistics, for their contributions.
References
- www.pcori.org/about-us/landing/
- American Cancer Society. Cancer Facts & Figures 2013. 2013.
- dhhs.ne.gov/publichealth/Pages/ced_cancer_data.aspx
- American Cancer Society. Cancer Facts and Figures 2012. 2012.
- Goodwin, PJ., Shepherd, FA. Economic issues in lung cancer: a review. J Clin Oncol. 1998; 16(12): 3900-12.
- Kutikova, L., Bowman, L., Chang, S., Long, SR., Obasaju, C., & Crown, WH. The economic burden of lung cancer and the associated costs of treatment failure in the United States. Lung Cancer. 2005; 50(2): 143-54.
- National Cancer Institute. SEER Data, 1973-2008. 2010 [cited; Available from: seer.cancer.gov/data/
- National Cancer Institute. Non-Small Cell Lung Cancer Treatment. 2012 [cited; Available from: www.cancer.gov/cancertopics/pdq/treatment/non-small-cell-lung/healthprofessional/page11
- Shekelle, P., & Mahar, A. Treatment of Metastatic Non-Small Cell Lung Cancer: A Systematic Review of Comparative Effectiveness and Cost Effectiveness.Department of Veterans Affairs. Health Service Research & Development Service. Washington, DC. 2012.
- Bruera, E., Willey, JS., Palmer, JL., & Rosales, M. Treatment decisions for breast carcinoma: patient preferences and physician perceptions. Cancer.2002; 94(7): 2076-80.
- Stacey, D., Paquet, L., & Samant, R. Exploring cancer treatment decisionmaking by patients: a descriptive study. Curr Oncol. 2010; 17(4): 85-93.
- US Census Bureau (quickfacts.census.gov/qfd/states/31000.html)
- Nebraska HHS Cancer Report. 2009 [cited; Available from: dhhs.ne.gov/publichealth/Pages/ced_cancer_data.aspx
- South Dakota Department of Health 2009 [cited; Available from: getscreened.sd.gov/documents/Lung2009.pdf
- Avera Cancer Institute. Annual report, 2008-2009. 2009 [cited; Available from: www.avera.org/pdf/queen-of-peace/cancer-center-annualreport-09_v2.pdf





