Intra-stent Coronary Perforation: a Race against Time
Piraino D1,Dendramis G2*, Buccheri D1, Paleologo C2, Teresi G2, Rotolo A2, Andolina G1, Assennato P2
1 Division of Cardiology, Department of Internal Medicine and Cardiovascular Diseases, Section of Interventional cardiology and hemodynamics, University Hospital “Paolo Giaccone”, Palermo, Italy.
2 Division of Cardiology, Department of Internal Medicine and Cardiovascular Diseases, Section of Intensive Coronary Care Unit, University Hospital “Paolo Giaccone”, Palermo, Italy.
*Corresponding Author
Gregory Dendramis, M.D,
U.O.C. di Cardiologia II con Emodinamica,
Via Del Vespro, 127, CAP 90127. Palermo, Italy.
Tel: 0916554303
Fax: 0916554304
E-mail: gregorydendramis@libero.it
Received: March 18, 2015; Accepted: April 02, 2015; Published: April 07, 2015
Citation: Dendramis G, et al., (2015) Intra-stent Coronary Perforation: a Race against Time. Int J Clin Ther Diagn. 3(2) 77-80. doi: dx.doi.org/10.19070/2332-2926-1500015
Copyright: Dendramis G© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Coronaric perforation, while representing fortunately a rare complication (incidence among 0.2–0.6 %), it is burdened by a high mortality rate if not properly and promptly treated. We report the case of an intra-stent coronary perforation at the end of revascularization of a non ST elevation myocardial infarction (NSTEMI), followed by immediate impairment of hemodynamic compensation due to significant pericardial effusion and subsequent cardiac tamponade.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Coronary Perforation; Covered Stent; Percutaneous Coronary Intervention; Myocardial Infarction; Intra Aortic Balloon Pump.
Introduction
Despite the different methods of coronaric revascularization, percutaneous coronary intervention (PCI) is gold standard as treatment for coronary lesions. The possible complications, however, deserve proper attention and treatment modality. Coronaric perforation, while representing fortunately a rare complication (incidence among 0.2–0.6 %), it is burdened by a high mortality rate if not properly and promptly treated [1, 2].
We report the case of an intra-stent coronary perforation at the end of revascularization of a non ST elevation myocardial infarction (NSTEMI), followed by immediate impairment of hemodynamic compensation due to significant pericardial effusion and subsequent cardiac tamponade.
Case Report
A 67 years old man, hypertensive and former smoker reports previous lateral NSTEMI in 2008 for which coronary angiography was performed with evidence of critical stenosis (70%-90%) of the distal left anterior descending (LAD) coronary dilated middle segment with a sequence of moderate stenosis, occlusion of the distal left circumflex artery (LCX) rehabilitated by collateral homocoronaric circulation, moderate stenosis of the right coronary artery (RCA).
After an ineffective attempt of distal LCX revascularization, the patient was discharged after medical therapy optimization.
Myocardial scintigraphy performed in January 2013 evidenced moderate/severe inducible ischemia with low workload involving the inferolateral myocardial wall. In November 2013, due to the appearance of localized pain in the left shoulder, noticing a NSTEMI ( ST depression in the anterior side extended max 3 mm in V3-5, ST elevation max 1 mm in aVr) (Figure.1), he was transferred to our cardiology care unit (CCU).
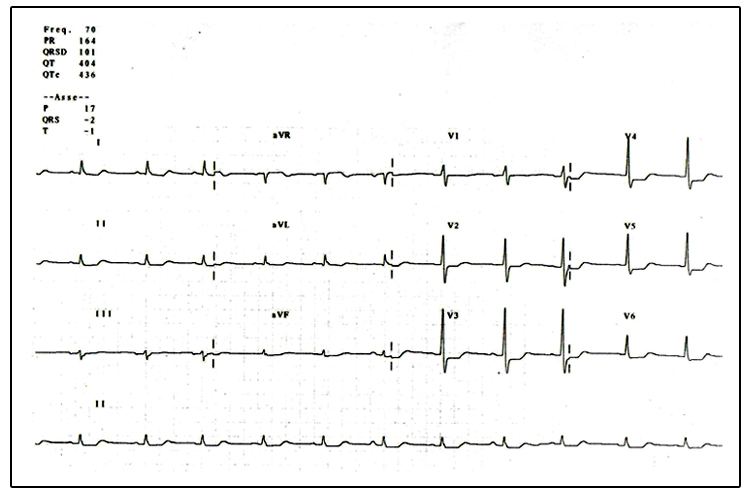
Figure 1
The patient had increased myocardial necrosis index (cTnI 0.035 ng/ml), eGFR (MDRD) 65.4 ml/min/1.73 mq, Killip class 1 and high GRACE risk score (153).
We gave him ASA 300 mg orally and enoxaparin 6000 IU sc. Urgent coronary angiography performed demonstrated extremely calcified coronary vessels, critical stenosis of middle LAD with occluded apical segment rehabilitated by collateral homocoronaric circulation. Distal LCX and obtuse marginal (OMB) were occluded and rehabilitated by homocoronaric collateral circulation (Figure. 2,3,4), RCA with critical stenosis along its course (Figure. 5).
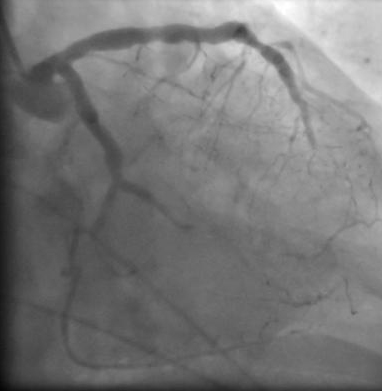
Figure 2

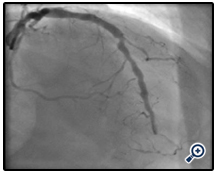
Figure 3
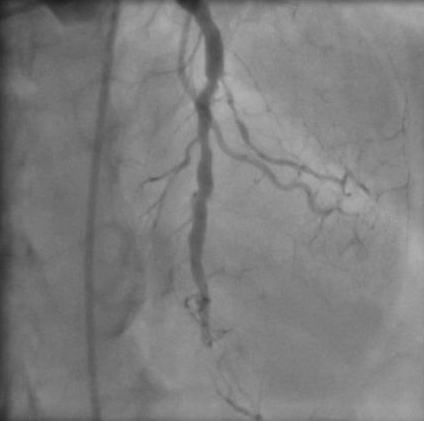

Figure 4
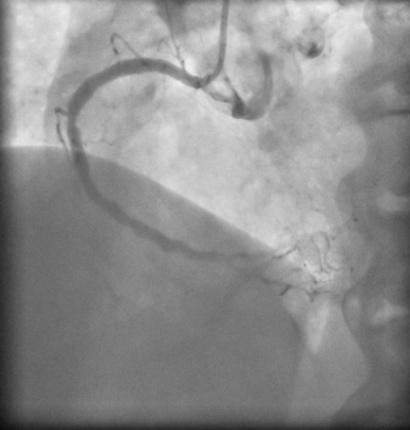
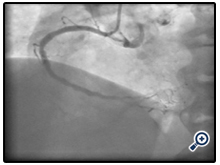
Figure 5
So we decided to give the patient prasugrel 60 mg orally and perform PCI on middle LAD, beyond the critic and extremely calcific stenosis with the guide wire BMW ABBOTT (a second ABBOTT BMW guide wire placed on diagonal branch) with implantation of a bare metal stent (BMS) MULTI -LINK ABBOTT 5 x 18 mm (issued to 16 atm, diameter reached 5.33 mm) (Figure. 6).
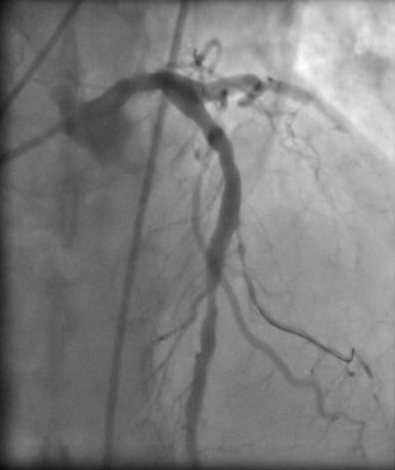
Figure 6
At the end of the implantation of the first BMS an accentuation of the critical limit stenosis with aspect to minus was observed down the edge of the stent, so we proceeded to implantation of a overlapping BMS MULTI-LINK ABBOTT 4.5 x18 mm (issued to 14atm, diameter reached 4.8mm) and post expended the point of overlapping with the balloon of the second stent. Angiography performed after implantation of these two overlapping BMS showed the presence of intra-stent coronaric perforation type III [1] with hemorrhage (Figure. 7,8) and progressive and rapid reduction in blood pressure and bradycardia.

Figure 7
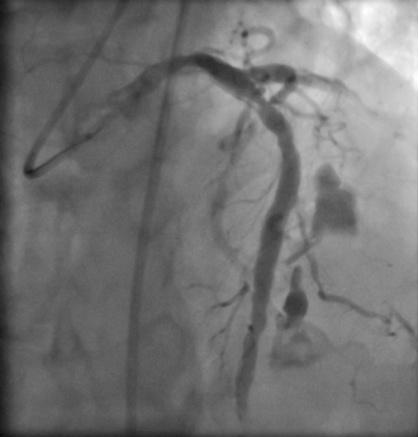
Figure 8
After placement of intra aortic balloon pump (IABP), a covered stent GRAFTMASTER (Jostent Graftmaster, Abbott Vascular) 3.5 x 16 mm (inflated up to cover the perforation) was placed (Figure. 9,10) but the angiographic acquisitions in the course of the placement of the covered stent and at the end of the placement revealed mutiple perforations (difficult to assess precisely because of severe hypotension, systolic blood pressure 60 mmHg) with slow-flow in the middle-distal LAD.
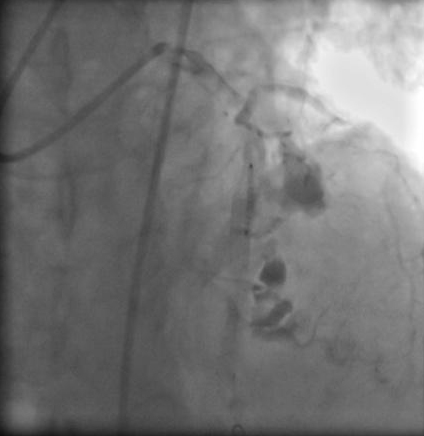
Figure 9
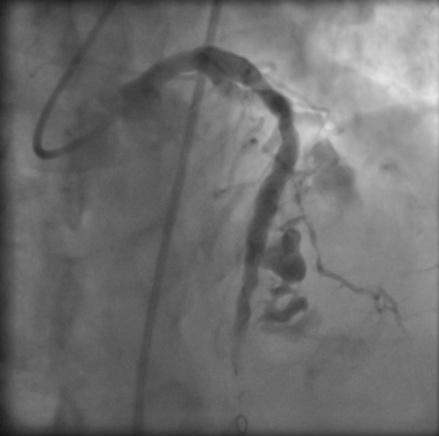
Figure 10
We proceeded to the positioning of a overlapping covered stent GRAFTMASTER 3.5 x 19 mm (Figure. 11). Subsequent angiogram showed adequate control of the perforated segments of LAD (Figure. 12).
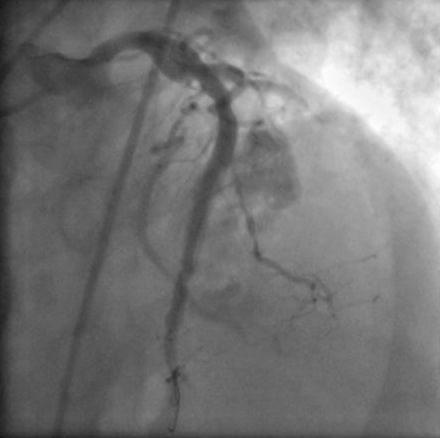
Figure 11

Figure 12
Meanwhile because of cardiac tamponade confirmed by echocardiography (38 mm pericardial effusion with collapse of the right cavities) pericardiocentesis was performed (subxiphoid approach) with aspiration of 350 ml of blood and rapid improvement in hemodynamic balance (normalization of pressure and cardiac frequency).
We removed the IABP when the patient stabilized and maintained pericardial drainage removed after 24 hours.
The seriated ECG performed until discharge showed resolution of ST-segment depression, with a normalization of myocardial necrosis index (Figure. 13). Echocardiography monitoring postpericardiocentesis showed normal-sized and contractility of left ventricle, ejection fraction 50%, no residual pericardial effusion. At day five post-procedural, the patient was discharged in dual antiplatelet (prasugrel and ASA) and at follow-up performed after one month he has adequate clinical conditions.
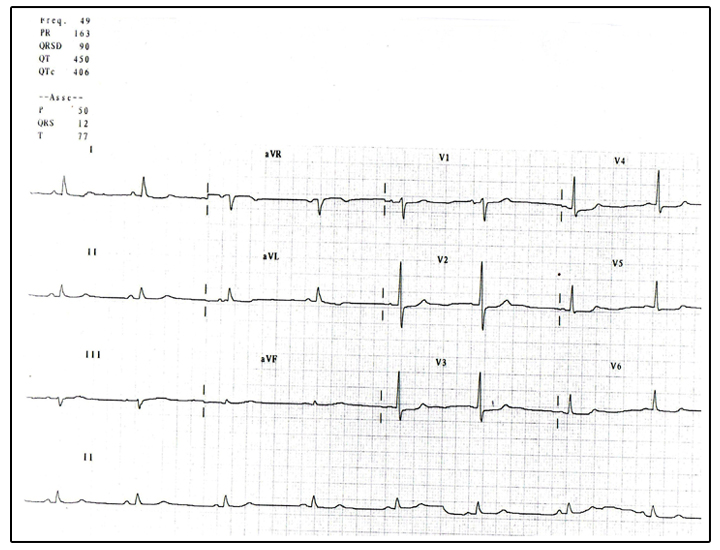
Figure 13
Discussion
According to the Ellis classification, the coronary artery perforation described in our case report appears to be of type III [1].
The coronary perforation is potentially lethal although a rare complication [3]. The sudden accumulation of blood in the pericardial space may lead to cardiac tamponade with resulting cardiogenic shock and high mortality rate. Closure of the perforated segment must therefore be immediate to limit the chain of events that could be fatal for the patient [4].
Several devices have been introduced to repair the coronary perforations, the one we used is the GraftMaster stent [5,6].
Although in the type III perforation with hemodynamic compromise the CABG emergency intervention might be indicated [7] the time needed to prepare the operating room might be too long. The stent graftmaster placement in our case, has allowed us to keep the patient alive by rapid correction of the hemorrhage. So the immediately pericardiocentesis, done in later time, has allowed to remove the cause of cardiac deficit, solving the cardiac tamponade with immediate recovery suggest by efficient ventricular contractility and correct hemodynamic compensation. The IABP placement was possible despite to presence of abdominal aorta aneurysm (AAA) under the kidney.
So, although CABG is an excellent treatment in type III Ellis perforation, the use of covered stents represented an alternative quicker treatment. Experience about the use of covered stents may provide an option to save valuable time for this serious complication [8], therefore, as reported by Gunning and others in a retrospective study CABG could be used as an alternative treatment when coated stent and the pericardial drainage had not corrected the initial hemodynamic compromise [3].
In regard to long-term complications, especially in type III coronaric perforation showed a high incidence rate. Rasha and others reported from a retrospective study of 24.465 patients 56 patients had type III coronary perforation, with a mortality rate of 3.6% [9].
Therefore our case report offers different points of reflection : faced with an acute and life-threatening as the type III Ellis coronary perforation, what to do?
Listed therapeutic options are : prolonged balloon inflation , coated stent implantation , CABG surgical repair and embolization [10, 11], but there are various points to consider.
Meanwhile, the type of injury that you have to face : although appropriate management would appear to include the immediate placement of a perfusion balloon (if longer available, balloon should be placed rapidly ) to minimize ischemia and because some perforations can be " sealed" [1], a highly calcified coronary segment often does not allow to recross the lesion and the perforated segment of the stent with the balloon (used and frayed) to make a prolonged balloon inflating, so we had to discard this hypothesis and place a covered stent (it was easy by the high caliber of the LAD).
We dropped the surgical option because of severe hemodynamic instability of the patient and there was not enough time (even if, due to the low pressure it was difficult an adequate visualization of the involved segment to understand if the extravasation blood had stopped after covered overlapping implantation stent).
Finally resolved perforation, pericardiocentesis has restored thehemodynamic stability and ventricular contractility.
According to the literature regarding the type III Ellis perforations , we have not stopped dual antiplatelet therapy once the perforation was resolved [1].
Conclusion
We have described the case of a coronary stenosis perforation in a subject with acute coronary syndrome; potentially a fatal complication which in our case was successfully treated with the use of two covered stents without having to resort to surgery by CABG.
The use of covered stents have meant that the CABG emergency requirements decreased [12].
References
- Ellis SG, Ajluni S, Arnold AZ, Popma JJ, Bittl JA, et al. (1994) Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation 90:2725-2730.
- Gunning MG, Williams IL, Jewitt DE, Shah AM, Wainwright RJ, et al. (2002) Coronary artery perforation during percutaneous intervention: incidence and outcome. Heart 88:495-498.
- Klein LW. (2006) Coronary artery perforation during interventional procedures. Catheter Cardiovasc Interv 68:713-717.
- Liu F, Erbel R, Haude M, Ge J. (2000) Coronary arterial perforation: prediction, diagnosis, management, and prevention. In: Ellis SG, Holmes DR Jr, eds. Strategic Approaches in Coronary Intervention, 2nd ed. Philadelphia: Lippincott Williams and Wilkins 501-514.
- Ramsdale DR, Mushahwar SS, Morris JL. (1998) Repair of coronary artery perforation after rotastenting by implantation of the Jostent covered stent. Cath Cardiovasc Diagn 45:310-313.
- Lansky AJ, Yang YM, Khan y, Costa RA, Pietras C, et al. (2006) Treatment of coronary artery perforations complicating percutaneous coronary intervention with a poly tetrafluoroethylene-covered stent graft. Am J Cardiol 98:370-374.
- Kihara S. I, Shimakura T, Tanaka S. A, Saito N, Sugawara Y (2000) Surgical angioplasty of ruptured left anterior descending coronary artery without cardiopulmonary bypass. The Japanese Journal of Thoracic and Cardiovascular Surgery 48(5):326-328.
- Gercken U, Lansky AJ, Buellesfeld L, Desai K, Badereldin M, Mueller, et al. (2002) Results of the Jostent coronary stent graft implantation in various clinical settings: procedural and follow-up results. Catheter Cardiovasc Interv 56:353-360
- Al-Lamee R, Ielasi A, Latib A, Godino C, Ferraro M, et al. (2011). Incidence, predictors, management, immediate and long-term outcomes following grade III coronary perforation. JACC: Cardiovascular Interventions 4(1):87-95.
- Chua SK, Lee SH, Shyu KG, Hung HF, Lin SC, et al. (2008) Incidence , Management, and Clinical Procedures Outcomesof -Related Coronary ArteryPerforation : 13.888 Analysis of Coronary Angioplasty Procedures. Acta Cardiol Sin 24:80 _5.
- Aslam MS, Messersmith RN, Gilbert J, Lakier JB (2000) Successful management of coronary artery perforation with helical platinum microcoil embolization. Catheter Cardiovasc Interv 51:320-322.
- Yeo K, Rogers J, Laird J (2008) Use of stent grafts and coils in vessel rupture and perforation. J Interven Cardiol 21:86-99





