A Multidisciplinary Approach to the Functional and Esthetic Rehabilitation of a Patient with Bulimia Nervosa: A Clinical Report
Pantzari F1*, Kamposiora P2, Papavasiliou G2
1 Former Resident, Department of Prosthodontics, Dental School, University of Athens, National and Kapodistrian University of Athens, Greece.
2 Assistant Professor, Department of Prosthodontics, Dental School, University of Athens, National and Kapodistrian University of Athens, Greece.
*Corresponding Author
Dr. Foteini Pantzari DDS,
Former Resident,
Department of Prosthodontics, Dental School,
University of Athens,
National and Kapodistrian University of Athens,
53 Agias Fotinis Street, 17121, Nea Smyrni, Athens, Greece.
E-mail: fotinipantzari@hotmail.com
Article Type: Case Report
Received: January 23, 2015; Accepted: March 12, 2015; Published: March 13, 2015
Citation: Pantzari F, Kamposiora P, Papavasiliou G (2015) A Multidisciplinary Approach to the Functional and Esthetic Rehabilitation of a Patient with Bulimia Nervosa: A Clinical Report. Int J Dentistry Oral Sci. 2(3) 53-58. doi: dx.doi.org/10.19070/2377-8075-1500012
Copyright: Pantzari F© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium,provided the original author and source are credited.
Abstract
Treatment of a patient with bulimia nervosa is a challenge for the dental clinician. The oral manifestations of bulimic behavior, which include sore and inflamed throat, swollen salivary glands, tooth wear and decay, require a multidisciplinary approach. This clinical report illustrates the treatment of a 22-year-old female patient with history of bulimia nervosa and dentition with extended signs of erosion. It included thorough diagnosis with the use of screening tool BITE (Bulimic Investigatory Test, Edinburgh) and initial evaluation of tooth wear with the TWI (Tooth Wear Index). Crown lengthening and prosthetic rehabilitation with all- ceramic restorations on anterior teeth and metal- ceramic single crowns on posterior teeth was the treatment of choice.
2.Introduction
3.Clinical Report
4.Discussion
5.References
Keywords
Bulimia Nervosa; Tooth Erosion; BITE Screening Tool; TWI (Tooth Wear Index).
Introduction
Anorexia and bulimia nervosa in the psychiatric literature are interconnected by the term “eating disorders’. Both affect the regulation of food intake. Anorexia nervosa is defined as an aversion to food due to psychological causes, leading to severe loss of weight [1]. Bulimia nervosa is defined as ‘Perpetual and voracious appetite for food in large quantities, as a result of increased hunger to a morbid degree’ [1]. The patient affected by bulimia nervosa consumes large amounts of food and feels a lack of control over this behavior. This binge – eating is followed by habits like forced vomiting, use of laxatives or diuretics, fasting, extreme exercise routines or a combination of these behaviors in order to compensate for overeating [2].
The profile of a bulimic patient can include:
- sore and inflamed throat,
- swollen salivary glands in the neck and jaw area,
- worn, sensitive and decaying teeth after being exposed to stomach acid,
- acid reflux disorder and other gastrointestinal problems
- intestinal irritation from laxative abuse
- severe dehydration from purging of fluids and
- electrolyte imbalance (too low or too high levels of sodium, calcium, potassium and other minerals) which can even lead to heart attack [3].
The Bulimic Investigatory Test, Edinburgh [4] (BITE) is used for the assessment of bulimic behaviors in a given population. BITE is a 33-item self- report measure, designed to identify the severity of symptoms and bulimic behaviors. High scores in Symptoms Scale give a high probability of meeting the criteria of bulimia nervosa, whereas high scores in Severity Scale should lead to further investigation. BITE as a test presents with high validity and internal consistency [5].
The majority of manifestations of bulimia nervosa being apparent in the head, neck and oral cavity qualify the dentist to identify the problem and guide the patient through coordinated care [6]. The clinician detecting the signs of eating disorders needs to refer the patient to a mental health specialist and a nutritionist [7]. Considering tooth wear, the dentist’s role is preventive, as well as educational.
Due to regurgitation and common vomiting, the bulimic patients present with erosion and destruction of hard tissues, mainly on the palatal surfaces of upper teeth and the occlusal surfaces of the lower. The appearance of smooth silky-glazed, sometimes dull, enamel surface with the absence of perikymata and intact enamel along the gingival margin are typical signs of erosion [8]. This initial stage as erosion progresses leads to rounding of tooth cusps and restorations rising above the level of the adjacent teeth. The ‘cupping’ and ‘cratering’ from erosion cannot be matched to surfaces of the opposing teeth. The tooth wear index (TWI) [9, 10] is widely used in order to record changes to the anatomical structure of the teeth, independently of the etiology.
Erosion also contributes to extensive root wear, which in turn can result in decreased vertical dimension of occlusion (VDO). Patients with chronic eating disorders exhibit higher signs and symptoms from the temporomandibular joint than healthy ones [11]. They may also suffer from muscle sensitivity to palpation, emotional distress and bruxism.
In general, treating a young patient diagnosed with bulimia nervosa constitutes a challenge for the dental clinician.
Clinical Report
A healthy, 22 year old, female patient initially diagnosed with bulimia nervosa eight years previously; was referred for dental treatment.
Following a systematic approach [12], the first step was to establish communication with the patient. The patient had bulimic behavior from the age of 14 to 16. Using the BITE screening tool, a dialogue was initiated, in order to assess patient’s psychological and health status. Referring to that period the patient had very high scores in the BITE test and admitted to have adopted unhealthy dietary patterns and to have used laxatives and diuretics in order to lose weight. At the age of 16, the patient consulted a mental health clinician and a nutritionist and with her parents’ help she returned to normal eating behaviors.
Dental history included suffering from tooth hypersensitivity, periodically clenching and grinding of her teeth. As suggested by JADA guidelines, the patient was encouraged to maintain good oral and general health, to eat healthy snacks and monitor her dietary habits.
Extra-orally, the facial reference lines revealed a harmonious face with symmetry between the left and right sides (Figure. 1) [13]. At rest position (Figure. 2a), the total height of the maxillary incisors was visible, [14] whereas during smiling (Figure. 2b), a gingival band was exposed, [15] identifying a high smile line for the patient. Evaluating the smile width, the patient exposed twelve teeth and so she was considered as having a wide smile [16].

Figure 1. Initial facial view.


Figure 2a. Tooth exposure at rest, 2b. Smile line.
Intra-orally, observing the complete dentition of the patient, the signs of dental erosion were evident at the majority of tooth surfaces (Figure. 3 a-d). Using the TWI, [9] the patient had high scores (Table I-II). The teeth were free of restorations.
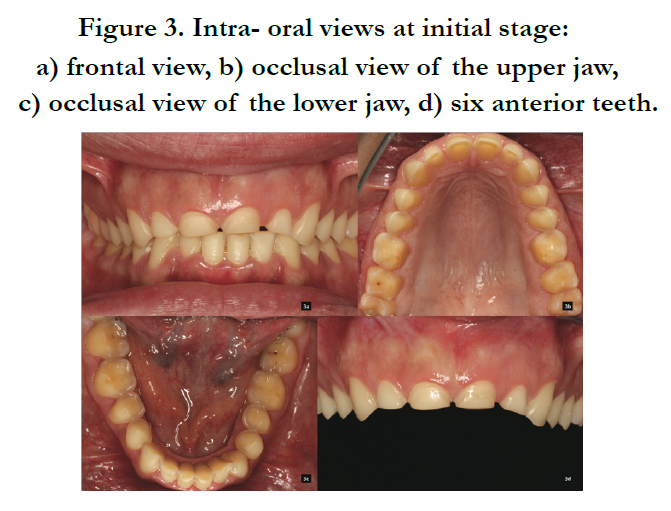

Figure 3. Intra- oral views at initial stage:
a) frontal view, b) occlusal view of the upper jaw, c) occlusal view of the lower jaw, d) six anterior teeth.
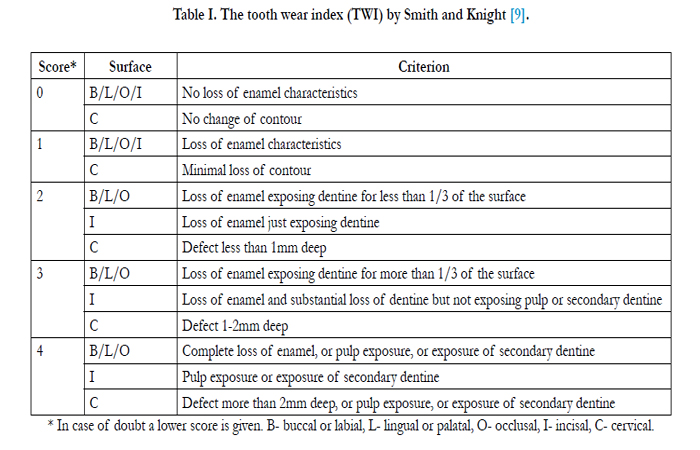

Table I. The tooth wear index (TWI) by Smith and Knight [9].
* In case of doubt a lower score is given. B- buccal or labial, L- lingual or palatal, O- occlusal, I- incisal, C- cervical.
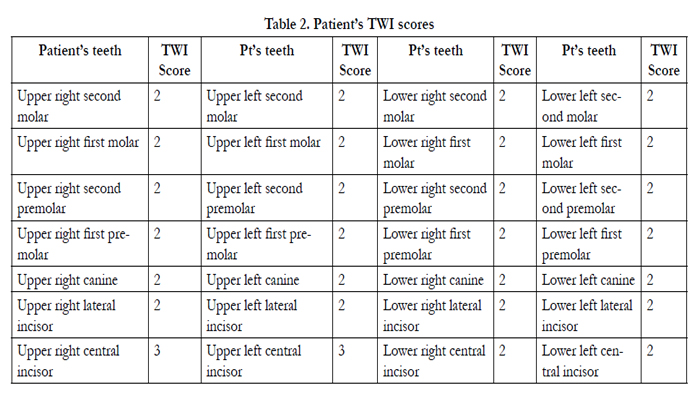
Table 2. Patient’s TWI scores
The appearance of the gingival tissues revealed accumulation of calculus and signs of gingival inflammation. There were no pockets measured. Examining the gingival margin outline, it could not be classified as esthetic [17]. The gingival margins of the central incisors were not symmetric to the canines’ and the lateral incisors revealed gingival margins at the same position with the central incisors.
In the panoramic radiograph (Figure. 4), the only pathology was a circumscribed area underneath the roots of the right mandibular first molar. The suspected tooth tested vital. The diagnosis was idiopathic pyknotic osteitis and the lesion required a radiograph six months later to reassure no further change.
The general diagnosis for the patient was worn dentition with localized patterns of erosion and abrasion due to the acidic attack because of the bulimic behavior of the patient. The signs of abrasion were due to the bruxing habits of the patient. The gingival inflammation was caused from the accumulation of dental plaque.
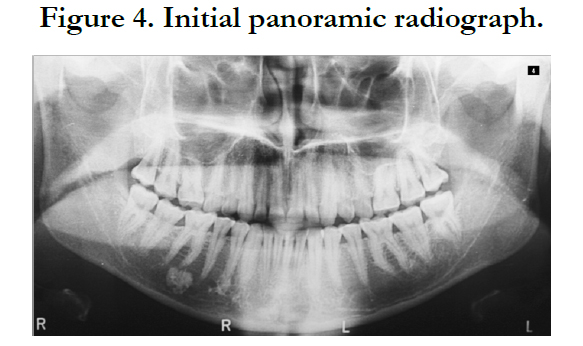

Figure 4. Initial panoramic radiograph.
Considering the classification system for the completely dentate patient, described by McGarry TJ et al. [18] the patient was classified as Class IV due to severely compromised tooth condition and substantially compromised occlusal scheme.
The initial restorative treatment was decided to be conservative with interim restorations. It was evaluated that the vertical dimension of occlusion was not reduced, so in order to restore the tooth size and reduce the soft tissue exposure during smile, it was decided to proceed with crown lengthening.
In collaboration with the periodontist, the patient was scheduled for crown lengthening. Procedures using Chu’s aesthetic gauges (Figure. 5a), [19] the tooth size discrepancies were quantified. Diagnostic waxing was done in order to match the existent width of the teeth with the height needed in order to achieve an esthetic result [17].
A surgical guide was fabricated in order to transfer information intraorally. The gingival margin outline was marked through the guide (Figure. 5b-c). Apart from the six maxillary anterior teeth the rest received more conservative crown lengthening procedures (Figure. 5d). The provisional restorations were adapted and the patient was allowed to heal for four months.
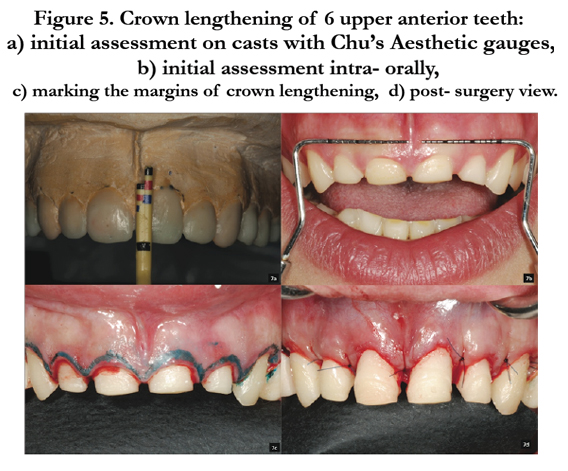

Figure 5. Crown lengthening of 6 upper anterior teeth:
a) initial assessment on casts with Chu’s Aesthetic gauges, b) initial assessment intra- orally,
c) marking the margins of crown lengthening, d) post- surgery view.
For the definite prosthetic rehabilitation, the teeth were prepared with caution due the proximity of the occlusal surfaces to the teeth’ pulps. Only the maxillary left first molar became sensitive and had to be treated endodontically. For esthetic reasons, it was decided to place all- ceramic single crowns (IPS e.max, Ivoclar Vivadent, Schaan, Liechtenstein) on the six maxillary and mandibular anterior teeth, whereas the posterior teeth were restored with metal-ceramic single crowns (Figure 6a-d, 7).
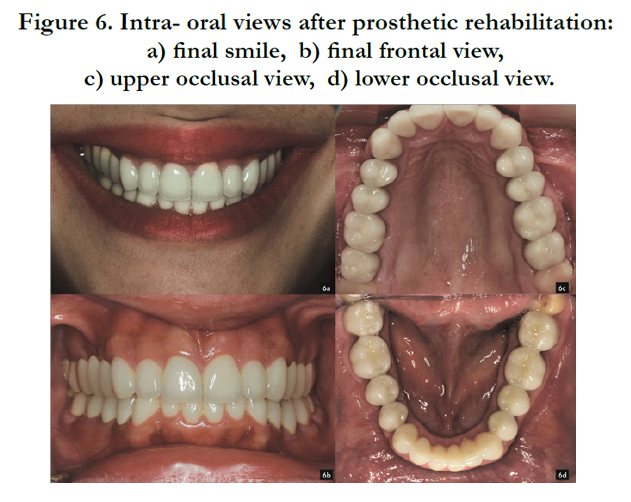

Figure 6. Intra- oral views after prosthetic rehabilitation:
a) final smile, b) final frontal view, c) upper occlusal view, d) lower occlusal view.

Figure 7. Final facial view.
At the 1-year recall appointment, the patient was functionally, esthetically and radiographically (Figure. 8) stable. There was no pathology or discomfort of the patient noticed or mentioned. The patient referred to the great impact that the dental rehabilitation had to her self- confidence and social life. Without any signs of bulimic behaviors and with a healthy figure she admitted that after restoring her oral health she became more determined to finish her studies and fulfill her dreams for the future.
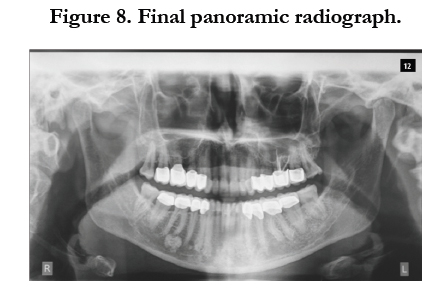

Figure 8. Final panoramic radiograph.
Discussion
Treating a patient with bulimia nervosa constitutes a great challenge and requires responsibility in order to maintain the desirable result and prevent future relapse. Bulimia remains the most frequent relapse diagnosis [20]. Keeping in mind the perspectives [21] referring to one third of the treated individuals to have early relapse and half of them to remain untreated 5 years after psychologic therapy, the dental patients with a history of bulimia nervosa require short recall intervals and thorough examination.
Considering the dental treatment, a factor of great impact is the evaluation of existing vertical dimension of occlusion. Gradual tooth wear is compensated by continuous eruption of the teeth, which maintain occlusal vertical dimension [22]. Furthermore, it is the phenomenon described as alveolar compensation [23]. It is observed that the worn upper teeth maintain contact with the lower teeth despite losing length. Alveolar bone and soft tissue appear to move in an occlusal direction. The teeth appear with short clinical crowns, which cannot be restored conventionally without increasing vertical space.
In this clinical report, no loss of vertical occlusion dimension was estimated, [24] but with space available. Manipulation of the mandible into centric relation provided space for restorative materials. Periodontal surgery was needed in this treatment in order to increase retention and to treat the soft tissue discrepancies.
Regarding the treatment option chosen for the patient, it is important to keep in mind the limitations associated with adhesive dentistry. The conservation of tooth structure was a major goal but there is a tendency to place excessively high expectations to adhesive dentistry. There are clinical reports of composite vertical bite reconstructions in eroded dentitions after 5 years but information on the use of resin composite materials to restore the complete occlusion of worn teeth is controversial and data are scarce [25-30]. In this clinical report, metal-ceramic crowns were chosen for posterior teeth and all-ceramic crowns for enhanced esthetics on anterior teeth. The amount of tooth wear and the revealed tooth surfaces from the surgical procedures required fullcoverage crowns for final rehabilitation.
Dental erosion is a contemporary, ‘silent’, multifactorial disease [26]. It is associated with modern lifestyle and the acquired eating patterns. In order to treat tooth wear, a careful weighing of the benefits and the risks of the treatment options that are considered, is crucial. Furthermore, there are no established guidelines for appropriate restorative methods and materials to treat erosive surfaces of a patient with history of bulimic behavior. There is a striking lack of evidence regarding the long-term performance of any treatment option. Interventional procedures should be reconsidered thoroughly and the advantages of both traditional and adhesive dentistry need to be utilized for optimum results.
References
- Critchley ME (1980) Butterworth’s Medical Dictionary. Butterworth-Heinemann, London.
- Walsh JME, Wheat ME, Freund K. Detection (2000) evaluation and treatment of eating disorders. The role of the primary Care Physician. J Gen Intern Med 15(8): 577-590.
- Lasater L, Mehler P (2001) Medical complications of bulimia nervosa. Eating Behavior 2(3): 279-292.
- Henderson M, Freeman CP (1997) A self-rating scale for bulimia. The ‘BITE”. Br J Psychiatry 150(1): 18-24.
- Rueda- Jaimes GE, Camacho Lopez PA, Rangel- Martinez- Villalba AM (2008) Internal consistency and validity of the BITE for the screening of bulimia nervosa in university students, Colombia. Eat Weight Disord 13(2): e35-9.
- Touger- Decker R (2006) Eating disorders: Detection and Referral- The role of the dental professional. Quint Int 37(3): 199-201.
- DeBate RD, Tedesco LA, Kerchbaum WE (2005) Knowledge of oral and physical manifestations of anorexia and bulimia nervosa among dentists and dental hygienists. J Dent Educ 69(3): 346-354.
- Lussi A, Jaeggi T (2008) Erosion- diagnosis and risk factors. Clin Oral Invest 12(1) : 5-13.
- Smith BG, Knight JK (1984) An index for measuring the wear of teeth. Br Dent J 156: 435-438.
- Berg- Beckhoff G, Kutschmann M, Bardehle D (2008) Methodological considerations concerning the development of oral dental erosion indexes: literature survey, validity and reliability. Clin Oral Invest 12(1): 51-58.
- Emodi-Perlman A, Yoffe T (2008) Prevalence of psychologic, dental and temporomandibular signs and symptoms among chronic eating disorders patients: A comparative control study. J Orofac Pain 22(3): 201-208.
- Fradeani M (2004) Esthetic analysis- A systematic approach to prosthetic treatment. Quintessence Publishing 19.
- Chiche GJ, Pinault A (1994) Artistic and scientific principles applied to esthetic dentistry.Esthetics of anterior fixed prosthodontics. Chicago, Quintessence. 13-32.
- Vig RG, Brundo GC (1978) The kinetics of anterior tooth display. J Prosthet Den 39(5): 502-504.
- Tjan AHL, Miller GD (1984) Some esthetic factors in a smile. J Prosthet Dent 51(1): 24-28.
- Dong JK, Jin TH, Cho HW, Oh SC (1999) The esthetic of the smile: A review of some recent studies. Int J Prosthodont 12(1): 9-19.
- Chiche GJ, Kokich VG, Caudillr (1994) Diagnosis and treatment planning of esthetic problems. Esthetic of anterior fixed prosthodontics. Quintessence. 33-52.
- McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, et al. (2004) Classification system for the completely dentate patient. J Prosthodont 13(2): 73-82.
- Chu SJ (2007) A biometric approach to predictable treatment of clinical crown discrepancies. Pract Proced Aesthet Dent 19(7): 401-409.
- Helverskov JL, Clausen L, Mors O, Frydenberg M, Thomsen PH , et al. (2010) Trans- diagnostic outcome of eating disorders: A 30-month followup study of 629 patients. Eur Eat Disord Rev 18(6): 452-463.
- Bouquot JE, Seime RJ (1997) Bulimia nervosa: dental perspectives. Pract Periodontics Aesthet Dent 9(6): 655-663.
- Sicher H ( 1949 ) Oral Anatomy (5th edtn). The C.V. Mosby Co, St Louis 270.
- Berry DC, Poole DF (1976) Attrition: possible mechanisms of compensation. J Oral Rehabil 3(3): 201-206.
- Rivera- Morales WC, Mohl ND (1992) Restoration of the vertical dimension of occlusion in the severely worn dentition. Dent Clin North Am 36(3): 651-664.
- Attin T, Filli T, Imfeld C, Schmidlin R (2012) Composite vertical bite reconstructions in eroded dentitions after 5,5 years: a case series. J Oral Rehabil 39(1): 73-79.
- Silva JSA, Baratieri LR, Araujo E, Widmer N (2011) Dental erosion: Understanding the Pervasive Condition. J Esthet Dent 23(4): 205-216.
- Vailati F, Belser UC (2008) Full-mouth adhesive rehabilitation of a severely eroded dentition: the three-step technique. Part 1. Eur J Esthet Dent 3(1): 30-44.
- Vailati F, Belser UC (2008) Full-mouth adhesive rehabilitation of a severely eroded dentition: the three-step technique. Part 2. Eur J Esthet Dent 3(2): 128-146.
- Vailati F, Belser UC (2008) Full-mouth adhesive rehabilitation of a severely eroded dentition: the three-step technique. Part 3. Eur J Esthet Dent 3(3):236-257.
- Mizrahi B (2008) Combining traditional and adhesive dentistry to reconstruct the excessively worn dentition. Eur J Esthet Dent 3(3); 270-289.





