Soft Tissue Calcification in Oral and Maxillofacial Imaging: A Pictorial Review
Omami G*
Assistant Professor, Department of Oral Health Practice, University of Kentucky, College of Dentistry, MN320 Chandler Medical Center, Lexington, KY, USA.
*Corresponding Author
Galal Omami, BDS, MSc, MDentSc, FRCD(C)
Assistant Professor, Department of Oral Health Practice,
University of Kentucky, College of Dentistry,
MN320 Chandler Medical Center, Lexington, KY 40536.
Tel: 859-257-5403
Email: jellodent@yahoo.com
Received: February 24, 2016; Accepted: March 29, 2016; Published: April 06, 2016
Citation: Omami G (2016) Soft Tissue Calcification in Oral and Maxillofacial Imaging: A Pictorial Review. Int J Dentistry Oral Sci. 03(4), 219-224.DOI : dx.doi.org/10.19070/2377-8075-1600046
Copyright: Omami G© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
2.Sialolith
3.Calcified Lymph Node
4.Tonsillolith
5.Phlebolith
6.Arterial Calcification
7.Antrolith
7.Calcified Stylohyoid Ligament
8.Myositis Ossificans
8.1.Longus Colli Tendinitis
9.Osteoma Cutis
5.References
Pathologic calcification of soft tissues occurs when calcium salts, essentially calcium phosphate, are deposited in an unorganized fashion in soft tissue (heterotopic calcification). There are three types of heterotopic calcification: 1) Dystrophic calcification which occurs in degenerating, inflamed, and necrotic tissues. 2) Metastatic calcification results when calcium salts are precipitated in normal tissue as a result of abnormal high levels of blood calcium or phosphate. 3) Idiopathic calcification (calcinosis) occurs in normal tissue despite normal blood calcium level.
Soft tissue calcifications in oral and maxillofacial region are relatively common. They are most often detected as incidental findings on routine radiographic examination. However, some soft tissue calcifications may be serious and require treatment or follow- up of the underlying cause. The anatomic location, number, distribution, and pattern of the calcifications are important interpretative criteria in radiographic evaluation of soft tissue opacities. In this pictorial review, we present the radiographic findings of soft tissue calcifications as seen on maxillofacial imaging.
Sialolith
Sialoliths are calcareous deposits in the salivary glands formed by precipitation of calcium salts around a central nidus that may consist of desquamated epithelial cells, bacterial debris, foreign body, or mucus plug [1]. Between 80% and 90% of salivary gland stones occur in the submandibular gland, 10% to 20% occur in the parotid glands, and only 1% to 7% occur in the sublingual glands [2]. Minor salivary glands stones are exceedingly rare, occurring most often in the upper lip and buccal mucosa.About 85% of submandibular salivary gland stones occur within the duct (Wharton’s duct), and 80% of submandibular stones and 60% of parotid stones are radiopaque on plain films [2]. Increased incidence of submandibular gland sialolithiasis compared to parotid gland, is attributed to the thicker, more mucous nature of submandibular gland secretions; their more alkaline pH, which helps precipitate salts; the higher concentration of hydroxyapatite and phosphatase; the narrower orifice of Wharton's duct compared to the caliber of the duct itself; long, tortuous and uphill course of the duct, and insinuation of the duct between mylohyoid and hyoglossus muscles.Gout is the only systemic disease known to cause salivary stones that are composed of uric acid. The majority of salivary stones are composed primarily of calcium phosphate [3]. Sialoliths occur as single or multiple stones and can cause swelling and pain. The symptoms are essentially experienced during salivary stimulation at mealtimes.
Large, well-calcified submandibular stones are clearly seen with panoramic and standard occlusal projections. When superimposed over the mandible, the radiopacity may be interpreted as enostosis within the bone. Stones in the parotid duct are best demonstrated by a periapical film of the buccal vestibule with one third the normal exposure time for this view. Sialoliths often are homogenously radiopaque and show evidence of multiple layers of calcification (laminated appearance) (Figure 1).However, about 20% of submandibular gland stones and 40% of parotid gland stones are unseen on routine plain films [3]. Because they (stones) are small and/or non-calcified (mucus plugs). Non-calcified stones are best diagnosedwith a sialogram.
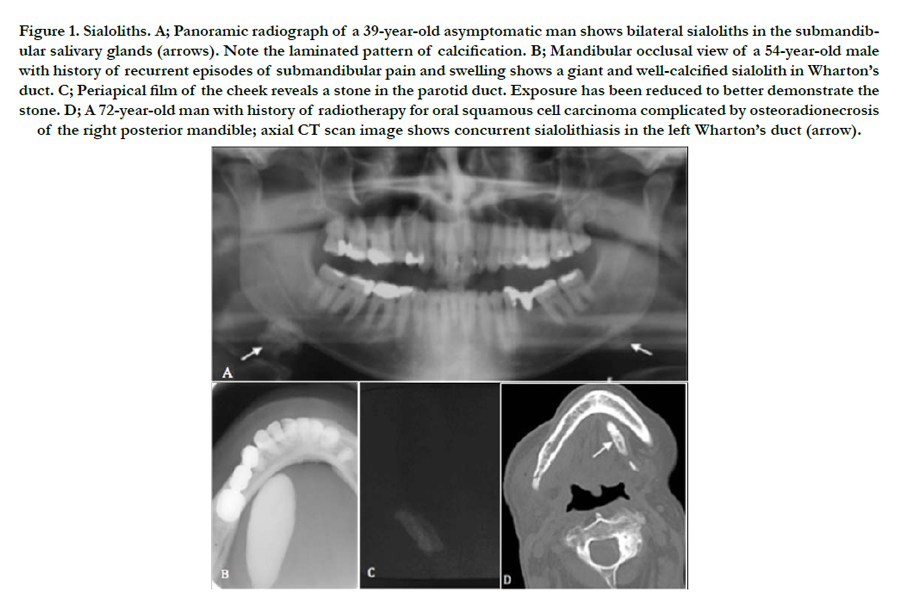
Figure 1. Sialoliths. A; Panoramic radiograph of a 39-year-old asymptomatic man shows bilateral sialoliths in the submandibular salivary glands (arrows). Note the laminated pattern of calcification. B; Mandibular occlusal view of a 54-year-old male with history of recurrent episodes of submandibular pain and swelling shows a giant and well-calcified sialolith in Wharton’s duct. C; Periapical film of the cheek reveals a stone in the parotid duct. Exposure has been reduced to better demonstrate the stone. D; A 72-year-old man with history of radiotherapy for oral squamous cell carcinoma complicated by osteoradionecrosis of the right posterior mandible; axial CT scan image shows concurrent sialolithiasis in the left Wharton’s duct (arrow).
Calcified Lymph Node
Lymph nodes in the head and neck are usually enlarged during inflammatory processes. Subsequently, the nodes become fibrous and foci of calcification start to develop. Tuberculous lymphadenitis (scrofula) is probably the most prevalent disease process associated with dystrophic calcification of sclerotic nodes [4]. Radiographically, the calcifications appear as multiple mottled radiopacities distributed along the course of a nodal chain. Calcific lymph nodes most often are irregular with a cauliflower appearance (Figure 2). In absence of clinical symptoms, a calcified submandibular lymph node is sometimes difficult to differentiate from a sialolith in submandibular salivary gland. However, a sialogram is useful in distinguishing between the two entities. Usually there is no treatment for calcified lymph nodes.
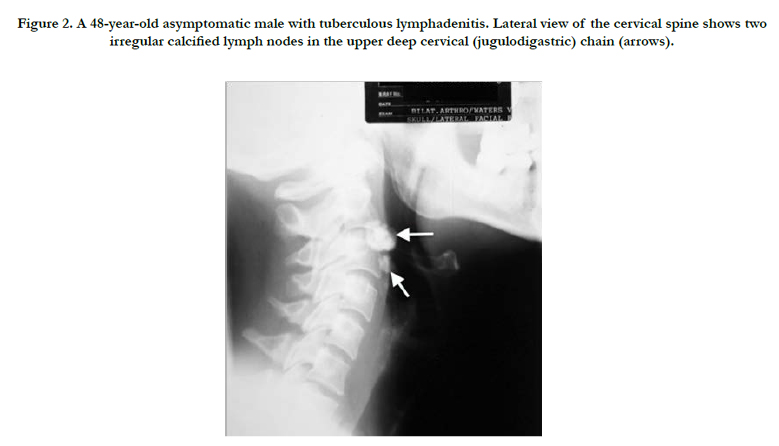

Figure 2. A 48-year-old asymptomatic male with tuberculous lymphadenitis. Lateral view of the cervical spine shows two irregular calcified lymph nodes in the upper deep cervical (jugulodigastric) chain (arrows).
Tonsillolith
Tonsillar calcifications are oropharyngeal concretions formed as a sequela of chronic tonsillitis where residual long-standing inflammation can serve as the nidus for dystrophic calcification [5]. In the panoramic film, tonsilloliths usually appear as a cluster of multiple small radiopacities superimposed over the midramus region (Figure 3).
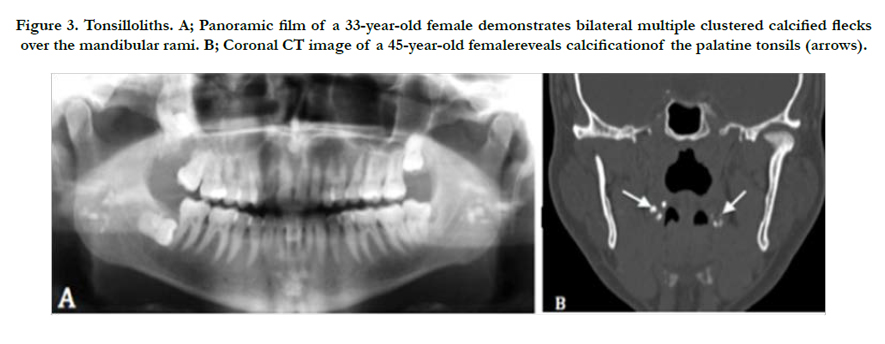
Figure 3. Tonsilloliths. A; Panoramic film of a 33-year-old female demonstrates bilateral multiple clustered calcified flecks over the mandibular rami. B; Coronal CT image of a 45-year-old femalereveals calcificationof the palatine tonsils (arrows).
Phlebolith
Phleboliths are calcified thrombi that occur in vascular channels associated withhemangiomas and venolymphatic malformations usuallywithin the soft tissues of the head and neck [6]. On a radiograph, they appear as round or oval calcified bodies, which may exhibit concentric calcific rings similar to the cross section of an onion. However, some phleboliths merely consist of a calcificed outer shell, a radiolucent layer beneath this shell, and a radiopaque central core (bull’s eye or target appearance) (Figure 4).Phleboliths are usually multiple and may vary in number from several to dozens within the affected area.
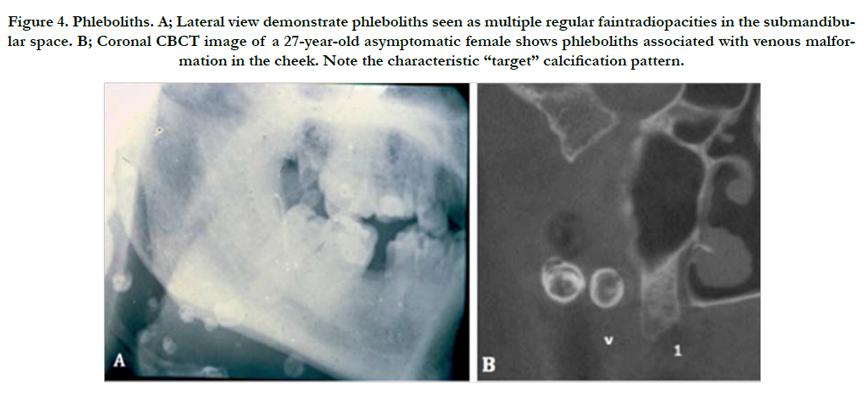
Figure 4. Phleboliths. A; Lateral view demonstrate phleboliths seen as multiple regular faintradiopacities in the submandibular space. B; Coronal CBCT image of a 27-year-old asymptomatic female shows phleboliths associated with venous malformation in the cheek. Note the characteristic “target” calcification pattern.
Arterial Calcification
There are two major types of pathologic calcification of arteries can be recognized radiographically and histologically. Monckeberg’s medial calcification (arteriosclerosis) and intimal calcification (atherosclerosis) [1]. Monckeberg’s medial calcification is characterized by deposition of calcium in the medial layer of an artery. These deposits do not narrow down the vessel or interfere with flow. This type of calcification is most frequently seen in elderly people. In the extracranial head and neck region the facial artery is affected most often [7] .On a radiograph, the pattern of mural calcification outlines an image of the affected artery (tramtrack appearance) (Figure 5). Intimal calcification is characterized by deposition of calcium in the atheromatous plaques within the intima of arteries. The lumen of the affected vessel is usually narrowed resulting in arterial insufficiency [8]. The most common location for an atherosclerotic plaque lesion is at the carotid bifurcation, therefore, it may be visible in the panoramic radiograph as a heterogenous radiopacity in the soft tissues of the upper neck at the level of the intervertebral space between C3 and C4 (corresponding to the level of carotid bifurcation) (Figure 5). Calcified atheromatous plaque in the carotid bifurcation may be confused with calcified triticeous cartilage, but the irregular size and shape of the former should be discriminatory.
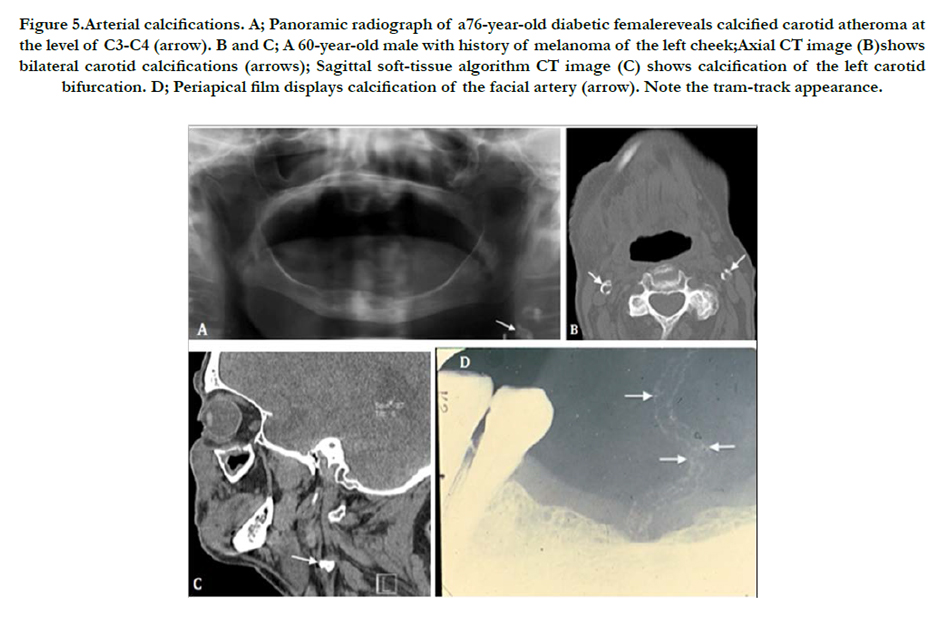
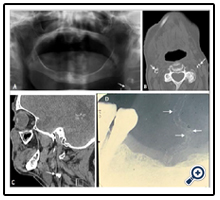
Figure 5.Arterial calcifications. A; Panoramic radiograph of a76-year-old diabetic femalereveals calcified carotid atheroma at the level of C3-C4 (arrow). B and C; A 60-year-old male with history of melanoma of the left cheek;Axial CT image (B)shows bilateral carotid calcifications (arrows); Sagittal soft-tissue algorithm CT image (C) shows calcification of the left carotid bifurcation. D; Periapical film displays calcification of the facial artery (arrow). Note the tram-track appearance.
Antrolith
Antrolith is a calcified mass in the maxillary sinus arises from the deposition of mineral salts around a central nidus which may be a blood clot, bone fragment, root tip, foreign body, or inspissated pus or mucus. On radiographic examinations, antroliths may be round to ovoid and irregular, ragged, or smooth in outline (Figure 6). Most antroliths are usually associated with the radiographic signs of sinusitis including mucoperiosteal thickening, polyps, and air-fluid levels [9]. When similar calcification occurs in the nasal fossa, it is called a rhinolith.
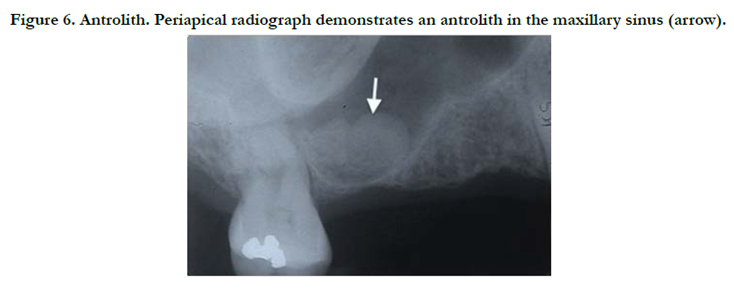
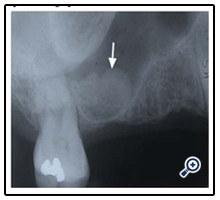
Figure 6. Antrolith. Periapical radiograph demonstrates an antrolith in the maxillary sinus (arrow).
Calcified Stylohyoid Ligament
Calcification of the stylohyoid ligament usually occurs bilateral and extends downward from the skull base. In majority of cases, the individuals are asymptomatic, and no treatment is required. Symptoms associated with calcified stylohyoid ligament are called Eagle’s syndrome resulting from cranial nerve impingement. These symptoms include vague deep throat pain on swallowing, turning the head, or opening the mouth, and otalgia (earache). Patient typically has a history of neck trauma or surgery (e.g., tonsillectomy). However, Calcification of stylohyoid ligament is relatively a common incidental finding on panoramic radiograph [10]. It appears as a thin, long, tapering radiopaque process extending downwards from the styloid process. The farther the mineralized ligament extends toward the hyoid bone, the more likely be interrupted by radiolucent junctions (pseudoarticulations) (Figure 7). Surgical resection is required in symptomatic patients.
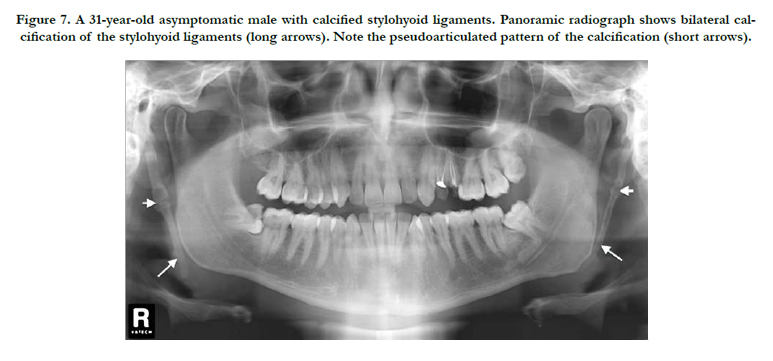
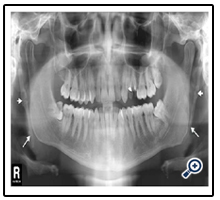
Figure 7. A 31-year-old asymptomatic male with calcified stylohyoid ligaments. Panoramic radiograph shows bilateral calcification of the stylohyoid ligaments (long arrows). Note the pseudoarticulated pattern of the calcification (short arrows).
Myositis Ossificans
Myositis ossificans results from trauma or heavy muscular strain that occurs in certain occupations and sports. The injury leads to hemorrhage within the interstitial tissue of the muscle. During the healing process, the hematoma in the traumatized region gets organized and subsequently undergoes metaplasia to osseous tissue. In the region of head and neck, muscles of mastication and sternomastoid are the most commonly involved [11]. When the lesion is associated with a muscle of mastication, it is usually associated with trismus. On a radiograph, the linear streaks (pseudotrabeculae) running in the same direction as the normal muscle fibers are very characteristic for myositis ossificans (Figure 8). The lesion is treated by surgical excision of the calcified mass with physiotherapy to reduce the likelihood of recurrence.
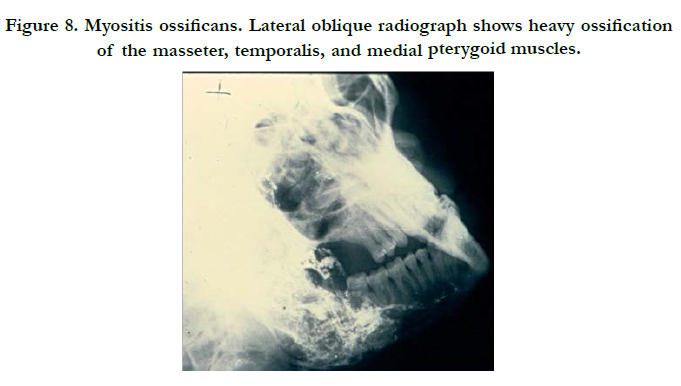
Figure 8. Myositis ossificans. Lateral oblique radiograph shows heavy ossification of the masseter, temporalis, and medial pterygoid muscles.
Longus Colli Tendinitis
Longus colli tendinitis, also known as retropharyngeal calcific tendinitis, is secondary to crystalline calcium compounds in the superior fibers of the longus colli muscle. The proposed pathophysiology is that rupture of these to calcium crystals provokes an inflammatory response in the surrounding longus colli that leads to formation of reactive fluid in the retropharyngeal space surrounding the muscle [12]. The typical clinical presentation is acute onset of neck pain, dysphagia, odynophagia, and low-grade fever. The pathognomonic radiographic findings consist of amorphous calcification anterior to C1-C2 and prevertebral soft tissue swelling or effusion (Figure 9). Most cases are self-limiting and resolve spontaneously after 1-2 weeks.
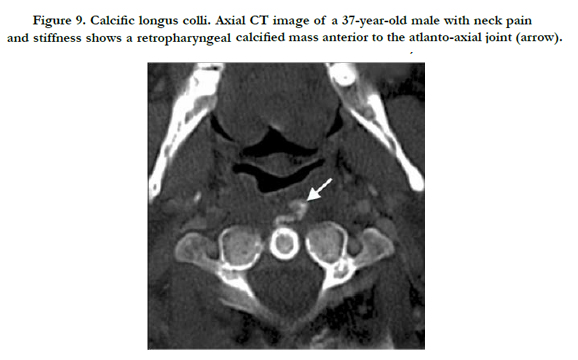
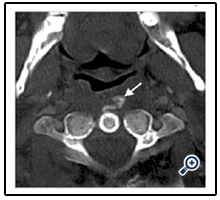
Figure 9. Calcific longus colli. Axial CT image of a 37-year-old male with neck pain and stiffness shows a retropharyngeal calcified mass anterior to the atlanto-axial joint (arrow).
Osteoma Cutis
Osteoma cutis is a rare soft tissue calcification in the skin. It is usually associated with chronic acne or dermatosis scars. The tongue is the most common intraoral site (osseous choristoma) [13]. They are found incidentally on radiographic examinations. They appear as tiny doughnut-shaped radiopacities with radiolucent centers that represent central marrow cavities (Figure 10).
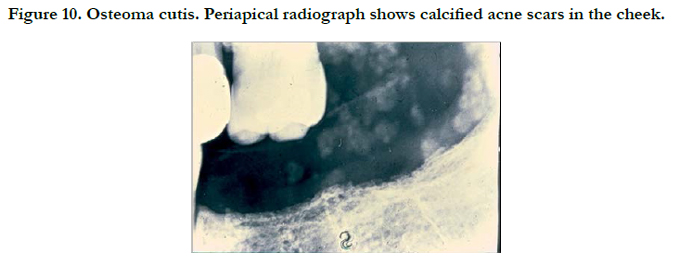
Figure 10. Osteoma cutis. Periapical radiograph shows calcified acne scars in the cheek.
Cysticercosis
When an individual ingests eggs of the pork tapeworms from contaminated water or food, the larval form of the tapeworms are hatched in the gastrointestinal tract, and then pass into the vascular system. They are eventually deposited in various tissues and organs of the body. After their death, the larval spaces are replaced byscarring tissue that later becomes calcified [14]. These calcifications in muscle and subcutaneous tissue are visible on a radiograph as multiple ovoid or elliptical radiopacities resembling grains of rice.
Conclusion
This comprehensive review should be of interest and aid learning for both specialty and general dental practitioners encountering soft tissue calcification in the oral and maxillofacial imaging.
References
- Monsour PA, Romaniuk K, Hutchings RD (1991) Soft tissue calcifications in the differential diagnosis of opacities superimposed over the mandible by dental panoramic radiography. Aust Dent J 36(2): 94-101.
- Lustmann J, Regev E, Melamed Y (1990) Sialolithiasis: a survey on 245 patients and a review of the literature. Int J Oral Maxillofac Surg 19(3): 135-138.
- Williams MF (1999) Sialolithiasis. Otolaryngol Clin North Am 32(5): 819- 834.
- Muto T, Michiya H, Kanazawa M, Sato K (1991) Pathological calcification of the cervico-facial region. Br J Oral Maxillofac Surg 29(2): 120-122.
- Pruet CW, Duplan DA (1987) Tonsil concretions and tonsilloliths. Otolaryngol Clin North Am 20(2): 305-309.
- Zachariades N, Rallis G, Papademetriou J, Konsolaki E, Markaki S, et al. (1991) Phleboliths: a report of three unusual cases. Br J Oral Maxillofac Surg 29(2): 117-119.
- Friedlander AH, Altman L (2001) Carotid artery atheromas in postmenopausal women: their prevalence on panoramic radiographs and their relationship to atherogenic risk factors. J Am Dent Assoc 132(8): 1130-1136.
- Miles DA, Craig RM, Langlais RP, Wadsworth WC (1983) Facial artery calcification: a case report and its clinical significance. J Can Dent Assoc 49(3): 200-202.
- Cohen MA, Packota GV, Hall MJ, Steinberg J (1991) Large asymptomatic antrolith of the maxillary sinus: report of a case. Oral Surg Oral Med Oral Pathol 71(2): 155-157.
- Balbuena L, Hayes D, Ramirez SG, Johnson R (1997) Eagle's syndrome (elongated styloid process). South Med J 90(3): 331-334.
- Mevio E, Rizzi L, Bernasconi G (2001) Myositis ossificans traumatica of the temporal muscle: a case report. Auris Nasus Larynx 28(4): 345-347.
- Eastwood JD, Hudgins PA, Malone D (1998) Retropharyngeal effusion in acute calcific prevertebral tendinitis: diagnosis with CT and MR imaging. Am J Neuroradiol 19(9): 1789-1792.
- Shigehara H, Honda Y, Kishi K, Sugimoto T (1998) Radiographic and morphologic studies of multiple miliary osteomas of cadaver skin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 86(1): 121-125.
- Romero De Leon E, Aguirre A (1995) Oral cysticercosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79(5): 572-577.





