A Comparison of Two Dental Age Estimation Techniques in Contemporary American Whites: The Moorrees and Demirjian Approaches
Tony L. Skanchy1*, Maness H2, Al Dayeh A3, Harris EF4
1 Orthodontic Graduate Student, Department of Orthodontics, School of Dentistry, University of Tennessee, Memphis, TN, USA.
2 Assistant Professor, Department of Orthodontics, School of Dentistry, University of Tennessee, Memphis, TN, USA.
3 Assistant Professor, Department of Orthodontics, School of Dentistry, University of Tennessee, Memphis, TN, USA.
4 Professor, Department of Orthodontics, School of Dentistry, University of Tennessee, Memphis, TN, USA.
*Corresponding Author
Dr. Tony L. Skanchy,
Orthodontic Graduate Student, Department of Orthodontics, 875 Union Avenue, Memphis, Tennessee 38163, USA.
Tel: 859-489-1343
E-mail: tonyskanchy@yahoo.com
DrSkanchy@gmail.com
Received: March 05, 2016; Accepted: May 18, 2016; Published: May 20, 2016
Citation: Tony L. Skanchy, Maness H, Al Dayeh A, Harris EF (2016) A Comparison of Two Dental Age Estimation Techniques in Contemporary American Whites: The Moorrees and Demirjian Approaches. Int J Forensic Sci Pathol. 4(5), 243-248.doi: dx.doi.org/10.19070/2332-287X-1600058
Copyright: Tony L. Skanchy© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: Historically, dental age estimation has used the methods of Moorrees, Fanning and Hunt1 and Demirjian, Goldstein and Tanner5. The purpose of this study is to apply these two methodologies to a contemporary sample of American whites, ages 9-14 years, and to evaluate the optimal concordance between the Moorrees (14-grade system) and the Demirjian (8-grade system) methods.
Materials and Methods: 199 pre-treatment panoramic radiographs of syndrome-free American white children, ages 9-14 years (97 boys, 102 girls), were evaluated by the author. Tooth mineralization stages were scored using seven left mandibular teeth using both techniques. The age of the subjects was predicted using the Demirjian and Moorrees approaches and compared to their actual (chronological) age. Survival analyses was performed, by sex, to include a comparison of the same sample of radiographs using the two methods of Moorrees et al. and Demirjian et al.
Results: Both methods, particularly the Moorrees approach, underestimated children’s ages. Applying the Demirjian method resulted in a mean overestimation of 0.1 years for girls and a mean underestimation of 1.6 years for boys, while the Moorrees technique resulted in an average underestimation of 2.3 years for girls and 1.9 years for boys.
Conclusion: Neither the Demirjian nor the Moorrees techniques accurately estimate chronological age in our sample of contemporary American whites. The reason these methods underestimated chronological age is most likely multifactorial, due to differences in methods and environments.
2.Materials and Methods
3.Results
3.1 Moorrees method
3.2 Demirjian method
4.Discussion
5.Conclusion
6.References
Introduction
Differences in the development among children of the same chronological age have led to the concept of physiological age as a means of defining a person’s progress towards biological maturity. Physiological age, or its frequently used synonyms of biological and developmental age, are measures for describing the status of a child, whereas chronological or calendric age convey only an approximation of this status because of the range in development observed for any given age [1].
Physiological age refers to the evaluation of maturation of one or more tissue systems. Developmental indicators include bone development, secondary sex characteristics, stature or weight [1] and tooth development. Dental age can be determined by the emergence of teeth through the gingival tissues and also by assessing tooth mineralization by radiographic examination. Dental maturity has played an important role in estimating the chronological age of individuals because of the reported low variability of dental indicators [2] since mineralization rates are more controlled by genes than by environmental factors [3].
The assessment of tooth mineralization is a superior method of evaluation compared to tooth emergence for assessing dental maturation for several reasons. The majority of teeth can be assessed using tooth formation at any given time, while emergence only allows us to see the teeth at a specific phase of short duration in the continuous process of eruption. Emergence of a tooth is a short lived event and its exact time is difficult to determine, whereas the formation of a tooth is a continuous process which can be observed at almost any time point. The emergence of teeth are also more prone to environmental factors such as infection, loss of deciduous predecessors, or lack of space in the dental arch, explaining some part of the variation in root length at emergence [1]. The early extraction of a deciduous tooth has a delaying effect on the emergence of its permanent successor, and late extraction favors early emergence. Any combination of these environmental factors may give a false estimation in the assessment.
Accurate age estimation is a useful part of the identification process for both living and deceased individuals. Accurate dental age estimation can help those in government positions, including identification purposes, prosecuting criminals, and making other important connections [4]. Estimating chronological age can be useful in societies for school attendance, social behaviors, employment, marriage and other reasons. Dental age information is also helpful in the field of dentistry, which can be used to accurately time treatment procedures and help predict eruption sequences in the field of orthodontics and pediatric dentistry [3].
There are different methods available to estimate dental age. Two common methodologies were developed (1) by Moorrees, Fanning and Hunt [1] and (2) Demirjian Goldstein and Tanner [5]. Moorrees’ method uses 13 developmental stages for single rooted teeth and 14 stages for multiple rooted teeth (Figure 1). Each developmental stage is assigned a numerical value specific to the tooth being evaluated. These numerical values are averaged to estimate the individual’s dental age. Dental age is the age at which the average child in the reference group exhibits that extent of tooth mineralization. Consequently, it is important that the reference group be representative of the timing and rate of dental development. The Demirjian technique uses 8 stages of tooth development (Figure 2), and inspects the 7 mandibular permanent teeth in one quadrant (omitting the third molar). Each stage of each tooth is assigned a specific code. These codes are weightedand summed, which gives a numerical value that is converted into a sex-specific dental age.
The purpose of this study was to test the accuracy of the dental agesproposed by (1) Moorrees, Fanning and Hunt [1] and (2) by Demirjian, Goldstein and Tanner [5] as applied to a contemporary population of American whites, ages 9-14 years.
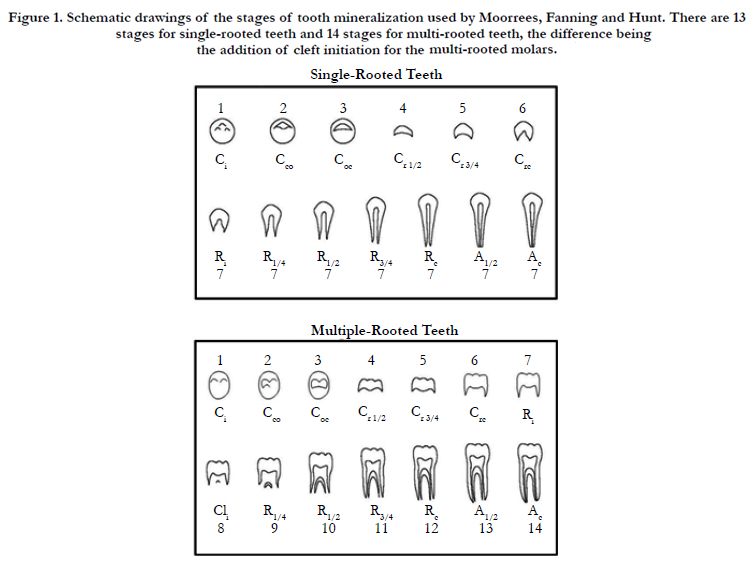

Figure 1. Schematic drawings of the stages of tooth mineralization used by Moorrees, Fanning and Hunt. There are 13 stages for single-rooted teeth and 14 stages for multi-rooted teeth, the difference being the addition of cleft initiation for the multi-rooted molars.
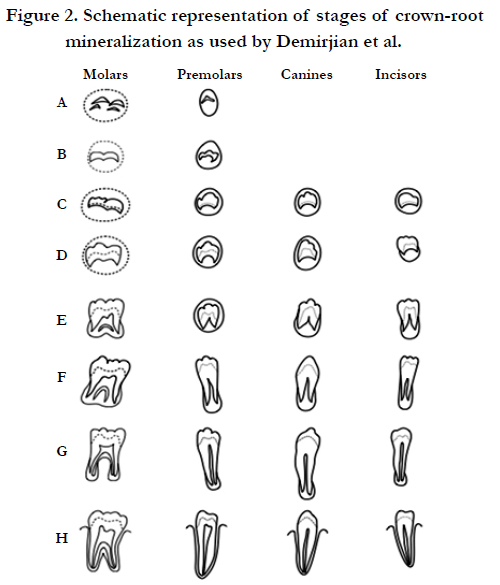
Figure 2. Schematic representation of stages of crown-root mineralization as used by Demirjian et al.
Materials and Methods
Institutional review board approval for this retrospective study was obtained from our institution (IRB# 14-03187-XM). Pretreatment panoramic radiographs of 199 routine orthodontic cases (97 boys; 102 girls) were studied. Patients were selected to be used from Dolphin Imaging (Chatsworth, CA) in chronological order. There was an evenly distributed number of males and females in each age group (Table 1). JPG images of the pretreatment panoramic radiographs were retrieved from Dolphin Imaging. Those of poor quality were omitted. All cases were American whites, free of syndromes, clefts, or systemic conditions. Patient’s age at the time of the initial radiograph were between 9 to 14 years of age, which spans the modal age at the start of orthodontic treatment. All radiographs were imported to Adobe Photoshop CC (San Jose, CA) and were enhanced (contrast and brightness) and magnified to aid the analysis of the mineralization stages. The first author collected all data and was blinded to the patient’s ages throughout data collection and analysis. The mandibular left 7 teeth (excluding the third molar) were each scored using the Demirjian 8-grade scheme, and then independently using the Moorrees system (13 grades for single-rooted teeth; 14 for molars). The Demirjian and Moorrees analyses were both completed on each patient, in the same sitting, before moving to the next patient to ensure consistency in the developmental stage assignments. For comparability, only the lower left 7 teeth were scored using both methods.
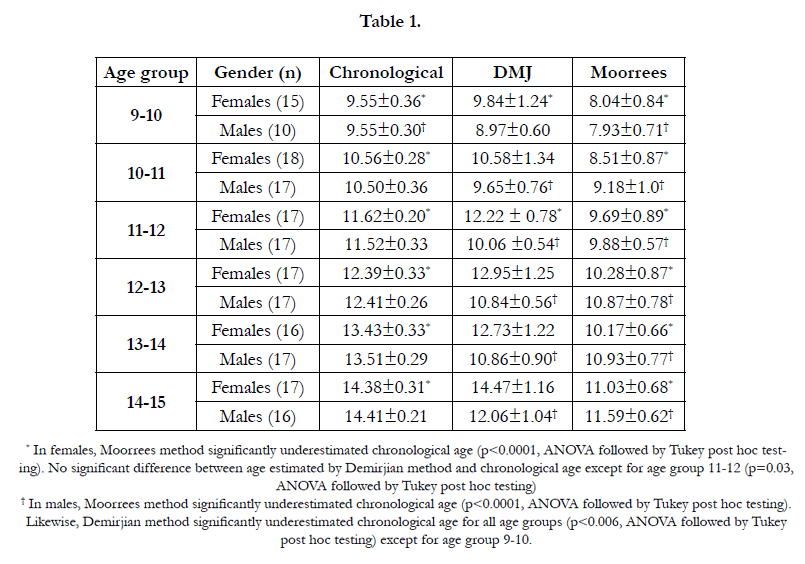

Table 1
oorrees et al. [1] used survival analysis to determine the median chronological age at which each observed stage of each tooth occurred [6]. Dental age estimates in the Demirjian [5] scheme likewise were derived from survival analysis. Median chronological age was calculated, by sex, using proportional hazards analysis. This method does not make the assumptions of normality or of equivalent variances. Several grades of each tooth type were untestable because the age range (9-to-14 years) was restricted. This affected the younger grades in young children when most permanent teeth mineralize [7]. Tooth formation ageswere normally distributed as tested with the Wilks and Kolmogorov-Smirnoff tests. Cox's proportional hazards analysis was used to test for sex differences. Analysis of covariance was used to compare the accuracy of the dental age estimates, with chronological age as the covariate, and to compare the Moorrees and Demirjian methods. The conventional level of alpha was used; tests were two-tail. Al
statistical tests were done using JMP statistical package (SAS Institute Inc., Cary, NC) and SPSS (Chicago, IL). Within each age group, ANOVA was followed by post hoc analysis to compare the two age estimation methods to chronological age.
Intra observer analysis was performed using the two grading schemes, which were assessed separately because they embody different levels of detail. Thirteen cases (91 teeth) were re-scored five weeks after completing data collection. The Moorrees system, with 14 stages, had a concordance rate of 85% (77/91); none of the 14 differences exceeded one stage. Gamma, a common measure of association, was 0.97 (SE = 0.016). The kappa statistic was 0.75 (SE = 0.053). The most common confusion was determining whether the root apex was open, partially closed or fully closed. Moorrees1reported a higher concordance rate (˜90%), but they (notably Elizabeth Fanning) originated the system, had considerable familiarity with it, and actually simplified it from even-more detailed gradations [4].
The Demirjian system, with 8 grades, was concordant for 91% of the teeth (83/91), again with no difference exceeding one stage. Gamma was 1.00 (SE = 0.005) and kappa was 0.85 (SE = 0.052). Kappa was higher for the Demirjian system because the stages are better defined and do not depend on the observer’s ability to envisage completed tooth size.
Results
Moorrees and coworkers [1] understood the accelerated dental formation rates of girls compared to boys, and they presented their data separately by sex. Inspection of Moorrees’ tables show that, predictably, girls achieved most formation stages at earlier chronological ages than boys. A statistically significant sex difference also is evident in the present data when chronological ages are plotted against the child’s dental age using the Moorrees method (Figure 3 and 4). The advancement of dental age with chronological age was statistically parallel in the two sexes (P = 0.2931), but girls attained most mineralization stages at earlier chronological ages than boys. Averaging across the 9-14 year age span, girls are advanced compared to boys by about 0.5 years (P < 0.0001) based on marginal least squares.Analysis showed that dental age estimation significantly underestimated chronological age. The average estimated dental age (DA) minus chronological age (CA) was -1.9 years for boys and -2.3 years for girls. These departures from zero (DA=CA) were highly significant by t-test (P < 0.0001)for both sexes. Within each age group (9-10, 10-11, 11-12, 12-13, 13-14, 14-15), the Moorrees method underestimated chronological age in boys by a minimum of 1.3 years and a maximum of 2.8 year and in females by a minimum of 1.5 years and a maximum of 3.3 years (Table 1).
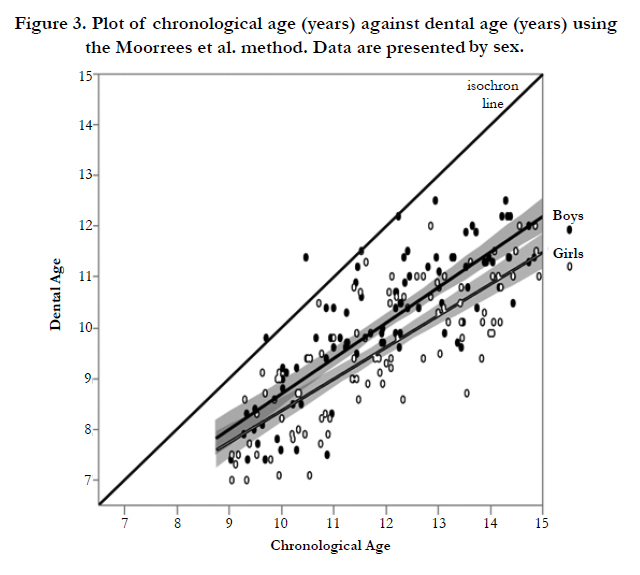
Figure 3. Plot of chronological age (years) against dental age (years) using the Moorrees et al. method. Data are presented by sex.
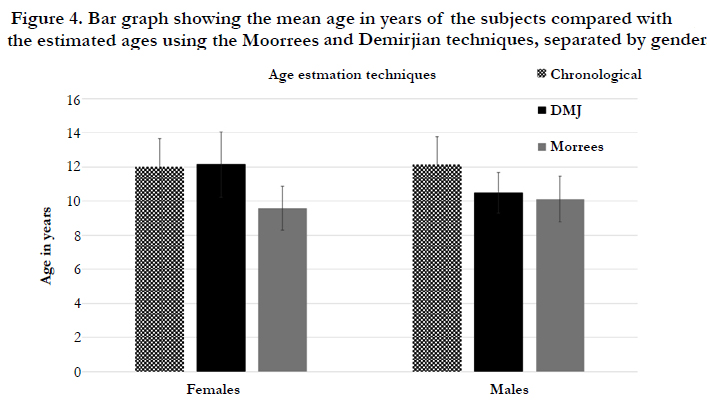
Figure 4. Bar graph showing the mean age in years of the subjects compared with the estimated ages using the Moorrees and Demirjian techniques, separated by gender.
The Demirjian group used multiple linear regression to develop sex-specific weighting coefficients to account for sexual dimorphism. Consequently, if the sex differencein the contemporary American sample were the same as in Demirjian’s French-Canadian reference sample, the best-fit regression lines for boys and girls would be superimposed (Figure 5).
When the Demirjian method is applied to the present data (Figure 4 and 5), the following information is noted: (1) Neither regression line intersects the origin, (2) there is a substantial difference between the best-fit lines for boys and girls (P < 0.0001), (3) girls mature faster than boys (P < 0.0001); and (4) the regression coefficients were significantly below 1, meaning that dental age progressed more slowly with advancing chronological age than occurred in Demirjian’s sample.
The considerable boy-girl difference in rates is due to Demirjian’s weighting coefficients. Demirjian et al. adjusted the weights of the coefficients in the two sexes to align them, and remove the sexual dimorphism in the French-Canadian children. When applied to a sample where the sexual dimorphism is different, the sex-specific results will be altered. In the present situation, their “sex adjustment” accentuated the sex difference in the rates of dental maturation. Cox’s proportional hazards analysis was used to calculate the median ages at attainment, by sex, in contemporary whites using the Demirjian method. On average, girls were 1.7 years ahead of boys in the 9-to-14 age interval. Using a common index of sexual dimorphism [8], [(¯XM - ¯XF ) / XM ]100, girls are dentally advanced over boys by about 16%. The average dental age (DA) minus chronological age (CA) using the Demirjian approach was -1.6 years for boys and .1 years for girls. Within each age group (9-10, 10-11, 11-12, 12-13, 13-14, 14-15), the Demirjian method age estimation in boys ranged from an overestimation of .6 years to an underestimation of 2.3 years, while in females it ranged from an overestimation of age from .6 years to an underestimation of .7 years (Table 1).
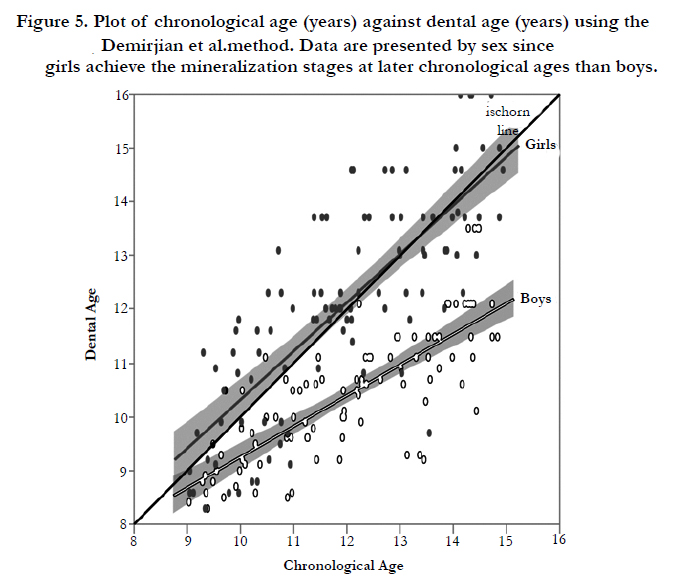
Figure 5. Plot of chronological age (years) against dental age (years) using the Demirjian et al.method. Data are presented by sex since girls achieve the mineralization stages at later chronological ages than boys.
Discussion
Both Moorrees et al. (1963) [1] and Demirjian et al. [5] were careful to stipulate that their results may be restricted to the samples studied. There have been several studies that have shown that most groups mature faster than the French-Canadian children assessed by Demirjian, Goldstein, and Tanner [9,10].
The substantial underestimation of age using the Moorrees method, about 2 years, merits discussion. There are several additive issues. One, the children’s records used by Moorrees et al. are far-removed in time, and their environment (e.g. childhood illness, diet, exercise level, secular trends) was distinct from those of children today. Two, Moorrees’ method of averaging across teeth was a good start, but it does not account for statistical redundancy (covariance) of data or for differences in variability among teeth and grades. Three, scrutiny of Moorrees’ study shows that the dental age data are fundamentally different from how they are used by others. That is, Moorrees used records from two studies (Boston, MA, Yellow Springs, OH) [11,12]. With longitudinal data, the onset of a mineralization stage can be pinpointed (within limits of the examination interval), and the data in Moorrees’ article pertain to those starting ages. From comparison of adjacent records, the onset of a tooth stage initiation can be bracketed.
With cross-sectional studies-which are far more common-researchers cannot estimate the starting age of a tooth-grade because, examining a child only once, says nothing about how long the presenting condition has existed. Cross-sectional studies estimate the average age at which children in the sample exhibit a given grade. Ages are necessarily combined whether a child has just entered a stage, is near the average of the duration, or almost ready to advance to the next stage. The age at onset of a stage necessarily occurs before its average age. Clinically, the issue normally is to compare a patient to other children who also exhibit a given stage of dental development-that is, the average age of attainment. This is not a new finding, though generally unappreciated; Smith described the difference in 1991 [11], and Harris provided a worked example [12]. Both the Moorrees and Demirjian studies relied on longitudinal data. The better predictive accuracy of the Demirjian study appears to stem from the use of weighting coefficients intended to minimize redundancy of information among teeth. These results support that caution should be used when applying both techniques to estimate dental age in subjects between the ages of 9-14.
Conclusion
This study examined the accuracy of dental ages applying the Moorrees and Demirjian methods to 199 contemporary American white children, 9-to-14 years of age. The following can be concluded from the investigation:
- Neither method accurately estimates the dental age of our sample of contemporary American whites.
- Overall, both methods underestimate the subjects’ chronological ages.
- The most accurate method was the application of the Demirjian technique to female subjects.
- The difference in the prediction of developmental age from chronological age (DA-CA)with the Demirjian standardsaveraged-1.6 years for boys and 0.1 years for girls, while that of the Moorrees standards was -1.9 years for boys and -2.3 years for girls.
- Differences are most likely multifactorial, possibly due to differences in evaluation methods, radiographic methods, environments, and our select age group.
- A correction of the Demirjian equations is suggested to align the estimates.
References
- Moorrees CFA, Fanning EA, Hunt Jr EE (1963) Age variation of formation stages in ten permanentteeth.JDentRes 42(6):1490-1502.
- Willems G, Van Olmen A, Spiessens, Carels C (2001) Dental age estimation in Belgian children: Demirjian's technique revisited. J Forensic Sci ;46(4): 893-895.
- Chaillet N, Willems G, Demirjian A (2004) Dental maturity in Belgian children using Demirjian’s method and polynomial functions: new standard curves for forensic and clinical use. J Forensic Odontostomatol 22(2): 18-27.
- Finney DJ (1971) Probit analysis, (3rd edn),Cambridge University Press, Cambridge, England. J Pharm Sci 60(9): 1432.
- Demirjian A, Goldstein H, Tanner JM (1973) A new system of dental age assessment. Hum Biol. 45(2): 211-227.
- Harris EF, Buck A (2002) Tooth mineralization.A technical note on the Moorrees-Fanning-Hunt standards. Dental Anthropology 16(1): 15-20.
- Van der Linden FPGM, Duterloo JS (1976) Development of the human dentition: an atlas. New York: Harper and Row 70(5): 582–583.
- Garn SM, Lewis AB, Kerewsky RS (1964) Sex difference in tooth size. J Dent Res 43(2): 306.
- Jayaraman J, Wong HM, King NM, Roberts GJ (2013) The French-Canadian data set of Demirjian for dental age estimation: a systematic review and meta-analysis. J Forensic Leg Med 20(5): 373-381.
- Yan J, Lou X, Xie L, Yu D, Shen G, et al. (2013) Assessment of dental age of children aged 3.5 to 16.9 years using Demirjian's method: a meta-analysis based on 26 studies. PLoS One 8(12): e84672.
- Smith BH (1991) Standards of human tooth formation and dental age assessment. In: Kelley MA, Larsen SP, editors. Advances in dental anthropology. New York: Wiley-Liss. 143-68.
- Harris EF (2011) Dental age: The effects of estimating different events during mineralization. Dental Anthropology 24(2): 59-63.





