Tuberculosis: Bacteriological And Epidemiological Aspects in The Central Region of Tunisia
Asma Ferjani1*,Manel Marzouk1,Imen Ben Kahla1,Walid Ben Salma1,Nadia Gharbi1,Hasna Tarmiz2, Hechmi Kenani2, Moncef Ben Said3,JalelBoukadida1
1* College of Forest Resources and Environment Nanjing Forestry University, Naniing 210037, P.R. China
2 College of Life Science, Key Lab of Protection and Utilization of Subtropic Plant Resources, Jiangxi Normal University, Nanchang 330022, P.R. China
*Corresponding Author
Asma Ferjani
Laboratory of microbiology and immunology, UR02, SP13,
Universitary Hospital Farhat Hached, Sousse 4000,Tunisia
Tel: 00 216 22604255; Fax: 00 216 22604255
E-mail: asma.ferjani@rns.tn
Article Type: Review Article
Received: May 18, 2013; Accepted: May 29, 2013; Published: May 31, 2013
Citation: Ferjani A, et al (2013). Tuberculosis: Bacteriological And Epidemiological Aspects in The Central Region of Tunisia. Int J Microbiol Adv Immunol. 1(2), 14-18. doi: dx.doi.org/10.19070/2329-9967-130003
Copyright: Ferjani A© 2013 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To present the situation of Tuberculosis (TB) in the region of Sousse.
Materials And Methods: A retrospective study conducted during 4 years (2006-2009) concerning all TB cases in the region of Sousse diagnosed according to bacteriological or histo-pathological and / or clinical criteria.
Results: The total of TB cases is 494. The incidences noted for the period study were respectively 20.7, 20.6, 24.7 and 22.4. The mean age was 39.7 years, the sex ratio was 1.4. Close contact was found in 29.7%. Twenty patients were prisoners. The mean delay for TB diagnosis was 45 days. Symptoms were predominated by cough and fever in pulmonary TB (PTB). HIV infection was noted in only 2 patients with extrapulmonary tuberculosis (EPTB). TB was 233 times pulmonary and 261 times extra pulmonary (31% lymph nodes). Bacteriology confirmed the diagnosis in 207 cases; microscopy was positive in 67.6% (PTB) and 15.9% (EPTB). Multidrug resistance (MDR) was observed for 8 strains / patients. Mortality attributed directly to TB was 0.2%.
Conclusion: TB remains endemic in our region. TB location is primarily lung and lymph nodes. TB is not related to HIV infection. MDR and mortality attributed to TB are rare in our region.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Tuberculosis; Epidemiology; Bacteriology; Sousse.
Introduction
Despite a “vaccine” used for over seventy years and effective antibiotics available for over sixty years, tuberculosis (TB) remains a major global public health problem [1]. However, TB has large variations in the expression of the disease and in its spread in the general population. These variations depend essentially on socio-economic and health status of populations. We describe the situation of TB in the central region of Tunisia, an endemic country of TB, with its different epidemiological and bacteriological characteristics.
Materials and Methods
It is a retrospective study conducted in the coastal region of east-central Tunisia, about 500 000 people with a socio-economic development among the highest in Tunisia and an annual income per capita of 4200 dollars. The national incidence of TB in Tunisia was 20.6 (in 2009) [1]. The study included all TB cases diagnosed between January 1st, 2006 and December 31, 2009 on the basis of biological and / or clinical or histo-pathological criteria.
Patients files collected were: sex, age, origin, marital status, socioeconomic status, clinical characteristics (including past history of TB, diabetes mellitus, malignancies, HIV...), treatment history (use of immunosuppressive drugs, steroids), past history of treatment for TB, smoking habits, history of known contact with a case of TB, stay in closed community (prison), date of hospital admission, hospital department, symptoms brought patient to consult (fever, weight loss, sweats, cough ..), chest radiographs investigations and the delay between the onset of symptoms and TB diagnosis (date of commencing treatment).
The bacteriological study included: the number of samples examined per patient and kind of each one (sputum, bronchial fluid, gastric aspirate, lymph node, pleural effusion...), date of sampling, result of Ziehl.
Neelsen staining (ZNS) (noted depending on the richness of acid fast bacilli (AFB) notified by number of crosses), result of cultures and positivity delay, and susceptibility to the first line agents (rifampicin, isoniazid (INH), streptomycin, ethambutol, and / or pyrazinamide).
The pulmonary samples were inoculated on Löwenstein Jensen (LJ) culture medium. The extra-pulmonary samples were inoculated on solid (LJ and Coletsos) and liquid (BacT/Alert MB; BioMérieux, France) culture media. Culture media were incubated at 37 ° C in an inclined position up to 3 months for solid media and 40 days for liquid media. Cultures on solid medium were examined once a week, those on liquid medium considered to the alarm signal. Bacteria grown on culture media were identified by conventional biochemical techniques [2] and confirmed by the GenoType molecular kits (Hain Lifescience GmbH, Nehren, Germany). Susceptibility to the first line drugs was testing by the technique of proportions (Biorad). Patients with extended disease to organs or tissues outside the thorax, including those patients who had pulmonary involvement, were considered as extra-pulmonary TB (EPTB).
Results
During the study period, a total of 494 cases of active TB patients was registered in our region; with an incidence of 20.77 in 2006, 20.6 in 2007, 24.72 in 2008 and 23.3 in 2009. The mean age of patients was 39.75 years ranging from 6 months to 94 years. The peak age was 20-29 years. The male to female ratio was 1.4. Most patients (60.5%) were from urban areas. Fifty six percent of patients were married and 46.8% were from the ‘casual laborer’ class. Forty six percent of patients were ‘ever smoked’ (those who were either currently smoking or ex-smokers). The proportion of patients who had a history of contact with a known case of TB was about one third of patients (29.7%). Twenty patients were prisoners. Patients were mainly hospitalized in chest diseases department (40.3%) and the remaining in various medical and surgical services. The mean delay between the onset of symptoms and diagnosis of TB (commencement of treatment) was 45 days (ranging from 2 to 240 days) [Figure 1]. TB disease was 233 times pulmonary (PTB) and 261 times extra-pulmonary (EPTB) [Table 1]. Thirty seven patients were suffering from diabetes mellitus. HIV status was only known for 24 out of the 494 patients, among them two were HIV positive and presented with extra-pulmonary localization. Ten patients had a history of treatment with immunosuppressive drugs. In PTB, clinical symptoms were mainly included cough (47.4%), fever (44.6%), asthenia, weight loss and anorexia in 43% cases; whereas in EPTB, signs most frequently found were fever (26%) and asthenia (22%). Chest radiographic findings suggestive of TB were found in all cases of PTB: right apical (29.9%) and bilateral located (27%) lesions were predominant. In EPTB, radiological TB signs were present in 38.6% of cases. TB diagnosis was based on bacteriological examination in 207 cases [Figure 2] and on histopathological examination and/or strong clinical and radiological evidence in 287 cases [Figure 3]. The two hundred seven non-redundant strains of Mycobacterium tuberculosis were isolated mainly from sputum (64.4%) and from lymph nodes (14.6%) [Figure 2]. ZNS positive bacilli were demonstrated in 67.6% and 15.9% of pulmonary and extra-pulmonary samples respectively. The estimated abundance of bacilli was noted at five crosses in 64 of the 140 positive ZNS pulmonary samples and one cross in 26 of the 33 positive ZNS EP samples. The delay of positivity of cultures on solid medium was 2 to 4 weeks (34.7%), 4 to 6weeks (32.6%) and beyond 6 weeks for the remaining cultures (32.7 %). On liquid media, the mean delay of positivity was 10 days. The initial antibiotherapy was based on the INH, rifampicin, pyrazinamide and ethambutol association in 96.2% of cases. Drug susceptibility testing showed acquired resistance to INH in 4 cases, to both streptomycin and INH in 5 cases, and to both streptomycin and rifampicin in one case. Seven cases of acquired multidrug resistance (MDR) were found: a double resistance to INH and rifampicin in 2 cases, a triple resistance to INH, rifampicin and streptomycin in 5 cases, and a primary resistance to the four drugs in one case. Twelve deaths were recorded during our study period. They were subsequent to fulminant hemoptysis in one case, to MDR TB in 3 cases, and to additional co-morbidities in the remaining eight cases.
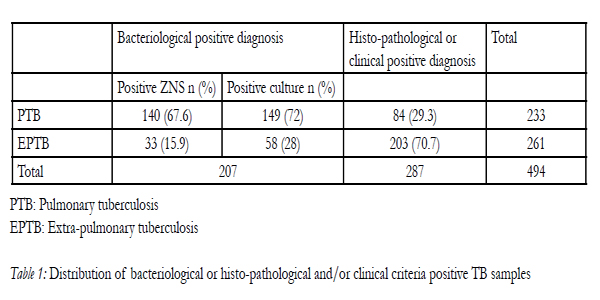

Table 1: Distribution of bacteriological or histo-pathological and/or clinical criteria positive TB samples
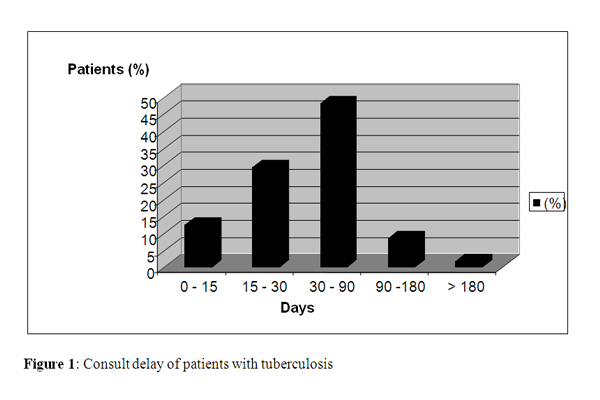
Figure 1: Consult delay of patients with tuberculosis
Discussion
TB remains a major public health problem worldwide [1]. Socio-economic problems and general health deficiencies are the main causes of endemic TB in developing countries. The incidence rate of TB in our region (between 20 and 25) is practically the same as in other parts of Tunisia [3]. Tunisia is ranged in the countries with a moderate TB incidence [3].
among men as compared to women [4-7]. This could be explained by the most prevalence of promiscuity in men, particularly in community meeting places (cafes and tea rooms) much frequented by the males in our society.
TB occurs at any age but mainly affects young adults with important social activity [8, 9]. This adds to the economic loss caused by TB as it affects the working age adults and parents of young children, imposing a work stoppage with major socioeconomic impacts [10, 11]. Some studies, however, reported a higher TB in the oldest segment of the population due to co-morbidities that are risk factors for developing TB and the reactivation of the disease [7, 12].
In our study, TB was found to primarily affect urban communities where promiscuity is the main promoting transmission factor of M. tuberculosis. The urban community meeting places (cafes and tea rooms) are at high risk of airborne transmission of M. tuberculosis. In contrast to previous studies where TB was shown to mostly occur in disadvantaged areas [4, 13].
TB is a common disease in the general population. The exact context of the contamination is rarely found. However, as it was likely the case in about one third of our patients, the transmission may originate from close contact with patient. Closed communities (prisons) are classical context that promote occurrence of TB, for obvious reasons related to incarceration [14]. Twenty of our patients acquired TB during their stay in prison.The ‘casual labourers’ class is most affected by TB. This is related to the lifestyle of these workers, who spend most of their free time in cafes, and are very prevalent in our country. Promiscuity in these relatively confined areas is very favourable to inhalation Pflügge particles
Smoking habits found in almost half of TB cases, have been implicated as a risk factor predisposing to TB. A causal relationship between smoking and development, recurrence of TB and mortality due to smoking was demonstrated [15, 16].
The period between the onset of symptoms and the commencement of treatment should be as shorter as possible to prevent the transmission of TB to contacts. Adopting the definition proposed by the panel of experts, the ‘acceptable’ period to receive treatment is 0-30 days [17]. The mean period is 45 days for our patients; it ranges from a few weeks to several months in other studies [17-19]. This relatively long period in our patients obviously needs to be shortened in order to prevent transmission to healthy individuals.
Additional risk factors for developing active TB include immuno-deficiency due to drugs or disease; HIV infection being the leading one in Western countries [5, 20], in contrast to our country where HIV positivity is not associated with TB. Indeed, TB is not considered in Tunisia as an opportunistic disease and knowledge of HIV status of TB patient is not needed.
TB can be clinically confusing because of the poor specificity of symptoms. Cough is the most common symptom of PTB [21, 22]. Undetected PTB in patients, where cough is attributed to other co-morbidities, may be a potent source of TB infection, especially for the close contacts [23]. In EPTB, symptoms mainly consist of alteration of general condition and a slight nocturnal fever [21].
Chest radiographs usually support the diagnosis of TB, especially in pulmonary localization [21, 24]. However, its contribution in extrapulmonary forms is poor, mainly in cases with negative microscopy.
TB can develop anywhere in the body. Nevertheless, the most common site remains the lungs [8, 25]. In the last decades, an increase of the lymph node TB was noted in many countries [8, 25, 26].
The diagnosis of TB is based on bacteriology. The histology is contributory in the EPTB cases with a negative ZNS [27]. The development of rapid diagnosis mycobacterial tests would further improve diagnosis of EPTB [28, 29]. Bacteriology is very effective in PTB [30]. Microscopy was positive in most of our patients with pulmonary localization. Culture on solid medium remains the “gold standard”, whatever the location of TB [2].
The amount of biological samples addressed to our lab for TB diagnosis doesn’t reflect the actual distribution of TB cases. Indeed, the bacteriology lab does not receive all the biological samples. This is due to the fact that clinicians are not fully aware of technical developments and new tests now available which improve the diagnosis of TB in lymph nodes and other solid biological samples (Stomacher mill and disperse).
In EPTB, although conventional bacteriology provides less positive immediate result, it remains essential for diagnosis and treatment of patients. Our bacteriological positivity rates in EPTB are similar to those reported by other authors [30].
AFB, which is a marker of contagiousness of the disease, was present in more than half of patients with PTB. Specificity of microscopy is very high [30]. The presence of AFB in pulmonary sample indicates that the patient is suffering from bacillary active and contagious TB. Other techniques have been evaluated in order to improve and accelerate diagnosis and treatment of TB [28, 29].
The management of TB cases has recently been complicated by the emergence of drug-resistant TB strains (MDR). Acquired resistance is almost always caused by inadequate treatment and non adherence to treatment [31, 32]. The rate of resistance noted in our study did not reach the alarming rates reported in other studies [33, 34]. In our region, rigorous TB control treatment measures have been implementing which consist of the direct observed therapy (DOT) programmes and a mobile health monitoring team. The rates of resistant TB strains in our region, although higher than those reported in Western countries [34], are below the overall rate reported by the world health organisation (WHO) in 2008 and in some countries [34, 35]. However, the rate of resistance we noted is mainly of the acquired type and should prompt our health authorities to be more vigilant and effective.
Nowadays, the mortality directly attributed to TB is rare, in well functioning TB management programs. In our study, the mortality is very low (0.2%), much lower than the rates of mortality due to TB reported by WHO in 2009 and in some countries [1, 35].
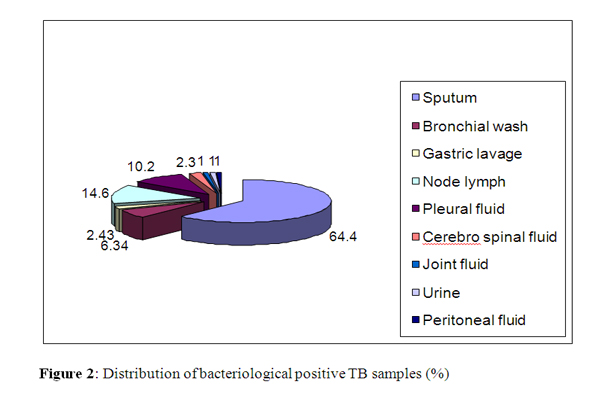
Figure 2: Distribution of bacteriological positive TB samples (%)
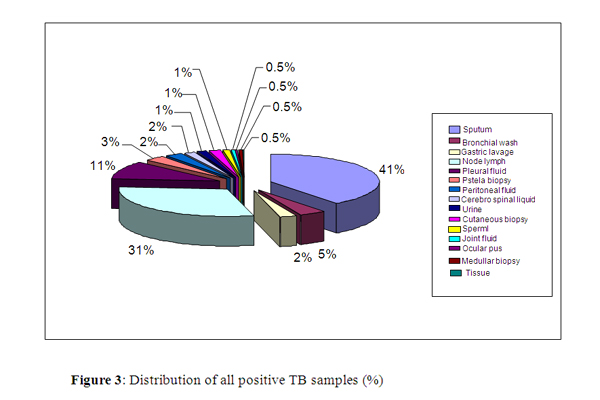
Figure 3: Distribution of all positive TB samples (%)
Conclusion
TB remains endemic in our region with an incidence between 20 and 25. It is mainly lung and lymph node, not related to HIV infection. Resistance to anti-TB is rare, and mortality directly attributed to TB is a rare event. The new medical techniques in mycobacteriology are very promising for better management of TB patients in the near future.
Acknowledgements
This work was realised in UR02SP13 activity financed by the MESRS. TN .
References
- World Health Organisation (WHO): Global tuberculosis control, WHO report 2009. (WHO/HTM/TB/2009.411). [http://www.who.int/gtb/publications].
- Mohr O’hara C, Weinsteine M.P, Miller M (2003) Manual and automated systems for detection and identification of microorganisms.In Manual of clinical microbiology 8th edition volume 1. Eds: Murray P.R, Baron E.J, Jorgensen J.H, Pfaller M.A, Yolken R.H. Washington, DC 20036-2904 pp: 185-207.
- Ministry of Public Health. Bulletin de la direction des soins de santé de base : programme national de lutte antituberculeuse. Ministry of Public Health, Tunisia; 2007.
- Enarson DA, Wang JS, Dirks JM. The incidence of active tuberculosis in a large urban area. Am J Epidemiol 1989; 129: 1268-1276.
- Long R, Njoo H, Hershfield E. Tuberculosis: 3. Epidemiology of the disease in Canada. Canadian Medical Association 1999; 160 (8): 1185-90.
- Decludt B. Epidémiologie de la tuberculose. Mycobacterium tuberculosis et mycobactéries atypiques In : Guides Médi/Bio. François Denis, Christian Perronne. Elsevier, 2004 : pp : 5-19.
- Pesut DP, Gledovic ZB, Grgurevic AD, Nagroni-Obradovic LM, Adzic TN. Tuberculosis incidence in elderly in Serbia: Key trends in socioeconomic transition. Croat Med J 2008; 49:807-812.
- Mtiraoui A, Soltani M, Ghannem H et al. Epidémiologie de la tuberculose dans le Sahel Tunisien. Med Mal Infect 1998 ; 28 : 199-202.
- Tocque K, Bellis MA, Tam CM et al. Long-term trends in tuberculosis. Comparison of age-cohort data between Hong Kong and England and Wales. Am J Respir Crit Care Med 1998; 158: 484-488.
- Tapiero BF, Lamarre V. Tuberculosis in Canada: Global view and new challenges. Paediatr Child Health 2003; 8: 139-140.
- Boulahbal F, Chaulet P. La tuberculose en Afrique. Med Trop 2004; 64 : 224-228.
- Davies PD. TB in the elderly industrialised countries. Int J Tuberc Lung Dis 2007; 11: 1157-1159.
- Salihu H.M, Naik E, O’Brien W, Dagne G, Ratad R, Mason T. Tuberculosis in North Carolina: Trends Across two decades, 1980-1999. Emerg Infect Dis 2001;7 (3): 570-574.
- Burman WJ, Cohn DL, Rietmeijer CA, Judson FN, Sbarbaro JA, Reves RR. Short-term incarceration for the management of noncompliance with tuberculosis treatment. Chest 1997; 112:57-62.
- International union against tuberculosis and lung diseases. Promotion de la santé respiratoire dans les pays à faible et moyen revenu. Programmes anti tabac de l’union 2007. www.tobaccofreeunion.org.
- Sreeramareddy CT, Panduru KV, Verma SC, Joshi HS, Bates MN. Comparison of pulmonary and extrapulmonary tuberculosis in Nepal-a hospital-based retrospective study. BMC Infectious Diseases 2008; 8: 1-7.
- Pirkis JE, Speed BR, Yung AP, Dunt DR, MacIntyre CR, Plant AJ. Time to initiation of anti-tuberculosis treatment. Tuberc Lung Dis 1996; 77: 401-406.
- Lawn S D, Afful B, Acheampong J W. Tuberculose pulmonaire : délai de diagnostic chez les Ghanéens adultes. Int J Tuberc Lung Dis 1998; 2 (8): 635-640.
- Beyers N, Gie RP, Schaaf HS et al. Delay in the diagnosis, notification and initiation of treatment and compliance in children with tuberculosis. Tuberc Lung Dis 1994 ; 75 : 260-265.
- Selwyn PA, Hartel D, Lewis VA et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med 1989; 320:545-550.
- Billy C, Perronne C. Infections dues aux mycobactéries tuberculeuses chez l’adulte. Mycobacterium tuberculosis et mycobactéries atypiques In : Guides Médi/Bio. François Denis, Christian Perronne. Elsevier, 2004 : pp 47-63.
- Wejse C, Gustafson P, Nielsen J et al. TBscore: signs and symptoms from tuberculosis patients in a low-resource setting have predictive value and may be used to assess clinical course. Scand J Infect Dis 2008;40:111-120.
- Veen J. Microepidemics of tuberculosis: the stone-in-the-pond principle. Tuberc Lung Dis 1992; 73:73-76.
- Thumerelle C, Pouessel G, Errera S et al. Imagerie de la tuberculose pulmonaire. Arch Ped 2005; 12 : S132-S136.
- Te Beek LA, Van Der Werf MJ, Richter C, Borgdoff MW. Extra pulmonary tuberculosis by nationality, the Netherlands, 1993-2001. Emerg Infect Dis 2006; 12:1375-1382.
- Ralisata LR, Rabenjamina FR, Ralison A. Les formes extrathoraciques de la tuberculose en milieu hospitalier à Mahajanga (Madagascar). Arch Inst Pasteur Madagascar 2000 ; 66 : 13-17.
- Ulrichs T, Lefmann M, Reich M et al. Modified immunohistological staining allows detection of Ziehl-Neelsen-negative Mycobacteriumtuberculosis organisms and their precise localization in human tissue. J Pathol 2005; 205(5):633-640.
- Ben-Selma W, Ben-Kahla I, Marzouk M et al. Rapid detection of Mycobacterium tuberculosis in sputum by Patho-TB kit in comparison with direct microscopy and culture. Diagn Microbiol Infect Dis 2009; 65:232-235.
- Ben Kahla I, Ben Selma W, Marzouk M, Ferjeni A, Ghezal S, Boukadida J. Evaluation of a simplified IS6110 PCR for the rapid diagnosis of Mycobacterium tuberculosis in an area with high tuberculosis incidence. 10.1016/j.patbio.2009.04.001
- Martin C, Vincent V, Denis F. Diagnostic bactériologique des infections à mycobactéries. Mycobacterium tuberculosis et mycobactériesatypiques In : Guides Médi/Bio. François Denis, Christian Perronne. Elsevier, 2004 : pp 139-189.
- Chan ED, Iseman MD. Current medical treatment for tuberculosis. BMJ 2002; 325: 1282-1286.
- Sbarbaro JA, Sbarbaro JB. Compliance and supervision of chemotherapy of tuberculosis. Sem Respir Infect 1994; 9:120-127.
- Blower SM, Chou T. Modeling the emergence of the “hotzones”: tuberculosis and the amplification dynamics of drug resistance.Nat Med 2004; 10:1111–1116.
- Zignol M, Hosseini MS, Wright A et al.Global Incidence of Multidrug-Resistant Tuberculosis. Stop TB Department, World Health Organization, Geneva, Switzerland 2008.
- Calver AD, Falmer AA, Murray M et al. Emergence of increased bresistance and extensively drug-resistance tuberculosis despite treatment adherence, South Africa. Emerg Infect Dis 2010; 16: 264-271.





