Prevalence, Antibiotic Susceptibility Pattern and Demographic Factors Related to Methicillin Resistant Staphylococcus aureus in Lahore, Pakistan
Hassan A K1, Mohammad M2, Humera K2, Samina N2, Ahmed A K1, Fridoon J A3, Riffat M3,4*
1 Institute of Molecular Biology and Biotechnology, University of Lahore, Pakistan.
2 Department of Pathology, King Edward Medical University, Lahore, Pakistan.
3 Department of Biomedical Sciences, King Edward Medical University, Lahore, Pakistan.
4 Present address: SISSA, International School for Advanced Studies, Trieste, Italy.
*Corresponding Author
Riffat M,
Assistant Professor,
Biomedical Sciences, King Edward Medical University,
Lahore, Pakistan.
E-mail: mehboob.riffat@gmail.com
Article Type: Research Article
Received: May 30, 2014; Accepted: June 20, 2014; Research Article June 23, 2014
Citation: Riffat M et al., (2014) Prevalence, Antibiotic Susceptibility Pattern and Demographic Factors Related to Methicillin Resistant Staphylococcus aureus in Lahore, Pakistan. Int J Microbiol Adv Immunol. 2(3), 45-48. doi: dx.doi.org/10.19070/2329-9967-140008
Copyright: Riffat M© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Methicillin Resistant Staphylococcus aureus (MRSA) is important nosocomial pathogen which has elevated morbidity and mortality rates.
Objectives: The aim of our study was to find out the present scenario of prevalence, antibiotic susceptibility pattern and the demographic factors such as age and gender related to MRSA in different wards of tertiary hospital.
Methods: Staphylococcus aureus was isolated from fifty one clinical specimens at Mayo hospital, Lahore and were subjected to in vitro sensitivity against various antimicrobials by using Kirby Bauer disc diffusion method.
Results: Out of total S. aureus isolated 55% were found to be resistant with methicillin/oxacillin. Most of the MRSA specimens were also found to be susceptible to vancomycin, whereas most were found resistant to ampicillin. Majority of MRSA were isolated from blood samples (31%) followed by pus samples (28%). Most MRSA isolates were seen in the patients admitted in medical wards (32%) followed by dermatology (18%).
Conclusions: Vancomycin is losing its effectiveness against methicillin resistant strains of S. aureus, as one vancomycin resistant sample was also isolated during the study. Prevalence of MRSA found elevated which was evident as more prevalent in males as compare to females, and 30-39 years age group was found to be more affected. Medical ward had most of the MRSA patients followed by dermatology. Improved diagnostic techniques can produce better results by promoting targeted therapy. Laws should be devised which will keep a check on the antibiotic prescriptions made by doctors.
2.Introduction
3.Material and Methods
4.Results
5.Discussion
6.Conclusion
9.References
keywords
MRSA; Prevalence; Demography; Lahore; Pakistan.
Introduction
Staphylococcus aureus belongs to the genus Staphylococcus having forty species of pathogenic organisms [1]. S. aureus is about 25-50% as component of normal microbiota of a Healthy individual [2].This pathogen is associated with broad array of pyogenic, health care-associated (HA), community acquired (CA); acute and chronic, superficial and deep skin infections, which leads to lifethreatening systemic infections. Pathogen cause diseases related to toxins with cuticular indications [3].It is still one of the five most common causes of hospital acquired infections and is often the cause of post surgical wound infections [4]. About 0.5 million staphylococcal infective individuals are admitted in American hospitals each year [5]. The death rate due to Methicillin Resistant Staphylococcus aureus (MRSA) infections are more than HIV/ AIDS in USA. In Canada, 49% were infected with MRSA out of which 51% are colonized, 59% of MRSA infections are of skin and soft tissue infections, while 57% were classified as community acquired till 2009 [6].
Resistant bacteria emerged which are not influenced by methicillin and related antibiotics. All MRSA are descendents of single ancestral S.aureus strain that got mecA [7] but recent advancement represent that some MRSA are divergent that transfer mecA between S.aureus lineages [8]. The striking phenomenon of MRSA is that high incidence levels, acquired in healthcare facilities or during healthcare procedures and low literacy regarding resistance of antibiotics in general public are alarming [9].
The objectives of our study were to determine the prevalence of S.aureus in tertiary care hospital of Lahore, Pakistan along with demographic factors and antibiotic susceptibility of these clinical isolates. This was done by using Kirby Bauer disc diffusion method.
Material and Methods
This study was carried out in the Microbiology lab, Department of Pathology, King Edward Medical University, Lahore. The routine microbiology specimens were taken from Mayo Hospital, Lahore, Pakistan. These specimens were processed within 2 hours of collection by standard microbiology techniques. The agars used for inoculation of samples were blood agar, MacConkey agar and chocolate agar. The plates were incubated in aerobic environment at 35°C for 24 hours. On the basis of colony morphology, Gram staining, catalase and coagulase tests, S. aureus were identified. Kirby-Bauer technique was used for antibiotic susceptibility testing and results were recorded according to Clinical Laboratory Standards Institute-CLSI Guideline (2007). Antibiotic susceptibility testing was performed for oxacillin, ampiclox, fusideem, linezolid, vancomycin and ampicillin. For antibiotic susceptibility testing of oxacillin disc (1µg) the zone size of ≤ 10mm was considered resistant; a zone size of 11-12mm was considered intermediate and zone size of ≥13mm was considered susceptible.
Results
A total of 51 samples were collected from different wards of Mayo Hospital consisting of different types of specimens such as pus, blood, nasal swab, sputum, wound swab, catheter tip, bed sore secretions, fluids, tissue exudates and throat swab. Staphylococcus aureus showed positive results for catalase and coagulase test whereas negative results were observed for oxidase test. A total of 28 MRSA were isolated during the study period. So, the prevalence of MRSA was recorded as 55%. Remaining 23 MSSA constitute 45% of samples (Figure 1).
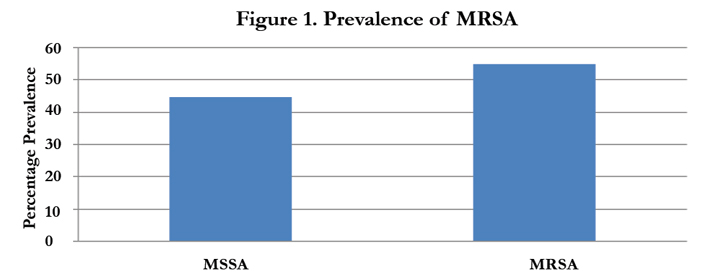
Figure 1. Prevalence of MRSA
Kirby Buyer method was used to check the antibiotic susceptibility pattern of clinical isolates. Two isolates (4%) were sensitive to ampicillin (Figure 2), whereas 98% of isolates were sensitive to vancomycin and 90% were sensitive to linezolid. Only 67%, 45% and 51% of the isolates were susceptible to fusideem, oxacillin and ampiclox respectively.

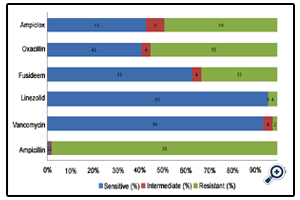
Figure 2. Drug resistance patterns of MRSA isolated from clinical specimens
Specimens that were taken during our study include pus, sputum, wound swab, catheter tip, blood, bed sore secretions, fluids (pleural and ascetic), tissue exudates and throat swab. Majority of MRSA were isolated from blood samples (31%) followed by pus samples (28%) (Figure 3). Gender wise distribution of MRSA found to be 79% in males and 21% in females (Figure 4).
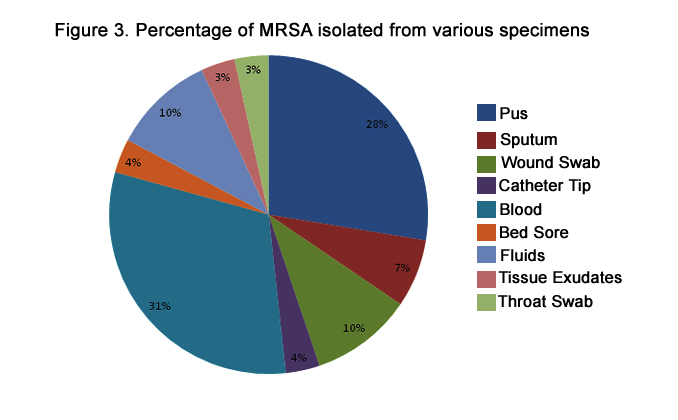
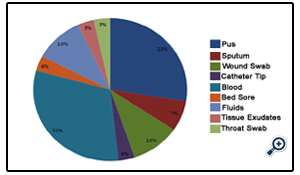
Figure 3. Percentage of MRSA isolated from various specimens
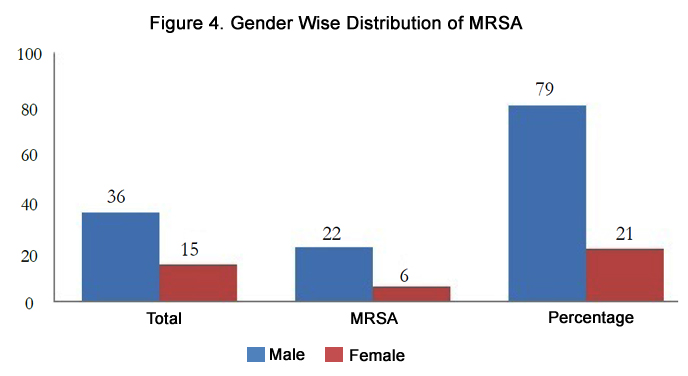
Figure 4. Gender Wise Distribution of MRSA
Prevalence of MRSA in different age groups was recorded in the study, which was highest among 30-39 years age group (39%) followed by 18-29 years age group (21%) (Figure 5). Most MRSA isolates were seen in the patients admitted in medical wards (32%) followed by dermatology (18%) (Figure 6).
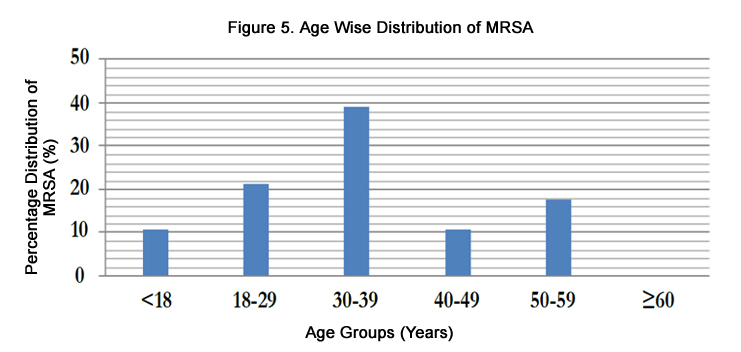
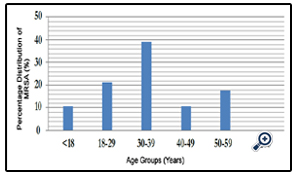
Figure 5. Age Wise Distribution of MRSA
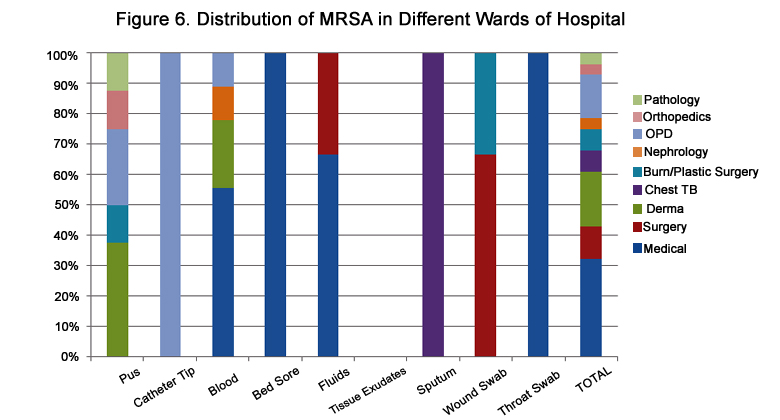
Figure 6. Distribution of MRSA in Different Wards of Hospital
Discussion
n the last decade, the prevalence of MRSA was found elevated at an alarming ratio not only in developed countries but also in Pakistan. In 1989, first MRSA case was reported in Pakistan and after this there was a gradual increase in its prevalence [10]. Increasing trend of MRSA is reported in big cities of Pakistan. Prevalence of MRSA is reported as 42% on the whole, which varies from 2-61% in Pakistan (Table 1). In Lahore, highest prevalence (61%) was reported in 2002 [11]. In our study, prevalence of MRSA is reported as 55% (Figure 1).
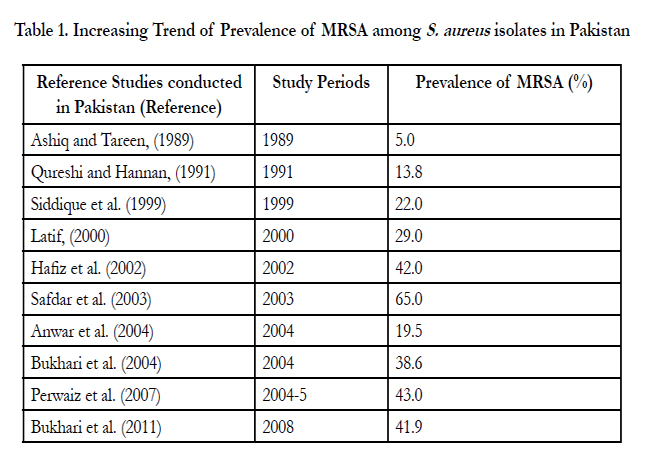

Table 1. Increasing Trend of Prevalence of MRSA among S. aureus isolates in Pakistan
The study that was conducted in the last 11 years showed that MRSA is still sensitive to vancomycin [11,12,13]. But, our study reported one MRSA isolate that was resistant to vancomycin also. The MRSA of clinical isolates showed a maximum of 96% resistance to ampicillin, 55% percent resistance to oxacillin followed by ampiclox (49%), fusideem (33%), linezolid (4%), and vancomycin (2%) (Figure 2).
In previous studies most MRSA were found in the pus samples (58%) [12]. In accordance of our findings, blood shows maximum percentage of MRSA (31%) followed by pus (28%) followed by 10% in fluids and wound swab, sputum (7%), 4% for catheter tip and bed sore secretions and the lowest 3% for tissue exudates and throat swab (Figure 3). Gender wise distribution shows similar results to the study conducted in 2006 in Saudi Arabia [14]. Males showed elevated MRSA distribution of 79% followed by females (21%) (Figure 4).
Different age groups showed different MRSA distribution. Age group of 30-39 years showed maximum prevalence of MRSA (39%) followed by 21% of 18-29 years, 11% for each <18 years and 40-49 years, while ≥60 years showed no MRSA (Figure 5).
Different samples were collected from different wards/departments to check out the percentage prevalence of MRSA. The wards from where the samples were collected included medical, surgery, dermatology, chest TB, burn/plastic surgery, nephrology, OPD, orthopedics and pathology. Highest prevalence was seen in medical ward (32%) followed by dermatology (17%), OPD (14%), surgery (11%), 7% each for chest TB and burn/plastic surgery,4% each for nephrology, orthopedics and pathology (Figure 6).
Emergence of MRSA is due to prolonged hospital stay, frequent use of antibiotics, self-medication and lack of awareness. The study of prevalence of MRSA will not only provide the current antimicrobial situation but also help to devise the appropriate treatment of these infections. Hospitals are also contributing to a great extent in spreading antibiotic resistance elevating MRSA [12].
Conclusion
There is an increase in the prevalence of Methicillin Resistant Staphylococcus aureus. Antibiotic Susceptibility results show that the frequent use of vancomycin for treatment of MRSA is making it resistant. This can produce vancomycin resistant strains of Staphylococcus aureus (VRSA). MRSA showed highest distribution in medical ward as it is a nosocomial pathogen and patients usually acquire it during hospital stay. The treatment of MRSA can become a challenge in the near future. Overuse and misuse of antibiotics along with self-medication should be avoided. Improved diagnostic techniques can produce better results by promoting targeted therapy. Laws should be devised that will keep a check on the prescriptions made by doctors.
References
- Tomasz Hauschild SS (2008) Identification of Staphylococcus spp. by PCR -Restriction Fragment Length Polymorphism Analysis of dnaJ Gene. J. Clin. Microbiol 46(12):3875–3879.
- Lowy FD (2010) Staphylococcal Infections. In: Harrison’s infectious Diseases (Dennis Kasper, Anthony Fauci). McGraw-Hill Professional 1:384
- Becker K, Sunderkötter C (2012) Skin infections with MRSA. Epidemiology and clinical features. The dermatologist, magazine of dermatology, venereology and transform areas 63(5):371-380.
- Poonam Sood Loomba JT, Bibhabati M, Methicillin (2012) Vancomycin Resistant S. aureus in Hospitalized Patients. J. Glob. Infect. Dis 2(3):275–283.
- M SB Fraunholz (2012) Intracellular Staphylococcus aureus, Live-in and let die. Front Cell Infect Microbiol 2:43.
- Matlow A FS, Pelude L, Embree J, Gravel D, Langley JM, et al (2012) Methecilin. Pediatr. Infect. Dis. J 31(8):814-820.
- Kreiswirth B, Kornblum J, Arbeit RD, Eisner W, Maslow JN, et al (2012) Evidence for a clonal origin of methicillin resistance in Staphylococcus aureus. J. sci 259(5092):227-230.
- Musser J, Kapur V (1992) Clonal analysis of Methicillin resistant Staphylococcus aureus strains from intercontinental sources: association of the mec gene with divergent phylogenetic lineages implies dissemination by horizontal transfer and recombination. J. Clin. Microbiol 30(8):2058-2063.
- Rohde R, Ross-Gordon J (2012) MRSA model of learning and adaptation: a qualitative study among the general public. BMC. Hlth. Serv. Res 12: 88.
- Ashiq B TA (1989) Methicillin resistant Staphylococcus aureus in a teaching hospital of Karachi-a laboratory study. J. Pak. Med. Assoc 39:6–9.
- Hafiz S HA, Ali L, Chughtai AS (2002) Methicillin resistant Staphylococcus aureus: A multicentre study. J. Pak. Med. Assoc 52:312–515.
- . Kaleem F UJ, Hassan A, Omair M, Khalid A, Roz Uddin (2010) Sensitivity pattern of methicillin resistant Staphylococcus aureus isolated from patients admitted in a tertiary care hospital of Pakistan. Indian J. of Microbiol 2:141-143.
- . Bukhari MH IA, Khatoon NA (2012) Laboratory study of susceptibility of methicillin-resistant Staphylococcus aureus (MRSA). Pak. J. Med. Sci 20:229–233.
- Manal M B (2006)Trends in antibiotic susceptibility patterns and epidemiology of MRSA isolates from several hospitals in Riyadh, Saudi Arabia. Annals of Clin. Microbiol. and Antimicrobiol 5:30





