Molecular Detection of blaTEM and blaSHF in Diarrhoegenic Escherichia coli Isolated from Egyptian Children
Maysaa El SZ1*, Elewa A1, Mansour AK2
1 Professor, Clinical Pathology Department, Mansoura University, Egypt.
2 Faculty of Medicine, Pediatric Department, Mansoura University, Egypt.
*Corresponding Author
Dr Maysaa El Sayed Zaki,
Professor, Clinical Pathology Department,
Mansoura University, Egypt.
E-Mail: may_s65@hotmail.com
Article Type: Review Article
Recieved: April 08, 2015; Accepted: May 18, 2015; Published: May 19, 2015
Citation: Maysaa El SZ, Elewa A, Mansour AK (2015). Molecular Detection of blaTEM and blaSHF in Diarrhoegenic Escherichia coli Isolated from Egyptian Children. Int J Microbiol Adv Immunol. 03(1), 49-54. doi: dx.doi.org/10.19070/2329-9967-150009.
Copyright: Maysaa El SZ© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Escherichia coli (E.coli) is a common bacterial pathogen for acute diarrhea in children. The aim of the present study was to determine the prevalence mainly of TEM and SHV-beta lactamase-encoding genes responsible for extended spectrum beta lactamase (ESBL) production amongst diarrheagenic E. coli species as these strains are reported to have been increased in recent years.
Methodology: The study included children with acute diarrhea presented in Mansoura University children hospital during the period from January 2011 till Jun 2014. In the microbiological laboratory stool samples were cultured and the isolated colonies were identified by standard biochemical reactions and by multiplex polymerase chain reaction (PCR) for identification of diarrheagenic E.coli strains. In vitro susceptibility testing of all isolates was performed using the discs diffusion method. E.coli isolates were subjected to testing to detect the possible presence of SHV, and TEM genes by conventional PCR.
Results and Conclusion: The study included 600 children presented as acute diarrhea. Acute diarrhea caused by E.coli was detected in 160 samples. ESBL genes either TEM or SHF was detected in 31.1% of isolated E.coli. The commonest gene was TEM (22.5%), then SHF (10%). Combined genes were detected only in 2 isolates, table 6.
The commonest resistance pattern of E.coli harboring ESBL genes cefepime (100%), cefazolin (96%) and cefotaxime (96%) and for non beta lactams the commonest was for ciprofloxacin (88%), amikacin and tobramycin (20% for each), Table7.
From this study we can conclude that extended beta lactamase production is common among diarrheagenic Escherichia coli isolated from children below 5 years. The bla-TEM is the common genetic mechanism for extended beta lactamase production in these isolates followed by bla-SHF.
2.Introduction
3.Material and Methods
3.1 DNA Extraction
3.2 Multiplex PCR for identification of Diarrheagenic E.coli species
3.3 Antimicrobial susceptibility testing and ESBL detection
3.4.PCR for the detection of TEM and SHV genes
4.Results
5.Discussion
6.References
keywords
Diarrheagenic E.coli; ESBLs; bla TEM; bla SHF.
Introduction
Acute infectious diarrhea is an important cause of morbidity and mortality in children worldwide. The disease remains a health problem challenge especially in developing countries [1-3]. The causative pathogens include a wide variety of microorganisms like bacteria, viruses and parasites. [4-7]. Diarrheagenic Escherichia coli; (E.coli) represented one of the most frequent causes of acute diarrhea in children under five years old in developing countries [8-10]. In UNICEF report in Egypt based on survey conducted by Egypt demographic and health state the overall percentage of children under five who had diarrhoea in survey was conducted was 8.5%. and though antibiotics and anti-diarrhoeal medications are generally not recommended to treat diarrhoea in young children; results from the survey reported that antibiotics were given to one-third of children with diarrhea [11].
Recent reports indicated increase in the prevalence of extended beta lactamase production among diarrheagenic E.coli species [12, 13]. The inappropriate use of antibiotics is one of the leading causes of acquisition of microbial resistance leading to severe infections. Moreover, E.coli is known to be an important reservoir for resistance genes as described previously in several reports [14, 15].
A common mechanism of antibiotics resistance in E.coli is the production of extended beta lactamase enzymes. Beta-lactamases are enzymes produced by some bacteria and are responsible for bacterial resistance to beta-lactam antibiotics like penicillins, cephamycins and carbapenems (ertapenem). These antibiotics have a common four-atom ring known as a beta-lactam in their molecular structure. The beta-lactamase enzyme breaks that ring open, leading to deactivating the molecule's antibacterial properties [16]. At the beginning (ESBL) producing organisms were isolated from outbreaks in Germany, United States and later on reported world wide [17]. ESBL organisms are commonly resistance to cephalosporines antibiotics [18].
The production of extended-spectrum β-lactamases like TEM-1, TEM-2 and SHV-1 by gram-negative bacteria renders these species resistant to penicillins, cephalosporins and aztreonam in the treatment of serious infections caused by these pathogens. Though there is no information on their molecular types [19, 20].
There are so many types of ESBLs like TEM, SHV, CTX, OXA, but majority of the ESBLs are derivatives of TEM or SHV enzymes and these enzymes are most often found in E. coli and K. pneumoniae [21].
There are limited studies about the molecular mechanisms of ESBLs in diarrheagenic E.coli in Egypt related to presence of bla-TEM and bla-SHF genes in diarrheagenic E.coli.
The aim of the present study was to determine the prevalence mainly of bla-TEM and bla-SHV genes common genes responsible for ESBL production amongst diarrheagenic E.coli species isolated from the children admitted to Mansoura University children hospital.
Material and Methods
The study included children with acute diarrhea presented in Mansoura University children hospital during the period from January 2011 till Jun 2014. Diarrhea was defined as
(i) at least three loose (or watery) stools within 24 h, regardless of other gastrointestinal symptoms;
(ii) two or more loose stools associated with one other symptom of gastrointestinal infection like abdominal pain, nausea, vomiting, and fever; or (iii) passage of a single loose stool with grossly evident blood and/or mucous [22].
Patients were selected according to the Centers for Disease Control and Prevention (CDC) definition of hospital acquired diarrhea which is acute onset of diarrhea in a hospitalized patient with a period of at least 3 days of hospitalization prior to the onset of diarrhea [23].
The parents of each child signed and the study was approved by the ethical committee of Mansoura Faculty of Medicine, Egypt. Each child was subjected to full history taking and clinical examinations. Stool sample were obtained from each patient and subjected to full microbiological examination.
Stool samples were collected in plastic containers. In the microbiological laboratory, stool samples were spread on MacConkey at 37°C for 24 hours. The isolated colonies were identified by standard biochemical reactions by MicroScan® WalkAway diagnostic microbiology system (Siemens HealthCare Diagnostics, formerly Dade Behring, USA).
E.coli was identified by furthure multiplex PCR to identify the five common diarrheagenic E.coli species namely Enterotoxogenic E.coli (ETEC) Enteroaggregative E.coli (EAEC) Enterohemorrhagic E.coli (EHEC), Enteropathogenic Esch.coli (EPEC) and Enteroinvasive Esch.coli (EIEC).
Ten colonies of isolated E.coli were suspended in 1ml of sterile distilled water and bacterial suspension was boiled for 10 minutes centrifuged and supernantent was used as DNA templates for all PCR procedures.
Multiplex PCR was designed for the detection of target genes: eae for enteropathogenic E.coli (EPEC), eae and stx for enterohemorrhagic E. coli (EHEC), ipaH for enteroinvasive E. coli (EIEC), CVD432, aspU and aggR for enteroaggregative E. coli (EAEC) and elt and est for enterotoxigenic E. coli (ETEC). The primers used and bp size were summarized in Table 1 [24].
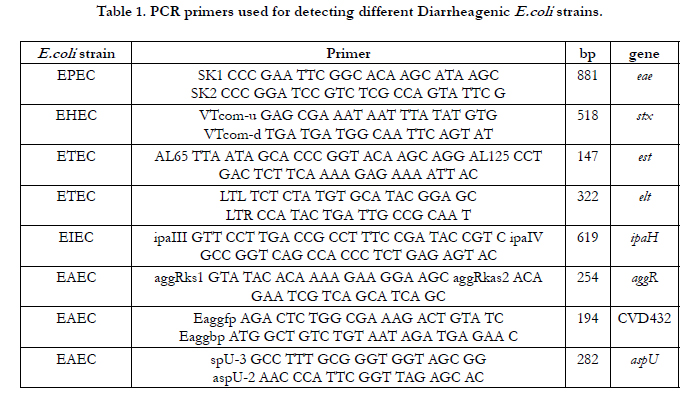

Table 1. PCR primers used for detecting different Diarrheagenic E.coli strains.
A total volume of 50μl master mixture was used for PCR using mixtures of 10x buffer 5μl, dNTP (0.2mM each) 4μl, primer mixture (30 p mol concentration of each) 3μl, Taq polymerase (2.5 U) 0.5μl, DNAase free water 36.5μl and DNA template (sample) 1μl.
Amplification was performed in the thermal cycler at 95ºC (Initialization) 5 minutes, 95ºC (Denaturation) 1 minute, 56ºC (Annealing) 1 minute 30 cycles, 72ºC (Extension) 1 minute 72ºC (Final extension) 10 minutes [24].
In vitro susceptibility testing of all isolates to a wide range of antimicrobials, including both beta-lactams and nn-beta-lactams, was performed using the discs diffusion method. Isolates reported as ESBL positive, were designated as ESBL screen-positive and were further subjected to a confirmatory test. Confirmation of the ESBL phenotype was performed using the combination disk method based on the inhibitory effect of clavulanic acid according to the CLSI criteria [25]. Antimicrobial disks used were obtained from BD BBL Sensi-Disc (Becton Dickinson, Sparks, MD, USA). The antibiotic susceptibility profiles of the isolates were determined to antimicrobials including amikacin 30 mcg, gentamycin 10mcg, ciprofloxacin 5mcg,tobramycin 10mcg, amoxicillin/ clavulanic acid 20/10mcg, cefotaxime 30mcg, ceftazidime 30 mcg, cefepime 30mcg, cefazolin 30mcg and imipenem 10mcgm.
E.coli isolates were subjected to testing to detect the possible presence of bla-SHV, and bla-TEM genes by conventional PCR. The primers used in multiplex PCR are listed in Table 2. A single colony of the isolated bacteria was emulsified in the 50μl reaction mix, which contained 10 pmol of each primer, 10mM dNTPs mix (Qiagen, Hilden, Germany) and 2.5 U of Taq polymerase (Qiagen, Hilden, Germany) in 1x Taq polymerase buffer.
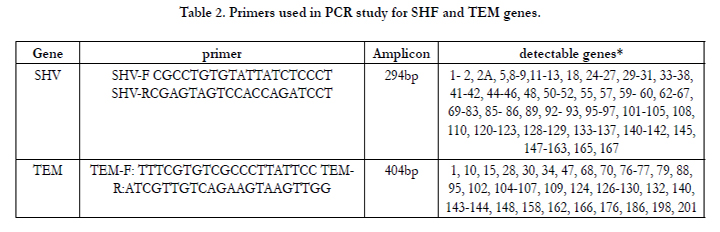
Table 2. Primers used in PCR study for SHF and TEM genes.
Amplification reactions were performed under the following conditions: initial denaturation at 94°C for 5 minutes, followed by 35 cycles of denaturation at 94°C for 30 seconds, annealing at 60°C for 30 seconds with an extension at 72°C for 50 seconds, and a final extension for one cycle at 72°C for 5 minutes. The PCR product was then run on a 1.5% agarose gel stained with ethidium bromide, and visualized under UV transillumination for detection of the amplified fragment.
Results
The study included 600 children who presented with acute diarrhea in the period from January 2011 till Jun 2014. E.coli was detected in 160 samples.
Table 3 summarizes the demographic and clinical data of children with acute diarrhea caused by E.coli. The study included 600 children with mean±SD age 3.3±1.8 years complaining of acute diarrhea during the period of the study. E.coli was isolated for diarrhea from 160 children (26.7%). One hundred patients were non breast feed mainly with hospital acquired diarrhea.
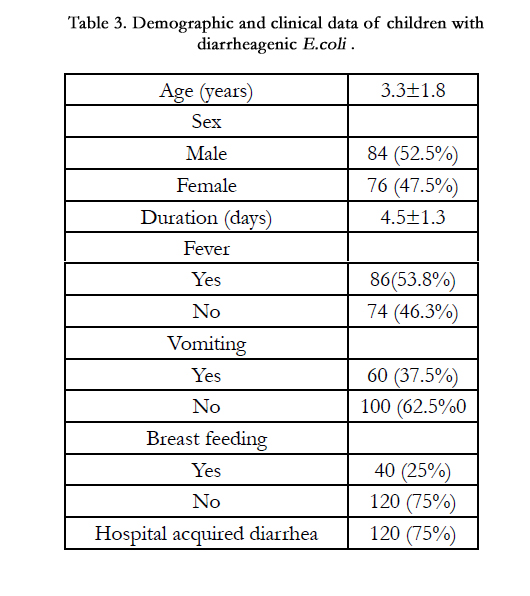
Table 3. Demographic and clinical data of children with diarrheagenic E.coli .
Isolated diarrheagenic species were mainly EAEC (31%) and EPEC (25%) Table 4.
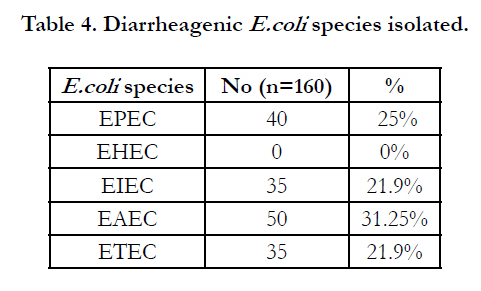
Table 4. Diarrheagenic E.coli species isolated.
The rate of antibiotics susceptibility of isolated E.coli for betalactams antibiotics was for cefepime (96.2%), cefazolin (97.5%), followed by amoxicillin/clavulinic acid acid (28.8%) and imipenem (28.8%). For non beta lactams antibiotics the commonest resistance rate was for ciprofloxacin (90%), Table 5.
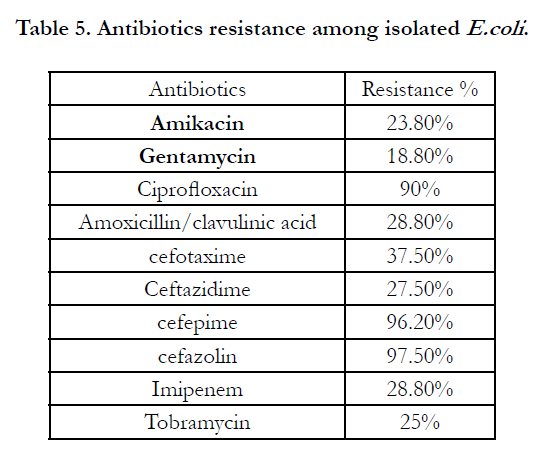
Table 5. Antibiotics resistance among isolated E.coli .
ESBL genes either TEM or SHF were detected in 31.1% of isolated E.coli. The commonest gene was TEM (22.5%), then SHF (10%). Combined genes were detected only in 2 isolates, Table 6.
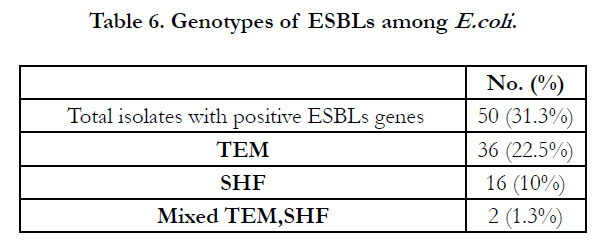
Table 6. Genotypes of ESBLs among E.coli .
The commonest resistance pattern of E.coli harboring ESBL genes cefepime (100%), cefazolin (96%) and cefotaxime (96%) and for non beta lactams the commonest was for ciprofloxacin (88%), amikacin and tobramycin (20% for each), Table7.
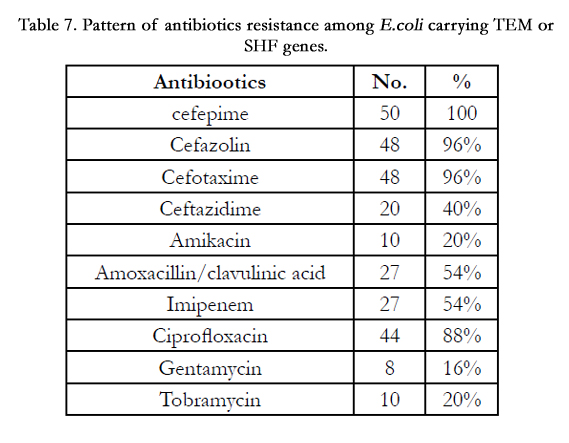
Table 7. Pattern of antibiotics resistance among E.coli carrying TEM or SHF genes.
Discussion
Diarrheagenic E.coli is known as common causative bacteria that cause diarrhea among children world wide [26-28]. Different reports have been investigating the role of E.coli as diarrheogenic cause in different countries. The frequency of isolated E.coli ranged from 30% up t0 40% in previous studies [29, 30]. In Egypt, in limited number of children it was 5.2% Out of 134 patients [31].
In the present study, of the 600 stool samples examined, DEC strains were isolated from (26.7%). of cases mainly under 5 years of age. This finding is online with the concept that diarrheagenic E.coli strains are the most common causes of diarrheal diseases in developing countries [32].
It is well known that E.coli diarrhea has mild course and it is usually self-limited and rehydration is the most effective treatment. The use of antibiotics in general has no role and has many limitations on the grounds of drug toxicity and the risk of increased wide-spread antimicrobial resistance [33, 34].
Isolated diarrheagenic species were mainly EAEC (31%) and EPEC (25%These results on lline to the findings in other study carried in Egypt recently where EAEC was the commonest species [35].
There is increase in antimicrobial resistance due multiple factors one of them is the inappropriate use of antibiotics therapy in developing countries (34). In the present study, the rate of antibiotics susceptibility of isolated E.coli for beta-lactams antibiotics was for cefepime (96.2%), cefazolin (97.5%), followed by amoxicillin/clavulinic acid acid (28.8%) and imipenem (28.8%). This finding has been observed also in an earlier study [36]. In another study, antibiotic resistance rates among Egyptian diarrhoegenic E.coli isolates were 68.2%, 57.2% and 24.2% for ampicillin, trimethoprim-sulfamethoxazole and ampicillin-sulbactam, respectively [37].
Many studies indicate that multidrug resistant E. coli are widespread among the DEC strains and occurrence of resistant DEC could be because of environmental conditions, including transmission of resistant isolates from adults to children, or from animals to humans [38]. The main factors for dissemination of resistance genes are mobilizable plasmids, self-transmissible plasmids and conjugative transposons [39].
The effective ß-lactam/ß-lactamase inhibitor combination was amoxicillin/clavulanic acid combination.The rate of resistance to ß-lactam/ß-lactamase inhibitor in this study was nearly similar to that recorded by Diaz et al. (2010) [40], who reported that 69.4% were susceptible to amoxicillin/clavulanates. Other study reported complete failure of clavulanate to retain the activity of amoxicillin against ESBL-producers derived from Egyptian medical institute [41]. Lower resistance rates (77%) to amoxicillin/clavulanic acid than our finding showed by hospitals and community derived E. coli isolates in medical institute in Cairo, Egypt [42]. This could be explained by the difference in the beta lacatamase types among different studies. It is well known that clavulanate is a potent inhibitor of betalactamase.
The rates of resistance that have been demonstrated by clinical E. coli isolates against the non-ß-lactam antimicrobials was for ciprofloxacin (90%), amikacin and tobramycin (20% for each) reflecting the high resistance rates against the different classes of antimicrobials and the limited therapeutic option for the treatment of the infections that are caused by these E. coli. The rate of resistance against quinolones in this study was similar to that reported previously [41], but greatly higher than that recorded by Mohamed Al-Agamy et al., (41.3%) (2006) [42]. Strong relation between resistance to quinolones and other types of ESBLs like CTX-M-15 production has been documented [43]. The rates of resistance against aminoglycosides, in general, in our study were higher than the previously reported rates [42, 44]. The resistance for both quinolones and ESBL producing E.coli strains may be associated with conjugative transfer of the same plasmids carrying resistance genes for both [45].
The blaTEM and blaSHF was detected in 31.1% from 160 E.coli isolates. The detection rates of ESBLs genes in various studies range from 4% up to 50% according to the geographical region of the isolates [46]. The commonest gene was TEM (22.5%), then SHF (10%). These rates are similar to previous findings in Iran where bla-TEM was reported in 24% of isolated E.coli and 6% was bla SHF and 3% had both genes.
The shortage of this study is the lack of identification of CTX-M genotype that might be responsible for ESBL activity.
From this study we can conclude that extended beta lactamase production is common among diarrhaegenic Escherichia coli isolated from children below 5 years. The bla-TEM is the common genetic mechanism for extended beta lactamase production in these isolates followed by bla-SHF. Antibiotics use should be restricted in diarrhea in children to restrict the spread of antibiotics resistance.
References
- Usein CR, Tatu-Chitoiu D, Ciontea S, Condei M, Damian M (2009) Escherichia coli pathotypes associated with diarrhea in Romanian children younger than 5 years of age. Jpn J Infect Dis. 62(4): 289–93.
- Ochoa TJ, Ruiz J, Molina M, Del Valle LJ, Vargas M, et al., (2009) High frequency of antimicrobial drug resistance of diarrheagenicEscherichia coli in infants in Peru. Am J Trop Med Hyg. 81(2): 296–301.
- Jafari F, Hamidian M, Rezadehbashi M, Doyle M, Salmanzadeh-Ahrabi S, et al.,( 2009) Prevalence and antimicrobial resistanceof diarrheagenic Escherichia coli and Shigella species associatedwith acute diarrhea in Tehran, Iran. Can J Infect Dis Med Microbiol.; 20(3): e56–62.
- Wilson G, Easow JM, Mukhopadhyay C, Shivananda PG (2006) Isolation& antimicrobial susceptibility of Shigella from patients with acute gastroenteritis in Western Nepal. Indian J Med Res.; 123(2): 145–50.
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE, W.H.O (2005) Child Health Epidemiology Reference Group.. WHO estimates of the causes of death in children. Lancet. 365 (9465): 1147–52.
- Niehaus MD, Moore SR, Patrick PD, Derr LL, Lorntz B, Lima AA, et al.,( 2002). Early childhood diarrhea is associated with diminished cognitive function 4 to 7 years later in children in a northeast Brazilian shanty town. Am J Trop Med Hyg. 66(5): 590–3.
- Nguyen TV, Le PV, Le CH, Weintraub A (2005) Antibiotic resistance in diarrheagenic Escherichia coli and Shigella strains isolated from children in Hanoi, Vietnam. Antimicrob Agents Chemother. 49(2): 816–9.
- Yang CM, Lin MF, Lin CH, Huang YT, Hsu CT, Liou ML (2009) Characterizationof antimicrobial resistance patterns and integrons in human fecal Escherichia coli in Taiwan. Jpn J Infect Dis. 62(3): 177–81.
- Vila J, Vargas M, Casals C, Urassa H, Mshinda H, Schellemberg D, et al.( 1999) Antimicrobial resistance of diarrheagenic Escherichia coli isolated from children under the age of 5 years from Ifakara, Tanzania. Antimicrob Agents Chemother. 43(12): 3022–4.
- Mansouri S, Shareifi S (2002) Antimicrobial resistance pattern of Escherichia coli causing urinary tract infections, and that of human fecal flora, in the southeast of Iran. Microb Drug Resist. 8(2): 123–8.
- www.unicef.org/egypt/Child_poverty_and_disparities_in_Egypt_FINAL_-_ENG_full_report_-_23FEB10.pdf
- Khoshvaght H1, Haghi F2, Zeighami H2. Extended spectrum betalactamase producing Enteroaggregative Escherichia coli from young children in Iran. Gastroenterol Hepatol Bed Bench. 2014 Spring;7(2): 131-6.
- Arancibia EM, Pitart C, Ruiz J, Marco F, Gasco´n J, Vila J (2009). Evolution of antimicrobial resistance in enteroaggregative Escherichia coli and enterotoxigenicEscherichia coli causing traveller’s diarrhea. J Antimicrob Chemother. 64: 343–47.
- Pickering LK (2004). Antimicrobial resistance among enteric pathogens. Semin Pediatr Infect Dis. 15(2): 71–7.
- Okeke IN, Aboderin OA, Byarugaba DK, Ojo KK, Opintan JA (2007). Growing problem of multidrug-resistant enteric pathogens in Africa. Emerg Infect Dis. 13(11): 1640–6.
- Bush K, Fisher JF (2011). Epidemiological expansion, structural studies, and clinical challenges of new beta-lactamases from Gram-negative bacteria. Annu. Rev. Microbiol. 65: 455-478.
- Duman M, Abacioglu H, Karaman M, Duman, N Ozkan H (2005) Betalactam antibiotic resistance in aerobic commensal fecal flora of newborns. Pediatr. Int. 47: 267-273.
- Giamarellou H (2005) Multidrug resistance in Gram-negative bacteria that produce extended-spectrum beta-lactamases (ESBLs). Clin Microbiol Infect 11 Suppl 4: 1-16.
- Paul GC, Gerbaud G, Bure A, Philippon AM, Pangon B, Courvalin P (1989) TEM-4, a new plasmid-mediated beta-lactamase that hydrolyzes broad-spectrum cephalosporins in a clinical isolate of Escherichia coli. Antimicrob. Agents Chemother. 33: 1958-1963.
- Marchandin H, Carriere C, Sirot D, Pierre HJ, Darbas H (1999) TEM-24 produced by four different species of Enterobacteriaceae, including Providencia rettgeri, in a single patient. Antimicrob. Agents Chemother. 43: 2069-2073.
- K Ahmad, R Mehdi, A Motahare and M Mitra (2013) Molecular detection of bla TEM and bla SHV genes among clinical isolates of Escherichia coli from Kashan, Iran. African Journal of Microbiology Research, 7(9), 751-754,
- Isenbarger, D. W., B. T. Hien, H. T. Ha, T. T. Ha, L. Bodhidatta, L. W. Pang, and P. D. Cam. (2001) Prospective study of the incidence of diarrhoea and prevalence of bacterial pathogens in a cohort of Vietnamese children along the Red River. Epidemiol. Infect. 127229-236.
- CDC (2009) Gould CV, Umscheid CA, Agarwal RK , Kuntz G,A and Pegues DA, and the Health care Infection control practices Advisory Committee (HICPAC) MMWR :51(16): 1-44.
- Toma, C, Lu, Y, Higa, N, Nakasone, N, Rivas, M and Iwanaga, M 2003 Multiplex PCR Assay for Identification of Human Diarrheagenic Escherichia coli, J Clin Microbiol, 41, (6): 2669.2671.
- Clinical Laboratory Standards Institute (2011) Performance standards for antimicrobial susceptibility testing. 21st informational supplement. CLSI document M100-S18. CLSI: Wayne, PA
- Wilson G, Easow JM, Mukhopadhyay C, Shivananda PG (2006) Isolation& antimicrobial susceptibility of Shigella from patients with acute gastroenteritis in Western Nepal. Indian J Med Res. 123(2): 145–50.
- Maira-Litran T, Allison DG, Gilbert P (2000) Expression of the multipleantibiotic resistance operon (mar) during growth of Escherichia coli as a biofilm. J Appl Microbiol. 88(2): 243–7.
- Jousilahti P, Madkour SM, Lambrechts T, Sherwin E (1997) Diarrhoeal disease morbidity and home treatment practices in Egypt. Public Health. 111(1): 5–10.
- Albert MJ, Faruque SM, Faruque AS, Neogi PK, AnsaruzzamanM, Bhuiyan NA, et al., (1995) Controlled study of Escherichia coli diarrhealinfections in Bangladeshi children. J Clin Microbiol.; 33(4): 973–7.
- Albert MJ, Faruque SM, Faruque AS, Neogi PK, AnsaruzzamanM, Bhuiyan NA, et al., (1995) Controlled study of Escherichia coli diarrhealinfections in Bangladeshi children. J Clin Microbiol. 33(4): 973–7.
- Shehabi AA, Bulos NK, Hajjaj KG (2003) Characterization of diarrhoeagenicEscherichia coli isolates in Jordanian children. Scand J InfectDis. 35(6-7):368–71.
- Davidson, G., G. Barnes, D. Bass, M. Cohen, A. Fasano, O. Fontaine, and S. Guandalini (2002). Infectious diarrhea in children: working group report of the First World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 35(2): S143-S150
- Cheesbrough M (2004) District Laboratory Practice in Tropical Countries. Vol. 2. Cambridge, UK: Cambridge University Press;.
- National Community for Clinical Laboratory Standards (2000) Performance standard for antimicrobial susceptibility testing eleventh informational supplement. Wayne Pennsylvania National Community for Clinical Laboratory Standards, NCCLS Documents M100-S11.
- Ali MM1, Ahmed SF, Klena JD, Mohamed ZK, Moussa TA, Ghenghesh KS. Enteroaggregative Escherichia coli in diarrheic children in Egypt: molecular characterizationand antimicrobial susceptibility. J Infect Dev Ctries. 2014,14 8(5): 589-96. doi: 10.3855/jidc.4077.
- Khalaf, N. G., M. M. Eletreby and N. D. Hanson (2009) Characterization of CTX-M- ESBLs in Enterobacter cloacae, Escherichia coli and Klebsiella pneumoniae clinical isolates from Cairo, Egypt. BMC. Infect. Dis. 9: 84.
- Putnam SD, Riddle MS, Wierzba TF, Pittner BT, Elyazeed RA, El-Gendy A, et al (2004) Antimicrobial susceptibility trends among Escherichiacoli and Shigella spp. isolated from rural Egyptian paediatric populations with diarrhoea between 1995 and 2000. Clin Microbiol Infect. 10(9): 804–10.
- Jafari F, Hamidian M, Rezadehbashi M, Doyle M, Salmanzadeh-Ahrabi S, Derakhshan F, et al (2009) Prevalence and antimicrobial resistance of diarrheagenic Escherichia coli and Shigella species associated with acute diarrhea in Tehran, Iran. Can J Infect Dis Med Microbiol. 20(3): e56–62.
- Brueggemann AB (2006) Antibiotic resistance mechanisms among pediatric respiratory and enteric pathogens: A current update. Pediatr Infect Dis J.25(10): 969–73.
- Diaz, M. A., J. R. Hernandez-Bello, J. Rodriguez-Bano, L. Martinez-Martinez, J. Calvo, J. Blanco and A. Pascual (2010) Diversity of Escherichia coli strains producing extended-spectrum ß-lactamases in Spain: second nationwide study. J. Clin. Microbiol. 48: 2840-2845.
- Fam, N. S and El-Damarawy, M .M (2008) CTX-M-15-extended-spectrum ß-lactamases detected from Intensive Care Unit of an Egyptian Medical Research Institute. Research .J. of Med and Med Sc.3 (1): 84-91.
- Al-Agamy M, El-Din Ashour M. S. and I. Wiegand (2006) First description of CTX-M-ß-lactamase-producing clinical Escherichia coli isolates from Egypt. Int. J. Antimicrob. Agents 27: 545-548.
- Naseer, U and A. Sundsfjord (2011) The CTX-M conundrum: dissemination of plasmids and Escherichia coli clones. Microb. Drug Resist. 17: 83-97.
- Nazik, H., Öngen, B., Yildirim, E.E. and Ermis, F. (2011) High prevalence of CTX-M-type ß-lactamase in Escherichia coli isolates producing extendedspectrum ß-lactamase (ESBL) and displaying antibiotic co-resistance. Afr J of Microb Res 5 (1): 44-49.
- Schaumburg F, Alabi A, Kokou C, Grobusch MP, Köck R, Kaba H et al.. High burden of extended-spectrum beta-lactamase-producing Enterobacteriaceae in Gabon. J Antimicrob Chemother. 2013; 68(9): 2140-3.
- Paterson DL, Bonomo RA (2005) Extended-spectrum beta-lactamases: a clinical update. Clin. Microbiol. Rev. 18: 657-686.





