Acute Patellar Tendon Rupture with Tibial Tubercle Avulsion Repair using Suture Anchors: Tiny Avulsed Fragment which Affects the Strength of Construction - A Case Report
Andri Maruli Tua Lubis1*, Ido Prabowo1
Department of Orthopaedics and Traumatology, dr. Cipto Mangunkusumo General Hospital, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia.
*Corresponding Author
Andri Maruli Tua Lubis,
Department of Orthopaedics and Traumatology, dr. Cipto Mangunkusumo General Hospital, Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia.
Tel: +62 8161177078
Email: andrilubisresearch@gmail.com
Received: March 17, 2022; Accepted: April 06, 2022; Published: April 07, 2022
Citation: Andri Maruli Tua Lubis, Ido Prabowo. Acute Patellar Tendon Rupture with Tibial Tubercle Avulsion Repair using Suture Anchors: Tiny Avulsed Fragment which Affects the Strength of Construction - A Case Report. Int J Surg Res. 2022;8(2):161-164. doi: dx.doi.org/10.19070/2379-156X-2200035
Copyright: Andri Maruli Tua Lubis© 2022. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Patellar tendon is one of the most important component of the knee extensor mechanism, which consisted of
quadriceps femoris muscle, quadriceps tendon, patellar bone and patellar tendon. The total disruption of patellar tendon will
lead to disability and significant morbidity of the patient, or even worse, the patient disable to walk.
Case Presentation: We presented a case of 14-year-old male with acute patellar tendon rupture accompanied by tibial tubercle
avulsion after injury during basketball game. We treated by four-strands Krakow's suture that stitched to three sutures anchor,
while cancellous screw plus washer introduced as internal fixation of bony avulsion at tibial tubercle.
Result: Range of motion and International Knee Documentation Committee (IKDC) score had been followed up within 2
years with good result. Full range of motion and the IKDC score 89.7 were achieved without major complication such as pain
and infection. The patient was able to return into sports activities.
Conclusion: The combination of cancellous screw with washer and three suture anchors leading into a good result in acute
total rupture of patellar tendon with bony avulsion at tibial tubercle.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Patellar Tendon Rupture; Tibial Tubercle Avulsion; Suture Anchor; Case Report.
Introduction
Patellar tendon rupture is a challenging case for the orthopaedic
surgeons. Until the nineteenth century many literatures describe
about conservative treatment, despite sporadic reports of successful
surgical repair.[1-3] The patient mostly younger than 40
years old, occur typically in young age and active population, also
commonly unilateral.[3] The disruption of extensor mechanism
of the knee joint is an essential mechanism that causing inability
to maintain standing position with involved extremity. The
mechanism of trauma is varied from low velocity, indirect blow,
penetrating injury on bending knee position whereas the extensor
mechanism in contraction.[4, 2] The rare finding showed a
patellar tendon rupture in patient which previously had harvested
tendon for ACL reconstruction.[5] Total rupture of patellar tendon
interfered the mechanism into disable condition, and leading
to morbidity ifnot treated well.[6, 7] It usually requires a surgical
repair by two most common techniques; transosseus tunneling
or suture anchor technique, depends on surgeon preference and
experience.[6-8] Suture anchor is thefirst consideration due to its
relatively easy to perform, decrease iatrogenic possibility, great
outcome to return intosports activity, range of motion and overall
outcome if compared to the other methods of tendon repair.[9,
10] Suture anchors also supports early load bearing rehabilitation
by decreasing gap formation and lowering the risk of failure or
re-rupture rate of patellar tendon repair.[10]
There were several options of surgical techniques which conducted
in many reports, such as trans-osseus tunneling, patellar
tendon augmentation with ipsilateral semitendinosus autograft,
and suture anchors.[11-13] Although biomechanical studies presented
to compare suture anchor versus transosseous tunnel, the
similar biomechanical properties was decribed, and many factors
that explained superiority of suture anchor techniques was often
reported.[14, 15] Therefore, we aim to evaluate the effectiveness
of suture anchors in management of acute patellar tendon rupture. This case report has been reported in line with the SCARE
Criteria.[16]
Case Presentation
History taking
A 14-year-old male complained of immediate onset of pain and
swollenon the right knee. He noticed while attempting to jump
off of both legs to dunk a basketball during a game. He heard
and felt the pop sound on his right knee. He was unable to actively
fully extend his right knee, while his knee in swollen and pain. He
still could not lift his leg afterwards. When he came to our centre,
the Thessaly test and Lachmann test were negative. Anteriorposterior
and lateral radiograph of right knee was taken with the
result of patella height pulled superiorly. Sagittal MRI of the right
knee identified the significant high patella (Fig. 1). The patient was
diagnosed acute patellar tendon rupture of the right knee. The
patient agreed to participate on this report for publication of the
images by the informed consent.
Surgical Technique
The surgery was performed under spinal anaesthesia and the patient
was positioned in supine position. The midline incision is
about 12 cm long started from superior border of patella to tibial
tubercle to ensure the exposure of all segments of patellar tendon.
We decided to perform patellar tendon repair that fixated with
three sutures anchor TWINFIXTM Ti Suture Anchor with two
preloaded ULTRABRAIDTM 5.0 mm (Smith & Nephew, Andover,
MA), and internal fixation of avulsed tibial tubercle using
cancellous screw 3.5mm with washer from Synthes®(Oberdorf,
Swtizerland). Initially, three suture anchors were placed below the
avulsed tibial tubercle (Fig. 2).
The patellar tendon was sutured in four-strand Krakow's technique
with ultra-braided suture from suture anchors (Fig.3). The
cancellous screw has the role of fixating the bone fragment to tibial
tubercle, as some portion patellar tendon attached to its bone.
Thereafter, the avulsed fragment of tibial tubercle was inserted
back into its right position and fixed using cancellous screw with
washer right in the middle of its initial position. The patient was
immobilized with knee brace within 4 weeks, initially full extension.
The knee was immobilized with knee brace in full extension.
Post-operative radiograph both anterior-posterior and lateral view
was taken with good position of the patella(Fig.4).
The brace was used in full extension for three weeks, the amount
of knee flexion is increased gradually until full flexion and full
weight bearing allowed at 6 weeks after surgery. Within 2 years
of followed up, the functional outcome score measured byInternational
Knee Documentation Committee (IKDC) score.The
IKDC score was 89.7, which is very good result. The full flexion
of knee was regained without pain.The patient is aprofessional
basketball player, eventually he is able return to sport activity.
Results and Discussions
Total rupture of patellar tendon is a condition of disability that
caused a significant alteration of the knee extensor mechanism,
and if untreated, the result could be a severe disability for the
patient. The etiologies were widely used traumatic and atraumatic,
which increase in patients younger than 40 years old. [3, 17, 18]
The most often traumatic factors are penetrating injury, while
simple fall or eccentric patellar tendon contraction is an atraumatic
condition, rarely ended with bony avulsion around the tibial
tubercle. [6, 8, 10, 19]
The bony avulsion of tibial tubercle were described in many studies.
[20, 21] It was vulnerableto injury by the development of apophysis
and the growth were in normal traction of patellar tendon.
The surgical fixation of bony avulsion was important, while the
surgeons chose several techniques with several different implants,
but the same principle of internal fixation. The surgery was indicated
in bony tibial tubercle fracture. The bony avulsion still
attached to the portion of the remaining patellar tendon, which
outcomes have generally beensatisfactory in many literatures. To
allow the early recovery protocol and a successful result, bone-tobone
healing was much better than tendon-to-bone healing.
The current issues of surgical technique in patellar tendon repair
were the numerous of condition and level of the rupture during
the surgery. The patellar tendon could be separated at distal border
of patella, central of patellar tendon or mid-substance, and
unexpectedly at the very distal of patellar tendon, often with a
small fragment of avulsed tibial tubercle.[6] The two widely used
techniques for fixation are transosseous tunnel or suture anchors.
[9, 15, 22] The transosseous tunnel which described early before
suture anchors, was reported in many studies that has higher rerupture
rate, due to more gap formation during functional loading
[6, 7]. Nowadays, more orthopaedic surgeons prefer suture
anchors technique to repair acute patellar tendon rupture.
In our case, beside preserving bony avulsion, we prefer to choose
suture anchors with bony avulsion preservation to improve the
stability of construction. Eventhough the cancellous screw fixed
the bone avulsion with some portion of patellar tendon still attached
to avulsed bone fragment, there was rupture of patellar
tendon that not directly connected to the bone avulsion. Tibial
tubercle avulsion has been fixed for bone-to-bone healing, while
tendon-to-tendon healing was achieved by Krakow's sutures. The
strength of the suture anchors was explained in many literatures.
Lissyetal showed the excellent improvement of functional assessment
within 6 months follow up with Krakow's sutures technique
based patellar tendon combined with knotless suture anchor to
patella, and vice versa, the knotless suture anchor to tibia.[5] Instead,
we use the combination of Krakow's sutures, three suture
anchors, and one cancellous screw as a combination method of
fixation. The relief of the symptoms and returning to sport activities
can be achieved in this case, even though the outcome of
patellar tendon rupture with bony avulsion of tibial tubercle is not
always satisfactory.
O' Dowd et al [7] evaluated 374 human knees (321 transosseous
tunnel and 53 suture anchors) retrospectively, showed significant
re-tear rate in 24 of 321 knees (7.5%) of transosseous group and
0 of 53 knees in the anchor group (p<0.05). Biomechanical study
reported by Lanzi et al [11] reported 48 porcine knees (12 transsosseous
group and 12 anchors group, randomly taken with 12
samples in each group) with all specimens of transosseous group
failed at knot tied over the proximal pole of the patella. In suture
anchors group failed 1 of 2 modes: by pullout from interference
around the anchor in the bone (5 specimens) or by suture breaking
at the first locking throw in the tendon (7 specimens). Two
cadaveric studies by Black et al and Ettinger et al were conducted
with different area of outcome; Black et al [15] reported 12 knee
of 6 cadavers (6 transosseous group and 6 anchors group whereas
suture anchors has no gap formation (2.6 mm gap in transosseous
group and 2.19 mm in anchors group), Ettinger et al [22] reported
30 knee cadavers (15 transsosseous group and 15 anchors group)
that the maximum load to failure was 301±114 N for the transosseous
group and 597±118 N for the anchors group (p<0.05).
In the avulsed tibial tubercle type of patellar tendon rupture with
suture anchors technique, some factors were contributed to the
strength; suchas suture material, number of suture anchor, suture
technique, and the cancellous screw anchor that only used in this
bony avulsion type of rupture.[12, 14, 22, 23]. The surgical technique
could be the combination of two or three suture anchors,
depending the intraoperative condition. The stability of the kneewas
examined bypassive range of motion and varus - valgus test.
In a systematic review by Grondin et al, the recovery procedure
after surgery was documented, with 52% to 100% of patients
returning to sports activities.[23] Six weeks immobilization with
gradually increased of knee flexion are currenty reported with
great result, without adverse event, and the patient returned to
professional basketball player.
Our report suggests that the use of three suture anchors combined
with the cancellous screw is effective to fix the acute patellar
tendon rupture with tibial tubercle avulsion, and the patient is
returned to sport activities without complication. The take home
message is the preserve of bony avulsion of tibial tubercle would
increase the holding strength of construction.
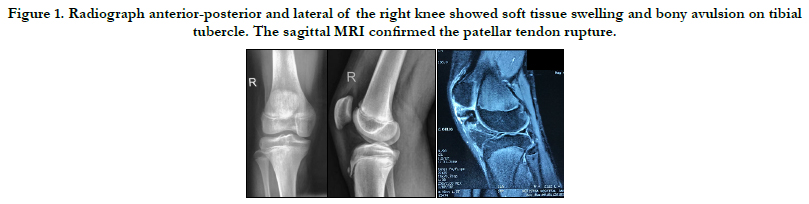
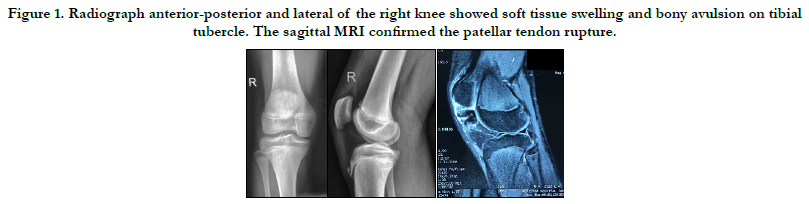
Figure 1. Radiograph anterior-posterior and lateral of the right knee showed soft tissue swelling and bony avulsion on tibial tubercle. The sagittal MRI confirmed the patellar tendon rupture.
Figure 2. The illustration of patellar tendon rupture and initially the three suture anchors was placed below the avulsed tibial tubercle.
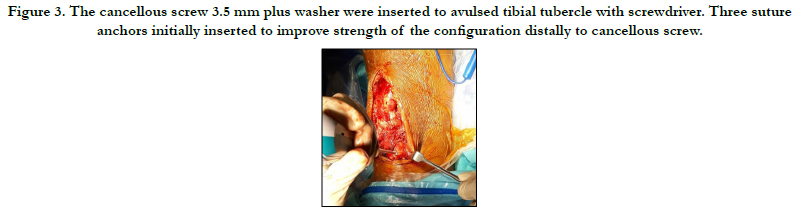
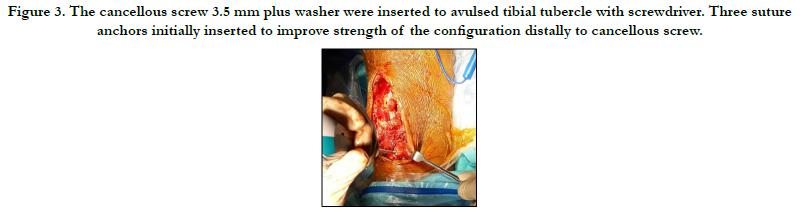
Figure 3. The cancellous screw 3.5 mm plus washer were inserted to avulsed tibial tubercle with screwdriver. Three suture anchors initially inserted to improve strength of the configuration distally to cancellous screw.
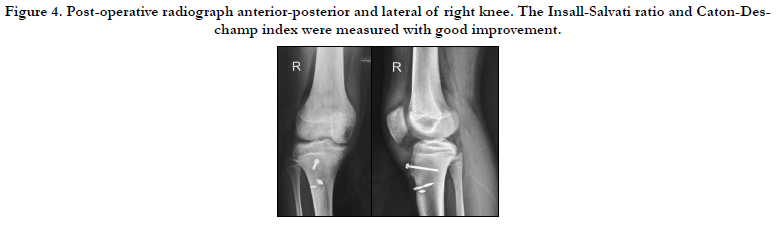
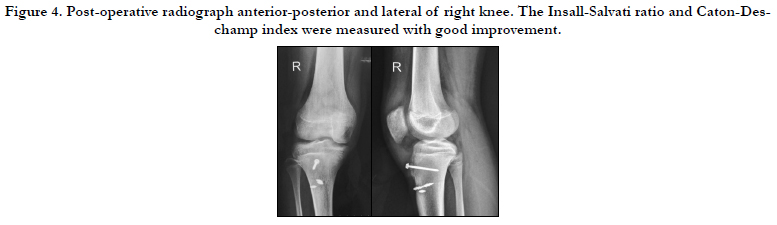
Figure 4. Post-operative radiograph anterior-posterior and lateral of right knee. The Insall-Salvati ratio and Caton-Deschamp index were measured with good improvement.
Conclusion
The combination of cancellous screw with washer and three suture
anchors leading into a good result in acute total rupture of
patellar tendon with bony avulsion at tibial tubercle. Therefore,
we recommend using suture anchors in treatment of acute patellar
tendon rupture.
Acknowledgement & Declarations
Author would like to express gratitude to the whole teaching staff
in Department of Orthopaedics and Traumatology in Faculty of
Medicine-Universitas Indonesia, Cipto Mangunkusumo General
Hospital.
References
- Matava MJ. Patellar Tendon Ruptures. J Am Acad Orthop Surg. 1996 Nov;4(6):287-296. PubMed PMID: 10797196.
- Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981 Jul;63(6):932-7. PubMed PMID: 6985557.
- Enad JG. Patellar tendon ruptures. South Med J. 1999 Jun;92(6):563-6. PubMed PMID: 10372848.
- Sanchez G, Ferrari MB, Sanchez A, Moatshe G, Chahla J, DePhillipo N, et al. Proximal Patellar Tendon Repair: Internal Brace Technique With Unicortical Buttons and Suture Tape. Arthrosc Tech. 2017 Apr 24;6(2):e491-e497. PubMed PMID: 28580272.
- Lissy M, Patel UJ. Surgical Technique: Repair of Patella Tendon Rupture in a Previously Harvested Tendon for an Anterior Cruciate Ligament Reconstruction. J Orthop Case Rep. 2019;9(4):34-40. PubMed PMID: 32405484.
- O'Dowd JA, Lehoang DM, Butler RR, Dewitt DO, Mirzayan R. Operative Treatment of Acute Patellar Tendon Ruptures. Am J Sports Med. 2020 Sep;48(11):2686-2691. PubMed PMID: 32757970.
- O’Dowd JA, Lehoang D, Butler RK, De Witt D, Mirzayan R. Trans-osseous versus Anchor Repair of Acute Patellar Tendon Ruptures. Orthop J Sports Med. 2018 Jul 27;6(7 suppl4):2325967118S00133.
- Andrea C, Federico P, Giovanni G, Alberto B. Patellar and quadriceps tendons acute repair with suture anchors. Acta Biomed. 2019 Jan 14;90(1- S):209-213. PubMed PMID: 30715027.
- Bushnell BD, Tennant JN, Rubright JH, Creighton RA. Repair of patellar tendon rupture using suture anchors. J Knee Surg. 2008 Apr;21(2):122-9. PubMed PMID: 18500063.
- Capiola D, Re L. Repair of patellar tendon rupture with suture anchors. Arthroscopy. 2007 Aug;23(8):906.e1-4. PubMed PMID: 17681216.
- Lanzi JT Jr, Felix J, Tucker CJ, Cameron KL, Rogers J, Owens BD, et al. Comparison of the Suture Anchor and Transosseous Techniques for Patellar Tendon Repair: A Biomechanical Study. Am J Sports Med. 2016 Aug;44(8):2076-80. PubMed PMID: 27179054.
- Woodmass JM, Johnson JD, Wu IT, Krych AJ, Stuart MJ. Patellar Tendon Repair With Ipsilateral Semitendinosus Autograft Augmentation. Arthrosc Tech. 2017 Nov 13;6(6):e2177-e2181. PubMed PMID: 29349015.
- Gaines RJ, Grabill SE, DeMaio M, Carr D. Patellar tendon repair with suture anchors using a combined suture technique of a Krackow-Bunnell weave. J Orthop Trauma. 2009 Jan;23(1):68-71. PubMed PMID: 19104306.
- Yen CY, Tsai YJ, Hsiao CK, Kao FC, Tu YK. Biomechanical evaluation of patellar tendon repair using Krackow suture technique. Biomed Eng Online. 2019 May 22;18(1):64. PubMed PMID: 31118104.
- Black JC, Ricci WM, Gardner MJ, McAndrew CM, Agarwalla A, Wojahn RD, et al. Novel Augmentation Technique for Patellar Tendon Repair Improves Strength and Decreases Gap Formation: A Cadaveric Study. Clin Orthop Relat Res. 2016 Dec;474(12):2611-2618. PubMed PMID: 27492687.
- Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A; SCARE Group. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg. 2020 Dec;84:226-230. PubMed PMID: 33181358.
- Kelly DW, Carter VS, Jobe FW, Kerlan RK. Patellar and quadriceps tendon ruptures--jumper's knee. Am J Sports Med. 1984 Sep-Oct;12(5):375-80. doi: 10.1177/036354658401200508. PMID: 6496835.
- Kuechle DK, Stuart MJ. Isolated rupture of the patellar tendon in athletes. Am J Sports Med. 1994 Sep-Oct;22(5):692-5. PubMed PMID: 7810795.
- Yousef MAA. Combined avulsion fracture of the tibial tubercle and patellar tendon rupture in pediatric population: case series and review of literature. Eur J Orthop Surg Traumatol. 2018 Feb;28(2):317-323. PubMed PMID: 28956182.
- Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ. Tibial tuberosity fractures in adolescents. J Child Orthop. 2008 Dec;2(6):469- 74. PubMed PMID: 19308544.
- Pereira AL, Faria ÂRV, Campos TVO, Andrade MAP, Silva GMAE. Tibial tubercle fracture associated with distal rupture of the patellar tendon: case report. Rev Bras Ortop. 2018 Jun 11;53(4):510-513. PubMed PMID: 30027088.
- Ettinger M, Dratzidis A, Hurschler C, Brand S, Calliess T, Krettek C, et al. Biomechanical properties of suture anchor repair compared with transosseous sutures in patellar tendon ruptures: a cadaveric study. Am J Sports Med. 2013 Nov;41(11):2540-4. PubMed PMID: 23982397.
- Grondin J, Menu P, Garraud T, Mesland O, Dauty M, Fouasson-Chailloux A. Return to Sport After Patellar Tendon Rupture: a Systematic Review. Muscles, Ligaments & Tendons Journal (MLTJ). 2019 Oct 1;9(4).





