Re-Engraftment of Prior Cord Blood Graft in a Patient with Relapsed/Refractory Acute Myeloid Leukaemia following Haploidentical Transplantation
Lim FLWI1*, Bari S1, Hwang WYK1
1 Singapore General Hospital, Department of Haematology, Outram Road, Singapore.
*Corresponding Author
Lim Wei Inng Francesca Lorraine,
Singapore General Hospital, Department of Haematology,
Outram Road, Singapore, 169608.
Email: francesca.lim.w.i@singhealth.com.sg
Article Type : Case Report
Received: October 29, 2015; Accepted: December 02, 2015; Published: December 04, 2015
Citation: Lim FLWI, Bari S, Hwang WYK (2015) Re-Engraftment of Prior Cord Blood Graft in a Patient with Relapsed/Refractory Acute Myeloid Leukaemia following Haploidentical Transplantation. Int J Stem Cell Res Transplant 03(6), 125-128. doi: dx.doi.org/10.19070/2328-3548-1500021
Copyright: Lim FLWI© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
We report the case of a 32-year-old man with poor risk acute myeloid leukemia (AML) who received transplantation of an UCB graft following myeloablative conditioning but unfortunately relapsed after one year with complete loss of donor chimerism. As this patient did not have an HLA - matched sibling donor or a volunteer MUD, he went on to receive a second transplant with haploidentical CD34 cells from his mother following a non-myeloablative conditioning. After initial engraftment with the haploidentical donor cells, the patient became progressively pancytopenic and chimerism analysis revealed decreased level of cells derived from the haploidentical graft. However, there was a concurrent increasing ratio of the UCB derived cells from the first transplant. The patient had eventual recovery and stabilization of his full blood count and repeat chimerism analysis demonstrated successful re-engraftment with the previous UCB graft. To the best of our knowledge, no such similar cases have been reported in the literature. Thus, cord blood cells from a prior transplant could remain present in small quantities at the phase ofleukemia relapse and re-emerge to establish long term hematopoiesis even after graft failure from a subsequent haploidentical transplant.
2.Introduction
3.Background
4.Case Presentation
5.Discussion
6.Conclusion
7.Consent
8.Author's Contribution
9.References
Keywords
Umbilical Cord Blood Transplant; Haploidentical Transplant; Relapse; Chimerism; Graft Failure.
Background
Allogeneic hematopoietic stem cell transplantation (HSCT) is a widely used therapeutic option in the management of advanced or high risk acute myeloid leukemia (AML). In fact, according to National Marrow Donor Program (NMDP, USA) over 35% of HSCT recipients in 2014 were diagnosed with AML. For patients who lack ahuman leukocyte antigen (HLA)-matched sibling donor or a volunteer matched unrelated donor (MUD), or when there is insufficient time for donor work up due to rapid progression of disease, there are two rapidly available alternative stem cell donor sources: a haploidentical transplantation from a family member or an unrelated umbilical cord blood (UCB) from a cord blood bank [1]. The choice of UCB versus haploidentical donor varies from institution to institution both with their respective advantages and disadvantages. With regards to UCB transplantation (UCBT), the relative ease of procurement of UCB together with its favourable alloreactivity with less risk of developing graft-versus- host-disease (GVHD) but maintaining the graft-versus-leukaemia (GVL) effect has made the use of UCB as a source of hematopoietic stem & progenitor cells (HSPCs) highly attractive [1]. With regards to haploidentical stem cell transplant (haplo SCT), a major advantage is its immediate availability and its potential strong GVL effect [1]. However the reason for a transplant centre to select one or the other option is often dependent on the specific expertise and familiarity with the respective approaches.Both UCBT and haplo SCT are important strategies for patients who do not have a fully matched donor.
During the post-transplant period, surveillance of allogeneic HSCT recipients is important and necessary and is often done by chimerism analysis comparing the ratio of donor and recipient derived cells; of which there are several methodological approaches. DNA microsatellite polymorphism, often referred to as short tandem repeats, have remained the most commonly used approaches [2]. Chimerism analysis can help assess if engraftment has been successful [3]. It can also provide an early indication of the risk of graft rejection/failure and of impending relapse [3]. Failure to engraft after HSCT or to sustain engraftment is a significant complication due to many possible factors. Fortunately, this complication is uncommon and occurs at an overall frequency of less than 5% and can be overcome by additional HSPC infusions. Several risk factors for graft failure include low HSPC dosewhere the quantity and quality of donor T lymphocytes are very important for successful engraftment; degree of HLA mismatch for unrelated donor transplant and major ABO blood group mismatched transplants; T-cell depletion of graft; reduced intensity conditioning (RIC) regimens; and viral infections, specifically, cytomegalovirus (CMV), human herpes virus type 6 (HHV6) and parvovirus. Drug toxicity and septicaemia have also been known to induce graft failure. Definitive recommendations for treatment of such complications are yet to be established [2].
This case report is about a patient with high risk AML who relapsed after an umbilical cord blood transplant. He went on to receive a haploidentical transplant from his mother. However this was complicated by further graft rejection/failure. Chimerism study revealed re-engraftment with UCB cells from his preceding transplant. The patient is currently well with limited chronic GVHD of the skin.
Case Presentation
A 32 year old man with no past medical history presented with fever in 2011. The patient was pancytopenia with haemoglobin (Hb) of 4.7g/dL, white blood cell (WBC)count of 41.3 x103/uL and platelet (PLT) count of 54 x 103/uL. Bone marrow aspirate confirmed the diagnosis of AML. Further tests revealed normal cytogenetics and presence of the FLT3 internal tandem duplication (FLT3-ITD) mutation. The patient received induction chemotherapy with idarubicin and cytarabine and achieved complete remission (CR) following which he received consolidation treatment with further cytarabine. In view of the presence of FLT3- ITD; a poor prognostic marker for AML, the patient was recommended to undergo further treatment with allogeneic HSCT. As the patient had no match sibling or unrelated donor, it was decided to perform an umbilicalcord blood transplant (UCBT). The conditioning regime consisted of fludarabine (25mg/m2, day -7 to -5), cyclophosphamide (60mg/kg day -6 to -5) and 1200cGy TBI (6 doses of 200cGy day -3 to -1). He was transplanted with two 4/6 HLA-matched cord blood units (CBU) with a total nucleated and CD34+ cell dosage of 4.3x107 cells/kg and 2.02x105 cells/kg respectively. Graft versus host disease (GVHD) prophylaxis comprised of cyclosporine (CSA) and mycophenolatemofetil (MMF). Neutrophil engraftment (defined by absolute neutrophil count of > 500 cells per μl for three consecutive days) occurred on day 18 and platelet engraftment (defined by platelet count > 20,000 per μl for three consecutive days) occurred on day 32. Chimerism analysis on day 14 and day 28 showed 100% CBU #1 engraftment in the mononuclear cells and the granulocytes. His posttransplant course was complicated by an episode of line related infection and grade 1 cutaneous and gastrointestinal GVHD. After which the patient remained well and his immunosuppressants were gradually tapered over a period of six months and eventually stopped. However, during regular follow up at 16 months post UCBT, patient relapsed with circulating blasts present on his full blood count (FBC). As a result, the patient received treatment with fludarabine, high dose cytarabine and idarubicin and achieved a second CR. Again no HLA compatible donors were identified. After discussion with patient, it was decided to perform haploidentical transplantation of stem cells from his mother who had a 4/8 HLA match with minor ABO mismatch. The conditioning regimen consisted of fludarabine (30 mg/m2, day -7 to -3), cyclophosphamide (14.5mg/kg, day -7 to -6) and 200cGy TBI (1#, day -2). He receiveda CD34+ cell dose of 3.15x106 cells/ kg after a total of three apheresis sessions from his mother. The haploidentical graft also contained CD3+ T cells of 372.79x106 cells/kg. GVHD prophylaxis was tacrolimus and mycophenolate. His post-transplant course was complicated by Escherichia coli infection and pancytopenia.
Peripheral blood DNA microsatellite polymorphism analysis on day 14 and day 28 on the D1S80 loci showed 95-100% donor cells in both the mononuclear cells and the granulocyte series. However the patient remained pancytopenic. One month post haploidentical transplant, the patient had Hbof 6.9g/dL, total WBC and PLT count of 0.55 x103/uL and 3 x103/uL respectively which persisted for at least 5 months. Repeat chimerism analysis demonstrated a falling donor cell chimerism of 10% from his mother (Figure 1). Based on the chimerism results, it is evident that the patient had graft rejection with failure to sustain the engraftment following haploidentical SCT. During this period, the patient received supportive treatment with blood products. He required at least two blood and platelet transfusion per week with intermittent filgrastim. He also received a trial treatment with eltrombopag, a thrombopoeitin receptor agonist, for 12 weeks; however, the patient’s platelet count still remained low. The option of a repeat HSCT was proposed to the patient; however he was not keen to undergo yet another round of HSCT. Analysis of chimerism was intermittently repeated which persisted to show a donor cell chimerism of 10% from his mother but 95-100% chimerism with the previous CBU #1. Interestingly after 6 months post haploidentical transplant, there was gradual improvement in the patient’s full blood count and by the seventh month, he was completely independent of blood and platelet transfusion.
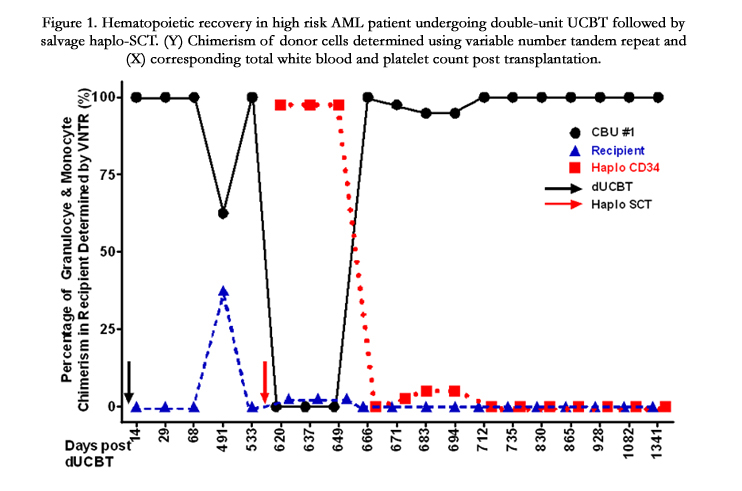

Figure 1. Hematopoietic recovery in high risk AML patient undergoing double-unit UCBT followed by salvage haplo-SCT. (Y) Chimerism of donor cells determined using variable number tandem repeat and (X) corresponding total white blood and platelet count post transplantation.
Discussion
This patient was diagnosed at the age of 30 years with FLT 3 internal tandem duplication (FLT3-ITD) positive AML with normal cytogenetics. He achieved first CR after induction chemotherapy. Ideally a HLA identical sibling donor would have been the preferred source of HSPC; however this was not available as our patient has no siblings. Further search for a MUD was also unsuccessful. As his parents are of the upper age limit for donors and our center having performed more UCBT compared to haplo SCT the decision was made for UCBT following discussion with the patient. This patient unfortunately relapsed after 16 months post UCBT. He went on to receive salvage chemotherapy and was able to enter CR2. The decision was made to perform haploidentical transplantation from his mother. However, 30 days post haplo SCT, the patient remained pancytopenic and chimerism analysis revealed only 10% of donor cells derived from his mother but with re-engraftment with the initial CBU#1 (100%) that the patient previously received. It is evident from the chimerism analysis that the patient had developed graft failure with the haplo SCT, however interestingly the patient had re-engrafted with his previous UCB graft. Over a period of time his counts showed improvement and repeat chimerism studies have demonstrated persistent engraftment with cord blood cells (Figure 1).
With wider usage of UCB and other HLA-mismatched transplants, graft failure is becoming an increasing problem of HSCT and is associated with high morbidity and mortality. It often manifests as either an initial lack of engraftment of donor cells, or as a loss of donor cells after initial engraftment as illustrated by our patient.Our patient had several risk factors for graft failure such as low stem cell dose for the UCBT and the use of a non myeloablative conditioning regime and a HLA-mismatched graft for the haplo SCT. The initial chimerism result indicated probable graft failure. However repeat analysis showed further reduction in the ratio of donor cells and the patient remained pancytopenic requiring blood and platelet transfusion support twice a week. Graft dysfunction, regardless of the etiology, should be recognized early and management often consists of the use of growth factors without additional HSPC infusions, infusions of HSPC without additional cytotoxic therapy or the performance of re-transplant with pre-infusion conditioning. But our patient is unique in that he had eventual recovery in his counts with re-engraftment with the initial CBU#1 from his first transplant. The mechanism as to why the patient was able to re-engraft with the cells from the CBU is not known. A literature search was performed but no such case has been reported before. Contrary to our findings,in other studies, the implementation of salvage HSCT with RIC conditioning using haploidentical CD34 graft due to failure of initial UCBT have always shown long term donor chimerism from the second haploidentical transplant [4-6]. However, it is known that there is significant shortening of peripheral blood mononuclear cell (PBMNC) telomeres in the recipient post bone marrow transplant [7]. Similar studies conducted on allogeneic UCB HSC transplant recipients demonstrated significantly longer telomeres compared to the allogeneic PBHSC transplant recipients and this in turn could be indicative of a replicative advantage inherent in the use of UCB HSC for transplant and could account for the delayed re-engraftment with the previous UCB unit [8]. We have previously shown that cord blood grafts can engraft late despite protractedly undetectable donor chimerisms in the initial period after transplant and others have also shown that in double unit cord blood transplants, the CB unit contributing to long term engraftment may not be the cord blood unit that initially appears to engraft [9]. In several studies, UCB grafts have been concurrently transplanted with haplo CD34 cells to overcome the problem of low cell dosage, which have resulted in faster and more robust engraftment of the UCB graft compared to the conventional use of single or dual UCBT, the mechanism of such is yet undefined [5, 10]. Hence would it be possible that in our patient, the infusion of the haplo CD34 cells could have acted as a catalyst for the UCB HSPC to reinitiate hematopoietic activity. These findings could also partly support previous basic findings that HSPC are very quiescent cells that could survive through several cycles of chemotherapy [11]. Also it could be speculated that the haploidentical graft consisting of a significant number of T cells and its different subsets, specifically T regulatory cells, could have exerted a GVL effect on the AML blast cells thus serving as an unintended session of immunotherapy [12]. Following such potential immunotherapy, a permissive niche could have been created for the UCB HSPC to regain hematopoietic activity in the patient. It could be further extrapolated that the UCB derived T cells could have led to an eventual loss of the haploidentical cells due to a graft versus graft effect. We believe that this current report lends weight to the hypothesis that cord blood hematopoietic stem cells have greater stem cell potential and that infused cord blood cells could remain undetectable and quiescent, engrafting later when conditions permit.
Conclusion
This is an interesting case of a patient with high risk AML who relapsed 1 year after a CBT blood transplant. He went on to receive a haploidentical transplant from his mother. This was complicated by graft failure but chimerism study revealed re-engraftment with the previous CBT cells which was unexpected and intriguing. The mechanism as to why the patient was able to re-engraft with the cells from the initial CBU is not known.
Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author's Contribution
This patient is under the care of HYKW and provided medical details of the patient’s condition and treatment. LWIFL and SB helped draft the case report. All authors read and approved the final manuscript.
References
- Ballen KK, Spitzer TR (2011) The great debate: haploidentical or cord blood transplant. Bone Marrow Transplant 46(3): 323-329.
- Mattsson J, Ringdén O, Storb R (2008) Graft Failure after Allogeneic Hematopoietic Cell Transplantation. Biol Blood Marrow Transplant 14(Supplement 1): 165-170.
- Stikvoort A, Gertow J, Sundin M, Remberger M, Mattsson J, et al. (2013) Chimerism patterns of long-term stable mixed chimeras posthematopoietic stem cell transplantation in patients with nonmalignant diseases: follow-up of long-term stable mixed chimerism patients. Biol Blood Marrow Transplant 19(5): 838-844.
- Fernández MN (2009) Improving the outcome of cord blood transplantation: use of mobilized HSC and other cells from third party donors. Br J Haematol 147(2): 161-176.
- Bautista G, Cabrera JR, Regidor C, Forés R, García-Marco JA, et al. (2009) Cord blood transplants supported by co-infusion of mobilized hematopoietic stem cells from a third-party donor. Bone Marrow Transplant 43(5): 365-373.
- Yoshihara S, Ikegame K, Taniguchi K, Kaida K, Kim EH, et al. (2012) Salvage haploidentical transplantation for graft failure using reduced-intensity conditioning. Bone Marrow Transplant 47(3): 369-373.
- Awaya N, Baerlocher GM, Manley TJ, Sanders JE, Mielcarek M, et al. (2002) Telomere shortening in hematopoietic stem cell transplantation: a potential mechanism for late graft failure? Biol Blood Marrow Transplant 8(11): 597-600.
- Pipes BL, Tsang T, Peng SX, Fiederlein R, Graham M, et al. (2006) Telomere length changes after umbilical cord blood transplant. Transfusion46(6): 1038-1043.
- Sideri A, Neokleous N, Brunet De La Grange P, Guerton B, Le BousseKerdilles MC, et al. (2011) An overview of the progress on double umbilical cord blood transplantation. Haematologica 96(8): 1213-1220.
- Magro E, Regidor C, Cabrera R, Sanjuán I, Forès R, et al. (2006) Early hematopoietic recovery after single unit unrelated cord blood transplantation in adults supported by co-infusion of mobilized stem cells from a third party donor. Haematologica 91(5): 640-648.
- Pietras EM, Warr MR, Passegué E (2011) Cell cycle regulation in hematopoietic stem cells. J Cell Biol 195(5): 709-720.
- Zou W (2006) Regulatory T cells, tumour immunity and immunotherapy. Nat Rev Immunol 6(4): 295-307.





