Laparoscopic Guided Transversus Abdominus Plane (Tap) Block – A Modified Technique
S.Gupta1*, F.ElMedani2, K Jain3
1 Consultant Surgeon, Departments of Surgery and Radiology, Lister Hospital, Stevenage, Hertfordshire, SG1 4AB, UK.
2 Registrar Surgery, Departments of Surgery and Radiology, Lister Hospital, Stevenage, Hertfordshire, SG1 4AB, UK.
3 Consultant Radiologist, Departments of Surgery and Radiology, Lister Hospital, Stevenage, Hertfordshire, SG1 4AB, UK.
*Corresponding Author
Sanjay Gupta,
Consultant Surgeon,
Departments of Surgery and Radiology, Lister Hospital,
Stevenage, Hertfordshire, SG1 4AB, UK.
E-mail: sanjay.gupta@nhs.net
Article Type: Brief Report
Received: August 18, 2014; Accepted: October 26, 2014; Published: October 27, 2014
Citation: S.Gupta, F.ElMedani, K Jain (2014) Laparoscopic guided Transversus Abdominus Plane (TAP) Block – a modified technique. Int J Anesth Res. 2(7), 68-69. doi: dx.doi.org/10.19070/2332-2780-1400017
Copyright: S.Gupta© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
We present a modified laparoscopic technique to administer quick and effective Tansversesus Abdominus Plane (TAP) block. The technique combines the benefit of laparoscopic guidance along with the knowledge of radiological anatomy of the abdominal wall.
2.Background
3.Surgical technique
4.Discussion and Results
5.References
Keywords
TAP Block.
Background
Whilst performing ultra-sound guided TAP block, we have observed the distance between the peritoneum and the neuro-vascular plane (plane between transverses abdominus and internal oblique) in the mid-axillary line to be relatively constant between 3-4 mm (figure. 1). This was further confirmed on ultra-sound scanning of 10 healthy volunteers by our radiologist. This anatomical fact has been utilised as the basis of current Laparoscopic guided TAP block technique.
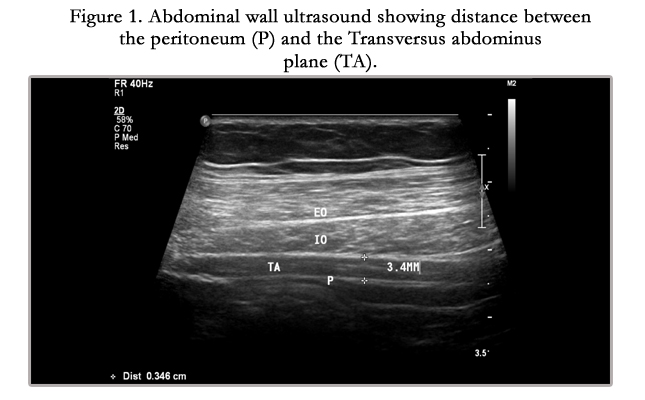

Figure 1. Abdominal wall ultrasound showing distance between the peritoneum (P) and the Transversus abdominus plane (TA).
Surgical technique
Pneumo-insuffulation is induced by open Has on cannulation of the umbilicus. A21gauge graduated regional anaesthesia needle(UniPlexNanoline, Pajunk® - figure. 2) is inserted through the skin in the mid axillary line midway between the costal arch and the iliac crest. The needle is advanced slowly until the needle tip reaches sub-peritoneal plane, easily identified on laparoscopy by peritoneal tenting. Caution is exercised by inserting the needle slowly so as to avoid any peritoneal puncture. Guided by the markings on the needle, the tip is then withdrawn by 3-4 mm so as to enter the neuro-vascular plane of the anterior abdominal wall. 20 ml of 0.25% Bupivacaine is then injected in this plane on each side (for bilateral blocks). The correct position of needle tip is confirmed by a slowly spreading bulge on laparoscopy (figure. 3).
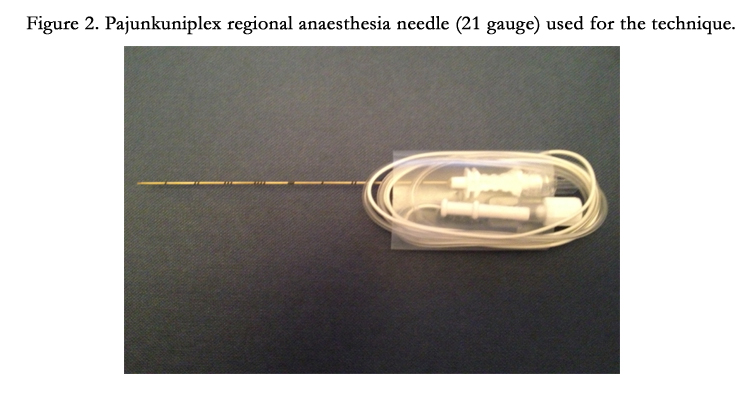
Figure 2. Pajunkuniplex regional anaesthesia needle (21 gauge) used for the technique.
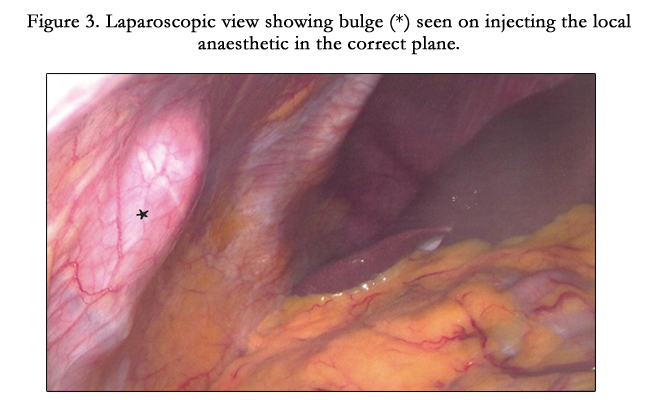
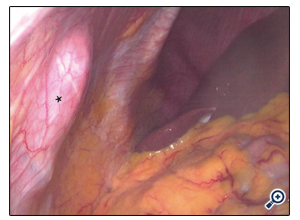
Figure 3. Laparoscopic view showing bulge (*) seen on injecting the local anaesthetic in the correct plane.
Discussion and Results
TAP block first described in 2001 [1], is an effective technique in providing post-operative analgesia especially following lower abdominal incisions [2]. Conventionally the block is performed using the classical ‘double pop’ technique or under ultrasound guidance. Laparoscopic guided TAP block first described in 2011 [3], is a simple and easy alternative obviating the need for an operative ultra-sound.
The current technique combines the merits of ultra-sound guided and laparoscopic guided techniques to enhance the speed and accuracy of the TAP block. Direct Laparoscopic visualisation of the needle tip renders the technique much faster when compared to ultra-sonic guidance. Knowledge of radiological anatomy as confirmed by our ultra-sound studies helps to increase the accuracy of drug delivery in the correct plane. We have used this technique on 30 patients undergoing laparoscopic lower abdominal procedures (hernia repairs and appendectomies). All these patients did well with only two patients requiring post-operative opiates. Further trials are being planned to confirm these findings.
References
- Rafi AN (2001). Abdominal field block: a new approach via the lumbar triangle. Anaesthesia; 56: 1024-6.
- Findlay JM, AshrafAQ, Congahan P (2012). Transversus abdominus plane (TAP) blocks-A review. The Surgeon; 10: 3611-67.
- Chetwood A, Agarwal S, Hrouda D, Doyle P (2011). Laparoscopic assisted transeversus abdominus plane block: a novel insertion technique during laparoscopic nephrectomy. Anaesthesia; 66(4): 317-18.





