Perioperative Anesthetic Management of a Patient with Primary Lateral Sclerosis
Lee L1*, Kapoor R2
1 Resident, Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, 43210, USA.
2 Assistant Professor, Clinical Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, 43210, USA.
*Corresponding Author
Linden Lee, MD,
Resident, Department of Anesthesiology, The Ohio State University,
Wexner Medical Center, Columbus, OH, 43210, USA.
Tel: 614-293-8487
Fax: 614-293-8153
E-Mail: Linden.Lee@osumc.edu
Article Type: Case Report
Received: November 13, 2014; Accepted: January 06, 2015; Published: January 12, 2015.
Citation: Lee L, Kapoor R (2015) Perioperative Anesthetic Management of A Patient with Primary Lateral Sclerosis. Int J Anesth Res. 3(1) 76-78.doi: dx.doi.org/10.19070/2332-2780-1500019
Copyright: Lee L© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Primary lateral sclerosis (PLS) is a rare degenerative disorder of the upper motor neurons innervating the voluntary musculature.
In this report, we describe the perioperative management of a patient diagnosed with PLS and investigate strategies to optimize treatment outcomes in this patient population.
2.Introduction
3.Case Description
4.Discussion
5.References
Keywords
Primary Lateral Sclerosis; Neuromuscular Disease; Amyotrophic Lateral Sclerosis.
Introduction
Primary lateral sclerosis (PLS) is a rare degenerative disorder of the upper motor neurons innervating the voluntary musculature. [1] It falls under the spectrum of motor neuron disorders which also includes the most common motor neuron disease, amyotrophic lateral sclerosis (ALS). ALS is distinguished by mixed upper and lower motor neuron dysfunction, whereas PLS is primarily an upper motor neuron disease. The most common manifestations of PLS are leg weakness and spasticity, and spastic bulbar weakness. [2] Symptoms of PLS typically begin in the fifth to sixth decade of life. Whereas ALS is rapidly progressive and the average life expectancy with ALS is about 3 years, PLS tends to follow a very
slowly progressive course. Longevity information for PLS cases is still incomplete. [3]There is no specific diagnostic test for PLS; however, it is distinguishable from ALS and other disorders that cause progressive spasticity by clinical criteria (Table 1). [4] As with ALS, there is no definitive treatment for PLS.
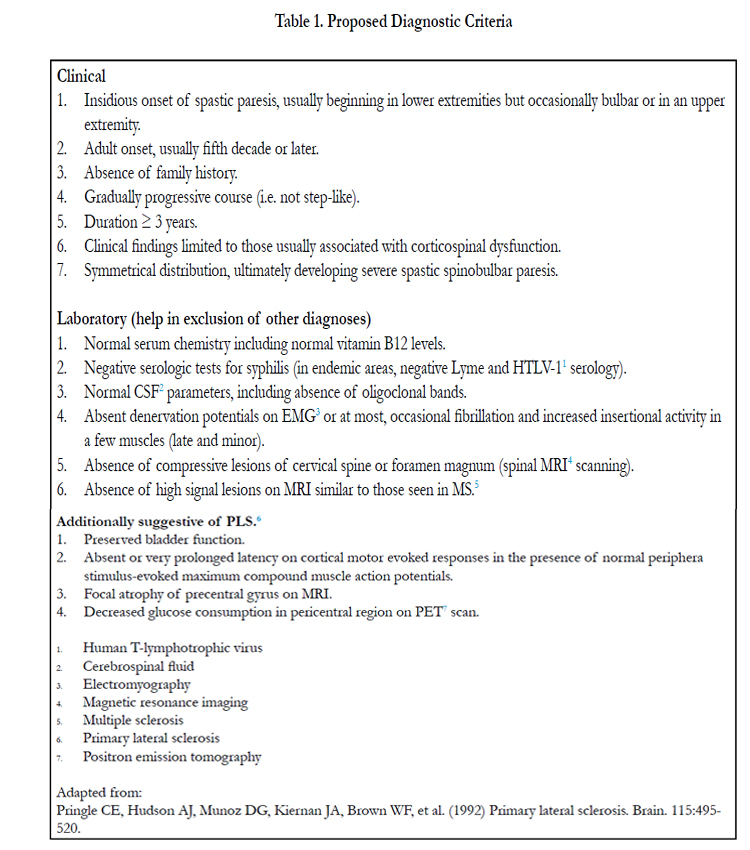

Table 1. Proposed Diagnostic Criteria.
Some consider PLS to be a variant of ALS, and while many articles have been published that outline anesthetic management in patients with ALS, few detail anesthetic management in patients with PLS. [3] We discuss here a case of a patient with PLS undergoing surgery and the preoperative, intraoperative, and postoperative concerns in patients with PLS.
Case Description
A 54-year-old male with a history of PLS presented for replacement of his intrathecal baclofen pump. His past medical history was significant for PLS, hypertension, hyperlipidemia, obstructive sleep apnea, and umbilical hernia. The patient was diagnosed with PLS at age 47 after initially presenting with progressive balance difficulties and frequent falls. His symptoms were comprised primarily of bilateral lower extremity spasticity which was improved with intrathecal baclofen. However at the time of presentation, his intrathecal baclofen pump was nearing the end of its useful life and required replacement.
The patient’s surgical history was significant for intrathecal baclofen pump placement, cervical spine fusion following C6-C7 fracture from a fall, tear duct surgery, and lumbar spine surgery. The patient had no known drug allergies and did not use tobacco or alcohol. He ambulated with the use of a cane. His family history was not significant for any known neurological disorders. The patient’s medication list included amitriptyline, gabapentin, intrathecal baclofen, hydrocodone-acetaminophen, sertraline, atenolol, simvastatin, and pantoprazole.
The patient visited the preoperative assessment center four days prior to his scheduled surgery. The patient was 178 cm tall, weighed 110 kg, and had a BMI of 35. His vital signs were as follows: temperature 36.9°C, heart rate 71 bpm, blood pressure 117/77 mmHg, oxygen saturation 95% on room air. His functional capacity was determined to be mildly impaired given mild dyspnea at rest. Spasticity and bulbar symptoms were not present
on physical exam. Previous anesthesia records were obtained which demonstrated that the patient was an easy intubation using a MAC4 laryngoscope blade and was extubated uneventfully at the conclusion of his surgery for intrathecal baclofen pump placement at age 48. No electrocardiographic abnormalities were noted. Pulmonary function test results were grossly normal with forced vital capacity (FVC) 93% of predicted, forced expiratory
volume in one second (FEV1) 87% of predicted, FEV1/FVC ratio 94% of predicted, and sniff nasal-inspiratory force 98% of predicted.
On the day of surgery, standard American Society of Anesthesiologists monitors were applied and an 18 gauge IV was placed in the patient’s left upper extremity. The patient was premedicated with midazolam 2 mg, preoxygenated, and induced with fentanyl 50 mcg and propofol 300 mg. A neuromuscular blocking agent was not administered. He was intubated without difficulty using a MAC3 laryngoscope blade, a 7.0 endotracheal tube was placed with one attempt, and the endotracheal tube was secured at 24 cm at the lips. Controlled mechanical ventilation was initiated and anesthesia was maintained with sevoflurane 2% in 50% oxygen-50% air mixture. The patient was placed in the left lateral decubitus
position for surgical exposure. Mean arterial blood pressure was maintained within 20% of the patient’s baseline using periodic boluses of phenylephrine. The patient received an additional 50 mcg of fentanyl during the procedure in addition to ondansetron 4 mg prior to emergence. A total of 800 ml Lactated Ringer’s solution was given during the surgery. The patient was suctioned and extubated at the conclusion of the surgery after standard extubation criteria – including responsiveness to verbal commands, tidal volume >5cc/kg, and sustained head lift – were met. He was
admitted overnight given his history of obstructive sleep apnea and PLS, and was discharged home on postoperative day 1.
Discussion
When formulating an anesthetic plan for a patient with PLS, a systematic approach is advised. Preoperatively, efforts should be made to determine the severity of the patient’s disease. Spasticity, bulbar symptoms, and ventilatory support at baseline can indicate progressive disease. Patients with prominent bulbar symptoms or advanced disease are at increased risk of aspiration and respiratory failure. [5] Pulmonary function testing can be utilized to assess respiratory function through metrics such as sniff nasalinspiratory force (SNIF) and vital capacity. Prediction of respiratory failure based on the results of pulmonary testing is imprecise, but decreased measures of inspiratory force (particularly SNIF) and vital capacity less than 50% of predicted are concerning indicators. [5] Neurology consultation may also prove valuable for preoperative assessment as well as for continuity of care. Local, regional, spinal, and epidural anesthesia have all been used successfully in patients with ALS [6]-[8] and should be considered for appropriate surgeries in patients with PLS to avoid possible postoperative respiratory failure following general anesthesia. If general anesthesia is to be administered, the patient should be informed about the potential of postoperative respiratory failure, intensive care unit admission, and tracheostomy.
Patients with neuromuscular disease may be sensitive to sedativehypnotics, so using these medications judiciously or considering a short-acting induction agent such as propofol may help avoid prolonged effects. [9] Intraoperatively, succinylcholine should not be administered due to the risk of life-threatening hyperkalemia while nondepolarizing neuromuscular blocking agents should be used cautiously as patients with PLS may demonstrate an increased sensitivity to these drugs. No neuromuscular blocking agents were administered during this case to avoid postoperative respiratory failure and prolonged muscle weakness. Maintenance with volatile anesthetics as well as by total intravenous anesthesia has been successfully performed. [5] Selection of a volatile agent with a short duration of action, such as desflurane or sevoflurane, may be preferential to avoid prolonged emergence. If the patient has severe disease, limiting premedication and intraoperative opioids, as well as using short-acting opioids like fentanyl or remifentanil should be considered. Such an approach will minimize the risk of respiratory depression at emergence. Patients with severe disease are at increased risk of aspiration. In these patients, airway patency should be ensured by oropharyngeal suctioning. The anesthesia providers must be prepared to manage the airway if the patient is unable to protect his airway after extubation. Lastly, the
patient must have sufficient respiratory drive and meet extubation criteria prior to extubation.
Postoperatively, patients may require ventilatory support; therefore, close monitoring and appropriate disposition are essential. If the patient is extubated, overnight admission to ensure that the patient’s respiratory function returns to baseline prior to discharge should be considered.
In conclusion, patients with PLS present the anesthesiologist with multiple challenges. Adequate planning, preparation, and perioperative management are essential to avoid complications and improve treatment outcomes in patients with PLS.
References
- Swash M, Desai J, Misra VP (1999) What is primary lateral sclerosis? Journal of the Neurological Sciences. 170: 5-10.
- Singer MA, Statland JM, Wolfe GI, Barohn RJ. (2007) Primary lateral sclerosis. Muscle & Nerve. 35: 291-302.
- Tomik B, Zur KA, Szczudlik A. (2008) Pure primary lateral sclerosis – Case reports. Clinical Neurology and Neurosurgery. 110: 387-391.
- Floeter MK, Mills R. (2009) Progression in primary lateral sclerosis: a progressive analysis. Amyotroph Lateral Scler. 10: 339-346.
- Fleisher LA. (2012) Anesthesia and Uncommon Diseases. Saunders, Philadelphia. pp 273-275.
- Kochi T, Oka T, Mizuguchi T. (1989) Epidural anesthesia for patients with amyotrophic lateral sclerosis. Anesthesia & Analgesia. 68: 410-412.
- Sertoz N, Karaman S. (2012) Peripheral nerve block in a patient with amyotrophic lateral sclerosis. Journal of Anesthesia. 26: 314-315.
- Park K, Son B, Hwang D, Jeon Y. (2012) Spinal anesthetic management for discectomy in a patient with amyotrophic lateral sclerosis. Korean Journal of Anesthesiology. 63(6): 547-549.
- Romero A, Joshi GP. (2013) Neuromuscular disease and anesthesia. Muscle Nerve. 48(3): 451-60.





