Ultrasonography of the Airway: A Bedside Predictor of Difficult to Intubate Obese Patients
Byron Rosero-Britton1*, Kapoor R1, Astrid Lopez-Gomez1, Kimura S1, Muhammad Shabsigh1, Bergese SD1,2
1 Department of Anesthesiology, The Ohio State University, Wexner Medical Center, Columbus, Ohio, United States.
2 Department of Neurological Surgery, The Ohio State University, Wexner Medical Center, Columbus, Ohio, United States.
*Corresponding Author
Byron Rosero-Britton MD,
The Ohio State University, Wexner Medical Center,
Department of Anesthesiology,
Doan Hall N411, 410 West 10th Avenue Columbus,
Ohio 43210.
Tel: 614-366-8397
Fax: 614-366-1943
E-mail: byronrb@gmail.com
Received: November 05, 2015; Accepted: December 03, 2015; Published: December 05, 2015
Citation: Byron Rosero-Britton, et al., (2015) Ultrasonography of the Airway: A Bedside Predictor of Difficult to Intubate Obese Patients. Int J Anesth Res. 3(11), 172-175.DOI : dx.doi.org/10.19070/2332-2780-1500042
Copyright: Byron Rosero-Britton© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A complete airway assessment of patients requiring monitored anesthesia care, regional anesthesia or general anesthesia, identifies difficult to intubate individuals and potential complications. Ultrasound (US) is considered a noninvasive, easy to perform bedside airway assessment tool for difficult to intubate patients. We performed a review of the literature available in PubMed using keywords such as: airway management, endotracheal intubation, ultrasonography, obesity, and body mass index. Based on our literature review we concluded that ultrasound could potentially be a useful addition to the traditional methods of diagnosing difficult airways in morbidly obese patients
2.Introduction
3.Conclusion
4.Conflict of Interest Statement
6.References
Keywords
Airway Management; Body Mass Index; Difficult Airways; Endotracheal Intubation; Obesity; Ultrasonography.
Proper airway management (AM) is an essential goal for anesthesia providers [1]. In his Letter to the Editor published in 1999 in Canadian Journal of Anesthesiology, Jonathan Benum of emphasized the importance of high quality training in AM, to prevent complications related to general anesthesia administration [2]. A complete preoperative airway assessment should be accomplished in order to assure a proper AM intraoperatively [3]. The results presented by the Royal College of Anesthetists of the United Kingdom and the Difficult Airway Society of the United Kingdom in the Fourth National Audit Project (NAP4), suggested that poor airway assessment and planning contributed to unfortunate airway outcomes [4].
Every patient undergoing regional or general anesthesia must be evaluated before the procedure to anticipate a potentially difficult airway (DA) [5, 6]. The anesthesiologist must create both a plan and a backup AM strategy based on the patient’s medical history, type of surgery, and predicted difficult airway access [7]. Multiple bedside tests such as Mallampati score, Patil’s test (Thyromental distance - TMD), Savva’s test (Sterno-mental distance -; SMD), Mandibulo-hyoid distance, inter-incisor distance (IID), upper lip bite test (ULBT), are available to evaluate patient’s airway; however these are proved to be of poor predictive value in identifying patients with evident airway abnormality or pathology [8-12]. Khan et al. assessed preoperatively the airway of 380 patients who were scheduled for surgery using the TMB, IID, SMD and ULBT. After induction of general anesthesia Cormack and Lehane was performed, and difficult intubation was defined as grade 3-4. Specificity, sensitivity, positive and negative predictive value of each test individually and in combination with ULBT was calculated. Khan conclude that the combination of UBLT with SMD offered the highest sensitivity and the ULBT by itself had a higher specificity and accuracy when compared with the other tests [11].
The lack of accuracy of the preoperative bedside tests to perform airway assessment (AA) and predict DA, creates opportunities to identify new tools of evaluating patients with anatomic abnormalities. Advanced methods of AA such as endoscopy, MRI (magnetic resonance imaging) or CT (computed tomography) are not cost-effective, and are time-consuming when fast bedside tests for AA are required [7].
The CDC (Center for Disease Control and Prevention) and the WHO (World Health Organization) define obesity as a BMI greater than or equal to 30kg/m2 [13-15] Some authors referred to this alarming increase in obese population as a “global pandemic”[16]. Obese patients are considered at increased risk for pulmonary complications, difficult bag-mask ventilation, and difficult endotracheal intubation [17]. Nevertheless, obesity as a selfdetermining risk factor for difficult endotracheal intubation has been controversial. Some studies suggest that obesity increases the risk of difficult tracheal intubation [18-20] or laryngoscopy [21], though others argue the opposite [3, 8, 22]. The airway complications are specifically related to the abdominal type of obesity (also named male-type, android, central, visceral or apple-shaped obesity) identified by the waist to hip ratio-not routinely done in clinical practice [16, 23]. Obese patients have anatomical and physiological changes in both the upper and lower airway that must be taken into consideration for an optimal AM. The relationship between a high BMI and difficult intubation has been described in the literature, few of recent articles concluding that a BMI >35 is associated with a difficult tracheal intubation [20, 24, 25]. Obese patients present an increased fat deposition in pharynx, predisposing the anterior-wall to collapse and developing more airway obstructions [26]. In patients with morbid obesity the accumulation of fat tissue adjacent to the chest wall and the abdomen decreases lung compliance. As a result, the patient experiences physiologic respiratory changes such as reduction in expiratory reserve volume (ERV), functional residual capacity (FRC), and total lung capacity (TLC) [27-29]. The work of breathing is increased due to small airway closure and the increased airway resistance [30-31]. Obese patients have a ventilation/perfusion (V/Q) mismatch caused by the combination of increased perfusion and decreased ventilation of the lower lobes [28, 32]. In addition to the aforementioned changes, increased oxygen consumption and carbon dioxide production accelerate the desaturation process during the endotracheal intubation, requiring the procedure to be carry out as fast as possible [33].
Ultrasound (US) evaluation of the airway is found to be an excellent tool in different medical settings including the operating room, intensive care unit and in the emergency department (ER). The utility of the US in the airway management is not limited to the upper airway assessment; it has been also used to evaluate the lower airway, lungs and pleura [34].
US has many advantages over other alternative techniques to AA, because its financial accessibility and safety. It is a fast method of patient’s evaluation, and does not require extensive training in order to be performed preoperatively [35].
Various studies described different US imaging techniques able to visualize difficult airways and to improve airway management; however, there is no conclusive research accomplished in order to establish US visualization during AM as a standard of care [35]. Currently, the various clinical applications of the US imaging of the upper airway include identification of endotracheal tube (ET) placement, guidance of percutaneous tracheostomy and cricothyroidotomy, detection of subglottic stenosis, prediction of difficulty intubation and post extubation stridor, prediction of pediatric ET and double lumen tubes size [36-40].
D. S. J. Elliot and colleagues evaluated the accuracy of surface land mark identification of the cricothyroid membrane by eighteen anesthetists, and reported that only 32 attempts (30% of anesthetists) accurately marked the skin area over the cricothyroid membrane and only 11 attempts (10% of anesthetists) marked over the center point of the membrane [41]. The most common complication for surgical cricothyroidotomy was incorrect tracheostomy tube placement due to inappropriate identification of anatomical references, thyrohyoid membrane being the most frequent route of the displacement [41-44]. Subcutaneous emphysema, distortion of the neck anatomy and pneumomediastinum are potentially fatal complications that result from failed identification of correct anatomical structures whenever the ventilation is initiated [41, 45]. The mean time to identify the cricothyroid membrane with US is 24.3 seconds, reducing fatal complications and healthcare costs significantly [46].
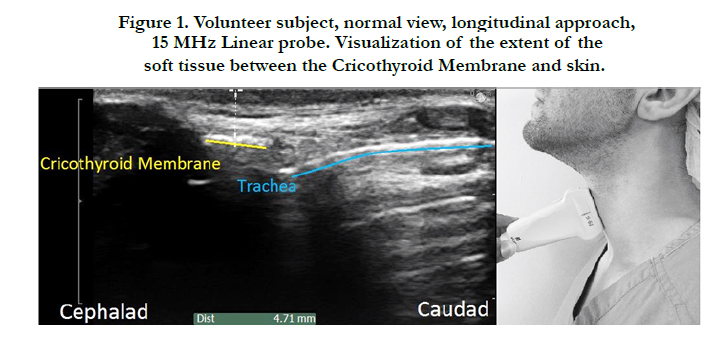
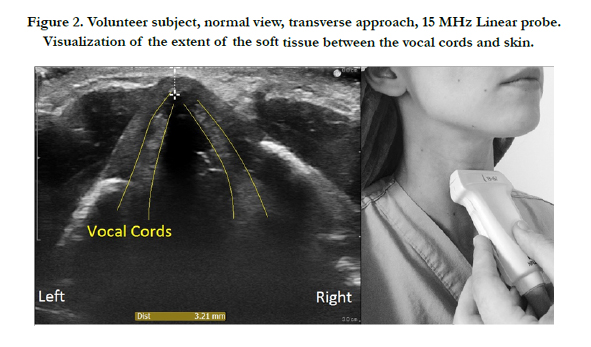
US can also play a role in predicting the difficulty of laryngoscopy in obese patients [21]. Some studies have concluded that pretracheal soft tissue at the level of the vocal cords is a good predictor of difficult laryngoscopy in obese patients. The anterior neck soft tissue thickness assessed by US at hyoid bone, thyrohyoid membrane, and anterior commissure levels could increase the prediction of a difficult laryngoscopy [47]. Patients with more pretracheal soft tissue (28 mm) and a greater neck circumference (50 cm) at the level of vocal cords are at increased risk of difficult intubation [37] (Figure 1-Visualization of the extent of the soft tissue between the Cricothyroid Membrane and skin, and Figure 2-Visualization of the extent of the soft tissue between the vocal cords and skin).

Conclusion
The role of US in AM is commonly underappreciated. More studies are required in order to support the use of US during AM as a standard of care.
US use should be incorporated into anesthesiology and ER residency training requirements, with specific guidelines for difficult AM. US should be routinely used for preoperative assessment of potential DA morbidly obese patients. Obese patients present excessive soft tissue in pre cricoid membrane, making the recognition of anatomic landmarks during cricothyroidotomy very difficult. Ultrasonography provides an accurate identification of the cricothyroid membrane, avoiding fatal complications.
The American Society of Anesthesiology (ASA) guidelines for AM were published in 1993, and have been modified twice since then. Video-assisted laryngoscopy was included in DA algorithm in 2013, demonstrating the qualitative impact of technological progress in patient care.
A fast evolving technology, with lower prices and user friendly machines will play an important role in rediscovering ultrasonography as a beneficial method for diagnosis of potential DA.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial of financial relationships that could be constructed as a potential conflict of interest.
References
- Gupta S, Sharma R, Jain D (2005) Airway assessment: predictors of difficult airway. Indian J Anaesth 49(4): 257-262.
- Benumof JL (1999) The unanticipated difficult airway. Can J Anaesth 46(5 Pt 1): 510-511.
- Baker P (2015) Assessment Before Airway Management. Anesthesiol Clin 33(2): 257-278.
- Woodall NM, Cook TM (2011) National census of airway management techniques used for anaesthesia in the UK: first phase of the Fourth National Audit Project at the Royal College of Anaesthetists. Br J Anaesth 106(2): 266-271.
- Rosenberg MB, Phero JC (2015) Airway Assessment for Office Sedation/ Anesthesia. Anesth Prog 62(2): 74-80.
- Woodall N, Frerk C, Cook TM (2011) Can we make airway management (even) safer?--lessons from national audit. Anaesthesia 66(Suppl 2): 27-33.
- Lauren Berkow M, Carin A Hagberg, Marianna Crowley (2015) Airway management for induction of general anesthesia. UpToDate.
- el-Ganzouri AR, McCarthy RJ, Tuman KJ, Tanck EN, Ivankovich AD (1996) Preoperative airway assessment: predictive value of a multivariate risk index. Anesth Analg 82(6): 1197-1204.
- Shiga T, Wajima Z, Inoue T, Sakamoto A (2005) Predicting difficult intubation in apparently normal patients: a meta-analysis of bedside screening test performance. Anesthesiology 103(2): 429-437.
- Vannucci A, Cavallone LF (2015) Bedside predictors of difficult intubation: a systematic review. Minerva Anestesiol.
- Khan ZH, Mohammadi M, Rasouli MR, Farrokhnia F, Khan RH (2009) The diagnostic value of the upper lip bite test combined with sternomental distance, thyromental distance, and interincisor distance for prediction of easy laryngoscopy and intubation: a prospective study. Anesth Analg 109(3): 822-824.
- Sharma D, Prabhakar H, Bithal PK, Ali Z, Singh GP, et al. (2010) Predicting difficult laryngoscopy in acromegaly: a comparison of upper lip bite test with modified Mallampati classification. J Neurosurg Anesthesiol 22(2): 138-143.
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, et al. (2014) 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 129(25 Suppl 2): S102-138.
- Organization WH (2015) Obesity and overweight: WHO Media centre. www.who.int/mediacentre/factsheets/fs311/en/.
- Centers for Disease Control and Prevention (2012) Division of Nutrition, Physical Activity, and Obesity. Defining Adult Overweight and Obesity.www.cdc.gov/obesity/adult/defining.html.
- Estis G, Segal E (2015) [Airway management in the morbidly obese patient]. Harefuah 154(4): 274-278.
- Butler KH, Clyne B (2003) Management of the difficult airway: alternative airway techniques and adjuncts. Emerg Med Clin North Am 21(2): 259-289.
- Brodsky JB, Lemmens HJ, Brock-Utne JG, Vierra M, Saidman LJ (2002) Morbid obesity and tracheal intubation. Anesth Analg 94(3): 732-736.
- Bond A (1993) Obesity and difficult intubation. Anaesth Intensive Care 21(6): 828-830.
- Lundstrom LH, Moller AM, Rosenstock C, Astrup G, Wetterslev J (2009) High body mass index is a weak predictor for difficult and failed tracheal intubation: a cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology 110(2): 266-274.
- Ezri T, Gewurtz G, Sessler DI, Medalion B, Szmuk P, et al. (2003) Prediction of difficult laryngoscopy in obese patients by ultrasound quantification of anterior neck soft tissue. Anaesthesia 58(11): 1111-1114.
- Wilson ME, Spiegelhalter D, Robertson JA, Lesser P (1988) Predicting difficult intubation. Br J Anaesth 61(2): 211-216.
- George A Bray (2014) Obesity in adults: Prevalence, screening, and evaluation.
- Uribe AA, Zvara DA, Puente EG, Otey AJ, Zhan J, et al. (2015) BMI as a Predictor for Potential Difficult Tracheal Intubation in Males. Front Med 2:38.
- Riess ML, Connolly LA, Woehlck HJ (2009) Body mass index: an illogical correlate of obesity. Anesthesiology 111(4): 920-921.
- Behringer EC (2002) Approaches to managing the upper airway. Anesthesiol Clin North America 20(4): 813-832.
- Lopata M, Onal E (1982) Mass loading, sleep apnea, and the pathogenesis of obesity hypoventilation. Am Rev Respir Dis 126(4): 640-645.
- Piper A, Yee B (2014) Pathogenesis of obesity hypoventilation syndrome. UpToDate.
- Piper AJ, Grunstein RR (2010) Big breathing: the complex interaction of obesity, hypoventilation, weight loss, and respiratory function. J Appl Physiol (1985) 108(1): 199-205.
- Steier J, Lunt A, Hart N, Polkey MI, Moxham J (2014) Observational study of the effect of obesity on lung volumes. Thorax 69(8): 752-759.
- Zerah F, Harf A, Perlemuter L, Lorino H, Lorino AM, et al. (1993) Effects of obesity on respiratory resistance. Chest 103(5): 1470-1476.
- Kessler R, Chaouat A, Schinkewitch P, Faller M, Casel S, et al. (2001) The obesity-hypoventilation syndrome revisited: a prospective study of 34 consecutive cases. Chest 120(2): 369-376.
- Arbelaez C, Bartels S, Brown CA (2014) Emergency airway management in the morbidly obese patient. UpToDate.
- Kristensen MS, Teoh WH, Graumann O, Laursen CB (2014) Ultrasonography for clinical decision-making and intervention in airway management: from the mouth to the lungs and pleurae. Insights Imaging 5(2): 253-279.
- Kristensen MS (2011) Ultrasonography in the management of the airway. Acta Anaesthesiol Scand 55(10): 1155-1173.
- Kundra P, Mishra SK, Ramesh A (2011) Ultrasound of the airway. Indian J Anaesth 55(5): 456-462.
- Terkawi AS, Karakitsos D, Elbarbary M, Blaivas M, Durieux ME (2013) Ultrasound for the anesthesiologists: present and future. The Scientific World Journal 2013: 1-15.
- Ding LW, Wang HC, Wu HD, Chang CJ, Yang PC (2006) Laryngeal ultrasound: a useful method in predicting post-extubation stridor. A pilot study. Eur Respir J 27(2): 384-389.
- Gupta K, Gupta PK, Rastogi B, Krishan A, Jain M, et al. (2012) Assessment of the subglottic region by ultrasonography for estimation of appropriate size endotracheal tube: A clinical prospective study. Anesth Essays Res 6(2): 157-160.
- Kim EJ, Kim SY, Kim WO, Kim H, Kil HK (2013) Ultrasound measurement of subglottic diameter and an empirical formula for proper endotracheal tube fitting in children. Acta Anaesthesiol Scand 57(9): 1124-1130.
- Elliott DS, Baker PA, Scott MR, Birch CW, Thompson JM (2010) Accuracy of surface landmark identification for cannula cricothyroidotomy. Anaesthesia 65(9): 889-894.
- Bair AE, Panacek EA, Wisner DH, Bales R, Sakles JC (2003) Cricothyrotomy: a 5-year experience at one institution. J Emerg Med 24(2): 151-156.
- Brantigan CO, Grow JB Sr. (1976) Cricothyroidotomy: elective use in respiratory problems requiring tracheotomy. J Thorac Cardiovasc Surg 71(1): 72-81.
- McGill J, Clinton JE, Ruiz E (1982) Cricothyrotomy in the emergency department. Ann Emerg Med 11(7): 361-364.
- Patel RG (1999) Percutaneous transtracheal jet ventilation: a safe, quick, and temporary way to provide oxygenation and ventilation when conventional methods are unsuccessful. Chest 116(6): 1689-1694.
- Nicholls SE, Sweeney TW, Ferre RM, Strout TD (2008) Bedside sonography by emergency physicians for the rapid identification of landmarks relevant to cricothyrotomy. Am J Emerg Med 26(8): 852-856.
- Wu J, Dong J, Ding Y, Zheng J (2014) Role of anterior neck soft tissue quantifications by ultrasound in predicting difficult laryngoscopy. Med Sci Monit 20: 2343-2350.





