The effect of an Intravenous Ketamine Infusion on Postherpetic Neuralgia
Ahn EunKyoung1, Kang YhenSeung1*, Choi SuYoun2
1 Department of Anesthesiology and Pain Medicine, National Health Insurance Service, Ilsan Hospital, Ilsan, Korea.
2 Department of Anesthesiology, Yonsei University College of Medicine, Seoul, Korea.
*Corresponding Author
Dr. Yhen Seung Kang, MD
Department of Anesthesiology and Pain Medicine,
National Health Insurance Service,
Ilsan Hospital, 100, Ilsan-ro, Ilsan-donggu, Goyang-si,
Gyeonggi-do, South Korea.
Tel: 82-31-900-0640
Fax: +82-31-900-0344
E-mail: kmsp131@hanmail.net
Article Type : Research Article
Received: June 02, 2015; Accepted: August 11, 2015; Published: August 14, 2015
Citation: Ahn EunKyoung, Kang YhenSeung, Choi SuYoun (2015) The effect of an Intravenous Ketamine Infusion on Postherpetic Neuralgia. Int J Anesth Res. 3(7), 150-153. doi: dx.doi.org/10.19070/2332-2780-1500037
Copyright: Kang YhenSeung© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: About 10~25% patients with herpes zoster suffers from postherpetic neuralgia (PHN). Yet, there is no certain treatment for PHN. Ketamine, an N-methyl-D-aspartate receptor (NMDA) antagonist, plays an important role in the central sensitization. In this aspect, we tried to find out the effect of IV ketamine in herpes zoster patients who suffered from PHN.
Methods: 40 herpes zoster patients with Visual Analogue Scale (VAS) > 5 after the antiviral, antidepressant and nerve block therapy over 4 weeks were enrolled in this study. 50mg of ketamine and 2.5mg of midazolam was mixed in 100mL of normal saline and administered intravenously to the patients for 1 hour. And we compare with the group who did not use IV ketamine by the chart review.
Results: VAS was significantly decreased by approximately 75% after the use of IV Ketamine whereas there was no significant change of VAS after not the use of IV Ketamine.
Conclusions: Use of IV ketamine is beneficial for pain control in treatment of patients with high risk of PHN.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Central Sensitization; Herpes Zoster; Ketamine; NMDA Antagonist; Postherpetic Neuralgia; VAS.
Introduction
Herpes zoster is a disease caused by the reactivation of varicella zoster virus. The inflammation of the dorsal root ganglion or the trigeminal ganglion through this virus can be cured by administration of antiviral agents and analgesics by its degree. However, for those whose inflammation gets serious, it can be led to the denervated pain, and eventually develop into neuralgia [1-5].
According to some reports, the percentage of zoster patients whose symptoms get transformed into neuralgia is 10~25% [5]. Its figure grows by the ages and the decrease of immune function, up to 45% [6].
Recently the IV injection of ketamine [7, 8], pulsed radiofrequency [9], or the intrathecal injection of steroid [10] are used for treating postherpetic neuralgia. Since the method of treatment is very limited, once the zoster transforms into neuralgia, aggressive early treatment is necessary [11].
We performed the survey based on ages, Dermatome of neural invasion, and occurrence of PHN among the outpatients in our hospital. We also would like to find out whether the IV injection of ketamine can be prevent zoster from transformed into PHN, and effectively treating subacute pain among the patients whose pain lasted 1-2 months after the zoster.
Materials and Methods
We focused on 40 patients with the persistent pain more than 4 weeks after neuropathic pain started, among all the patients who were treated for zoster from January 2007 to September 2009 in the our Hospital. Patients with shingles and pain lasts for more than 4 weeks after neuropathic pain started so received ketamine IV infusion was performed the retrospective chart review. We excluded patients who dropped out from the treatment for personal reasons. The Institutional Review Board of our Hospital approved the study protocol (approval date :2014, June, 24 and approval number : 2014-110).
Ages, sex, height, weight of patients were documented, as well as affected dermatome of the outbreak, accompanied allodynia, times and numbers of nerve blocks and Ketamine injections. We set the size of wound at the first treatment as 0% to 100% of skin rash, vesicle or pigmentation at involving dermatome, and at the last treatment. We checked the cold sensory with alcohol setting the normal as 100 and none as 0. We documented the occurrence of PHN by the time of closing the treatment. The severity of pain was documented on 1 week, 2 weeks, 3weeks, 4 weeks, 2 months, and 4 months after the outbreak of pain. The severity of pain before and after the ketamine treatment was also documented using visual analogue scale.
The nerve block such as stellate ganglion block, trigeminal nerve block, C2 ganglion block and epidural block (with & without triamcinolone) were executed according to the involved dermatome. The ketamine injection was made with ketamine 50mg, midazolam 2.5mg and 100mL of saline. It was injected for about an hour while blood pressure and SaO2 monitored every 5minutes. The treatment was stopped if patients complained of headache, or the blood pressure get increased by 20% after the ketamine injection. But this case was rare.
The demographic and clinical data of patients were divided into groups as groups with no PHN, and with PHN then, recorded by mean ± S.D. We used independent samples t-test to analysis the duration of outbreak before nerve block and ketamine injection, each numbers of treatment, sizes of the wound, the rates of sensory loss, and the severity of pains within 1week to 4months. Based on this data, we compared the statistical similarity between no PHN and PHN groups. The correlation between all these data and the outbreak of PHN among all the targeted patients were examined using Pearson’s correlation analysis. We defined P-value 0.05 as a statistical similarity.
Results
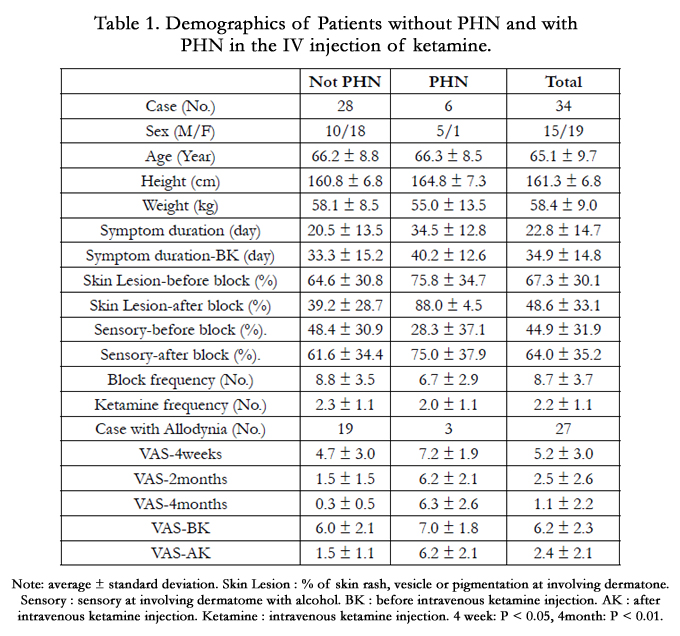
The enrolled patients were 19 males and 21 females, and the average ages were 66.1 ± 9.7 years. Four month later of treatment, PHN patients sustained with pain were 6, No PHN patients recovery from pain were 28 and patients with follow up loss at 3,4 month later of treatment were 6. The ratio of fully recovered patients from PHN among the female group (18 among 19) was statistically significant, but age, height, and weight were not the statistically significant factors. The average of the duration before the treatment was 34.9 ± 14.8 days (min 3 days~max 60 days), and there were no statistical significant difference between two groups regarding durations and the timing of ketamine injection.
Patients with allodynia prior to the treatment were 27 (67.5%), and there was no statistical difference between two groups, as well as the numbers of nerve block and Ketamine injection (each 8.7 ± 3.7 and 2.2 ± 1.1). The cold sensory to alcohol at the first and the last treatment got decreased (each 8.7 ± 3.7 and 2.2 ± 1.1) for the standard of Alcohol swap. The sizes of wounds were 64.3% and 48.6% each. The size of wound among PHN at the last stage of treatment was 88.0%, which was significantly bigger than that of fully recovered group, 39.2% (P < 0.01).
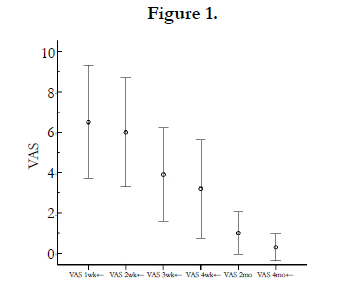
The severity of pain tended to get decreased as a week went by after the outbreak (Figure 1); As the sizes of wounds got bigger at the last stage of treatment, the severity of pain at 4 weeks and 3 months got significantly higher (4 weeks: P < 0.05, 4 months: P < 0.01).
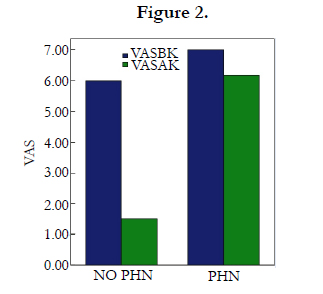
Before and after the ketamine injection, the severity of pain (VAS score) among the fully recovered group were 6.0 ± 2.1 and 1.5 ± 1.1 respectively while those of the PHN group were 7.0 ±1.0 and 6.2 ± 2.1 (Figure 2).
Ages, duration, the time of the first block, allodynia, the severity of pain at the early stage of the outbreak, and the rates of sensory loss had no relevance to the progress of PHN (P > 0.05, Table1).

Discussion
PHN is one of the common intractable chronic pain syndrome, meaning pain lasts even after treating skin rash. It is controversial to define when PHN starts, 1, 3, 4, and 6 months after appearing or disappearing skin rashes. However, it is predominant to define PHN if pain lasted 30 days even after the disappearing skin rashes [12, 13].
Numbers of mechanism can be involved in evolving PHN, those can affect one patient simultaneously or over the course of time. Maybe it can explain all the different types of pain 17 weeks after the outbreak. The involvement of the central nerve system is the reason why it is important to treat at the early stage [14-17].
It is reported that PHN can be occurred frequently if the patients had underline disease such as diabetes or cancer, and by ages, the size of wound at the early stage, and severity of pain [6, 18, 19]. In this research, the size of wound at the final stage of treatment, which was after 4 month, rather than size of wound at the early stage, had relation with the occurrence of PHN. It shows that the size of the wound after 4 months, which leaves scar such as pigmentation, can be a strong prediction factor, rather than the total size of wounds. The bigger the size of scar and the severity of pain also can be the prediction factor [20]. The reason why we excluded diabetes and cancer as a prediction factor in this research was that much larger patients group than ours should be required to gain more accurate result.
Originally, Ketamine was an anesthetic but recently it’s known to help neuropath; pain. Hocking and other claimed that the effect of ketamine for treating chronic pain was weak or moderate, but it could be used as the third treating option for the patients with chronic pain who failed to be cured [7]. ketamine plays a key role in central sensitization as NMDA antagonist [21, 8]. We experienced the decrease of pain for the patients with constant pain 4 weeks after the outbreak. We assumed it could be effective to prevent PHN by injecting Ketamine around 4 weeks of the outbreak.
Conclusion
It can be helped to inject Ketamine to prevent PHN, especially in case of using classical treatment such as injecting antiviral agents or steroid nerve block cannot decrease the pain. However, we recommend further study regarding perfect timing for Ketamine injection.
References
- Hope-Simpson RE (1954) Studies on shingles: is the virus ordinary chicken pox virus? Lancet 267(6852): 1299-1302.
- Weller TH, Witton HM, Bell EJ (1958) The etiologic agents of varicella and herpes zoster: isolation, propagation, and cultural characteristics in vitro. J Exp Med 108(6): 843-868.
- Straus SE, Reinhold W, Smith HA, Ruvechan WT, Henderson DK, et al. (1984) Endonuclease analysis of viral DNA from varicella and subsequent zoster infections in the same patient. N Engl J Med 311(21): 1362-1364.
- Weller TH (1995) Varicellar-zoster virus: history, perspectives, and evolving concerns. Neurology 45(12 Suppl 8): S9-10.
- Hope-Simpson RE (1965) The nature of herpes zoster: a long-term study and a new hypothesis. Proc R Soc Med 58: 9-20.
- Loeser JD (1986) Herpes zoster and postherpetic neuralgia. Pain 25(2): 149-164.
- Hocking G, Cousins MJ (2003) Ketamine in chronic pain management: An evidence-based review. Anesth Anlg 97(6): 1730-1739.
- Hoffmann V, Coppejans H, Vercauteren M, Adriaensen H (1994) Successful treatment of postherpetic neuralgia with oral Ketamine. Clin J Pain 10(3): 240-242.
- Kim YH, Lee CJ, Lee SC, Huh J, Nahm FS, et al. (2008) Effect of pulsed radiofrequency for postherpetic neuralgia. Acta Anaesthesiol Scand 52(8): 1140-1143.
- Abram SE (1999) Intrathecal steroid injection for postherpetic neuralgia: What are the risks? Reg Anesth Pain Med 24(4): 283-285.
- Bonezzi C, Demartini L (1999) Treatment options in postherpertic neuralgia. Acta Neurol Scand 100(s173): 25-35.
- Arani RB, Soong SJ, Weiss HL, Wood MJ, Fiddian PA, et al. (2001) Phase –Specific analysis of Herpes Zoster associated pain data: a new statistical approach. Stat Med 20(16): 2429-2439.
- Dworkin RH, Portenoy RK (1994) Proposed classification of Herpes Zoster pain. Lancet 343(8913): 1648.
- Robert WJ, Robert HD (2003) Treatment of herpes zoster and postherpetic neuralgia. BMJ 326: 748-756.
- Dworkin RH, Johnson RW, Breuer J, Gnann JW, Levin MJ, et al. (2007) Recommendations for the management of Herpes zoster. Clin Infect Dis 44(Suppl 1): S1-26.
- Cunningham AL, Breuer J, Dwyer DE, Gronow DW, Helme RD, et al. (2008) The prevention and management of herpes zoster. Med J Aust 188(3): 171-176.
- Ji G, Niu J, Shi Y, Hou L, Lu Y, et al. (2009) The effectiveness of repetitive paravertebral injections with local anesthetics and steroids for the prevention of postherpetic neuralgia in patients with acute herpes zoster. Anesth Analg 109(5): 1651-1655.
- Weinberg JM (2007) Herpes zoster: epidemiology, natural history, and common complications. J Am Acad Dermatol 57(6 Suppl): S130-S135.
- Thomas SL, Hall AJ (2004) What does epidemiology tell us about risk factors for herpes zoster? Lancet Infect Dis 4(1): 26-33.
- Ahn EK, Yang JY, Cho JG, Kim J, Chon S, et al. (2004) Significance of Infrared Thermal Imaging in Herpes Zoster patients. Korean J Anesthesiol 47(4): 505-515.
- Rabben T, Skjelbred P, Oye I (1999) Prolonged analgesic effect of ketamine, an N-methyl-D-aspartate receptor inhibitor, in patients with chronic pain. J Pharmacol Exp Ther 289(2): 1060-1066.





