The Effect of Intravenous Fentanyl and Bupivacaine Infiltration on the Hemodynamic Respons During Mayfield Skull Clamps Fixation in Neurosurgery
Morina Q1*, Morina A2, Bunjaku D1, Kelmendi F2, Matoshi D1, Mekaj A2
1 Anesthesiologyst, Anesthesiology Clinic and Intensive Care Unit, University Clinical Center of Kosova Prishtina, Kosova.
2 Neurosurgeon Clinic of Neurosurgery University Clinical Center of Kosova Prishtina, Kosova.
*Corresponding Author
Qamile Morina, PhD,
Anesthesiologyst, Anesthesiology Clinic and Intensive Care Unit,
University Clinical Center of Kosova Prishtina, 10000 Kosova.
Tel: +37744155727
E-mail: qamilemorina00@gmail.com
Received: April 23, 2016; Accepted: July 04, 2016; Published: July 15, 2016
Citation: Morina Q, Morina A, Bunjaku D, Kelmendi F, Matoshi D (2016) The Effect of Intravenous Fentanyl and Bupivacaine Infiltration on the Hemodynamic Respons During Mayfield Skull Clamps Fixation in Neurosurgery. Int J Anesth Res. 4(7), 290-293.DOI : dx.doi.org/10.19070/2332-2780-1600061
Copyright: Morina Q© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The aim of our study was to compare the effects of three techniques for preventing the hypertensive response to the insertion of Mayfield skull pins (MSP): group F (fentanyl), group B (bupivacaine) and FB (combined fentanylbupivacaine).
Material and Methods: A hundred and eight patients scheduled to undergo craniotomy were randomly divided into three groups. Patients whose conditions of their current medication that might affect the stability of hemodynamic were excluded. Gr. F (n=36) received 2 mcg/kg fentanyl i.v. 5 min. before placement of MSP, group B (n=36) after induction the skin areas for the each pin were infiltrated with 3ml 0.5% bupivacaine. After an interval of 3 min the pins were inserted. In gr FB (n=36) both methods were applied together. All patients were given a TIVA with propofol and fentanyl. Blood pressure and heart rate-HR were recorded at five preset times: 1. after induction 2. at the onset of local anaesthesia 3. at the insertion of pin holder 4. 120 sec. and 5.240 sec after insertion. The measurements were compared with the immediate pre insertion values.
Conclusion: Our results suggest that a significant reduction of the hemodynamic effects caused by insertion of the MSP can be achieved by the use of combined intravenous fentanyl and bupivacaine infiltration. Total TIVA alone with propofol and fentanyl cannot protect against these hemodynamic stimuli.
2.Introduction
3.Materials and Methods
3.1.Statistical analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Pain; Fentanyl; Bupivacaine.
Introduction
Pin-holder application for skull fixation in craniotomy patients is common in clinical practice. The Mayfield Skull Clamp is a cranial stabilization device which allows the neurosurgeon to position the skull pins in critical areas [1-5]. Pin insertion causes pain and this is associated with hemodynamic changes as are hypertension, rise of heart rate and increase in cerebrospinal fluid pressure [2-4]. Such changes in hemodynamic can be detrimental for patients with intracranial hypertension, intracranial aneurysms, cardiac diseases, especially for the patients with compromised intracranial compliance [1, 2].
Use of local anesthetic infiltration has shown that prevent this hemodynamic response [1, 2, 6].
The aim of our study was to compare the effects of three techniques for preventing the hypertensive response to the insertion of Mayfield skull pins (MSP): group F (fentanyl), group B (bupivacaine) and FB (combined fentanyl-bupivacaine).
Materials and Methods
After approval of the local Ethics Committee and obtaining written informed consent, 108 patients, ASA classification I-II, aged 30- 62 years, of both sexes, 67 males and 41 females, were included in the study. Patients whose conditions of their current medication that might affect the stability of hemodynamic were excluded. Exclusion criteria were patients who takes antihypertensive medications, patients with cardiac, renal and hepatic disease and those patients which undergoing reoperations.
All patients about an hour before surgery were pre medicated with midazam p.o. All patients were given a TIVA with propofol and fentanyl. Intra operative monitoring included non invasive blood pressure, electrocardiogram, heart rate, SpO2 and end tidal CO2.
A hundred and eight patients scheduled to undergo elective craniotomy were randomly divided into three groups. Group F (n=36) received 2 mcg/kg fentanyl i.v. 5 min. before placement of MSP, group B (n=36) after induction the skin areas for the each pin were infiltrated with 3ml 0.5% bupivacaine. After an interval of 3 min the pins were inserted. In group FB (n=36) both methods were applied together. Blood pressure and heart rate were recorded at five preset times. The measurements were compared with the immediate pre insertion values.
Data processing was done with the statistical package Instat 3. Data are expressed as arithmetic mean and standard deviation. The data obtained are presented in tables and graphs. Testing of quantitative data that had normal distribution is done with One Way ANOVA and Tukey - Kramer Multiple comparison test, and testing of data that didn’t have normal distribution is done with the Kruskal Wallis test and Dunn's Multiple Comparison test for comparison between groups. The difference is significant if P value is less than 0.05.
Results
The three groups were compared for their baseline heart rate and mean arterial pressure, were recorded at five preset times: 1) After induction; 2) At the onset of local anaesthesia; 3) At the insertion of pin holder; 4) 120sec. after insertion; and 5) 240sec after insertion; and those hemodynamic recordings were comparable.
In Group F the mean arterial pressure (MAP) measured in Induction was 81.3mmHg (SD± 6.5mmHg), after onset of local anesthesia MAP was 80.9 mmHg (SD±4.6 mmHg), upon insertion of Mayfield skull pins (MSP), MAP was 119.8 mmHg (SD±5.5 mmHg), 2 minutes after insertion it was 113.4 mmHg (SD±5.8 mmHg) and four minutes after insertion MAP was 93.3 mmHg (SD ± 6.3mmHg). Between the blood pressure values measured at different times of the F group we have earned the distinction with important statistical significance (P < 0.0001) have had an increase in blood pressure upon insertion of the MSP. (Table 1 and Figure 1)
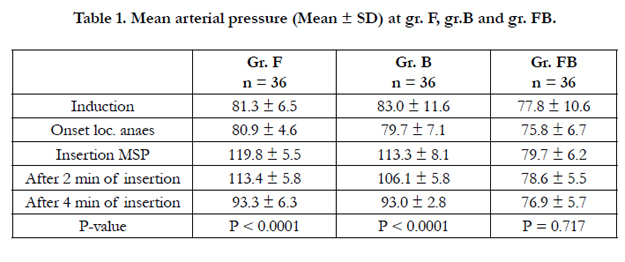

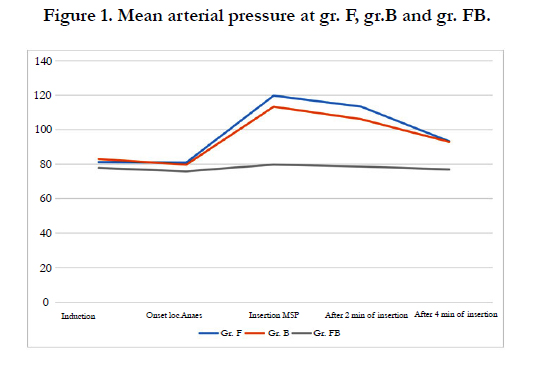
In Group B the mean arterial pressure (MAP) measured in Induction was 83.0mmHg (SD± 11.6mmHg), after onset of local anesthesia MAP was 79.7mmHg (SD±7.1mmHg), upon insertion of Mayfield skull pins (MSP), it was 113.3 mmHg (SD±8.1 mmHg), 2 minutes after insertion it was 116.1mmHg (SD±5.8 mmHg) and four minutes after insertion MAP was 93.0 mmHg (SD ±2.8mmHg). Between the blood pressure values measured at different times of the B group we have earned the distinction with important statistical significance (P<0.0001) have had an increase in blood pressure upon insertion of the MSP. (Table 1 and Figure1)
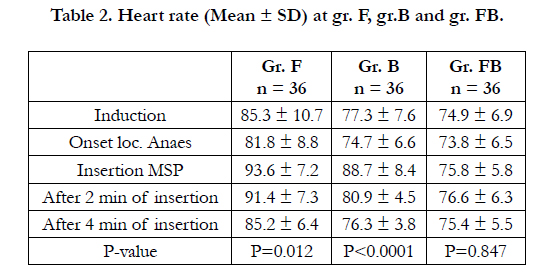
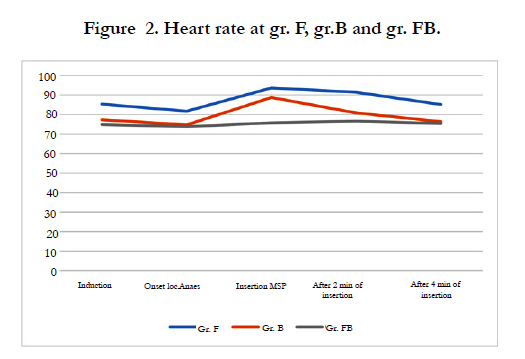
In Group FB the mean arterial pressure (MAP) measured in Induction was 77.8mmHg (SD ± 10.6mmHg), after onset of local anesthesia MAP was 75.8mmHg (SD±6.7 mmHg), upon insertion of Mayfield skull pins (MSP), MAP was 79.7 mmHg (SD±6.2mmHg), 2 minutes after insertion it was 78.6 mmHg (SD ± 5.5 mmHg) and four minutes after insertion MAP was 76.9 mmHg (SD ± 5.7 mmHg). Between the blood pressure values measured at different times of the FB group we have not earned the distinction with important statistical significance (P > 0.05) have had an increase in blood pressure upon insertion of the MSP. Mean arterial pressure remained stable all the time (Table 1 and Figure 1). In Group F the mean heart rate per minute measured in Induction was 85.3 (SD ± 10.7) beats/min, after onset of local anesthesia it was 81.8 (SD ± 4.6)/min, upon insertion of Mayfield skull pins (MSP) 93.6 (SD ± 7.2)/min, 2 minutes after insertion it was 91.4 (SD±7.3)/min and four minutes after insertion was 85.2 (SD ±6.4)/min. Between the heart rate values measured at different times of the F group we have earned the distinction with important statistical significance (P < 0.05) have had an increase in heart rate upon insertion of the MSP. (Table 2 and Figure 2)
In Group B the mean heart rate per minute measured in Induction was 77.3 (SD± 7.6) beats/min, after onset of local anesthesia it was 74.7 (SD±6.6)/min, upon insertion of Mayfield skull pins (MSP) was 88.7 (SD±8.4)/min, 2 minutes after insertion it was 80.9 (SD±4.5)/min and four minutes after insertion was 76.3 (SD ±3.8)/min. Between the heart rate values measured at different times of the B group we have earned the distinction with important statistical significance (P < 0.0001) have had an increase in heart rate upon insertion of the MSP. (Table 2 and Figure 2)
In Group FB the mean heart rate per minute measured in Induction was 74.9 (SD ± 6.9) beats/min, after onset of local anesthesia it was 73.8 (SD ±6.5)/min, upon insertion of Mayfield skull pins (MSP) it was 75.8 (SD ± 5.8)/min, 2 minutes after insertion it was 76.6 (SD ± 6.3)/min and four minutes after insertion was 75.4 (SD ± 5.5)/min. Between the heart rate values measured at different times of the FB group we have not earned the distinction with important statistical significance (P >0.05), we have had a stable heart rate all the time. (Table 2 and Figure 2)
Discussion
Hemodynamic responses during pain insertion may lead to brain edema and increase in intracranial pressure. Different anesthetic and pharmacologic techniques, including local anesthetics, narcotics, anti hypertensive drugs and deepening of anesthesia, have been used to blunt this deleterious effect with variable success [3, 4, 7-11].
Ozköse et al in their comparison of intravenous fentanyl 2 mcg/ kg, 5 minutes before pinning and intravenous fentanyl 2 mcg/ kg with local infiltration of 1% lidocaine, have shown that a combination of both the intravenous fentanyl and local infiltration was more effective than either one of them alone in reducing the hemodynamic response to Mayfield head holder placement [6]. Schaffranietz et al have suggested that a significant reduction of the hemodynamic effects caused by insertion of the Mayfield skull clamp can be achieved by the use of local anesthesia and that total intravenous anesthesia alone with propofol and alfentanil cannot protect against these hemodynamic stimuli [9].
Many studies have suggested that local infiltration at the pin site provides sufficient analgesia and hemodynamic stability at the time of pin insertion [1-3, 6-8, 11]. Lidocaine as a local anesthetic, when combined with adrenaline, doubles its duration of action due to the vasoconstrictor effects of adrenaline, which limits its systemic absorption. Despite being an antiarrhythmic, when used as a local anesthetic, has very little potential side effects,especially when used with adrenaline. Infiltration of the scalp with lidocaine and adrenaline before pin insertion was found to prevent hemodynamic changes effectively [1]. Rubial et al., performed regional blockade of the occipital and frontal nerves and found it to be a useful method for maintaining hemodynamic stability during craniostate placement [10]. Geze et al in their study conclude that not only does the scalp block with 0.5% bupivacaine attenuate the hemodynamic response to the scalp pin insertion, it also decreases the stress hormone levels (cortisol and ACTH) better than routine anaesthesia or scalp infiltration with bupivacaine and should be considered in conjunction with general anaesthesia for craniotomy [4]. Zohry et al in their study shown that in craniotomy patients, local infiltration of the scalp with lidocaine 2% at the sites of pin insertion attenuated pain-induced hemodynamic and CBFVMCA (cerebral blood flow velocity in the middle cerebral artery) changes during pin application while prior administration of fentanyl (1μg/kg) failed to achive this effect, and this effect can be of particular importance in patients with critically compromised intracranial compliance [2]. Fentanyl was found to be effective in blood pressure after pin insertion, but the required dose was relatively large (4.5μg/kg) and resulted in bradycardia and/or hypotension [12].
In our study we demonstrate that hemodynamic changes that occur during pin insertion in craniotomy surgery can be kept under control by infiltration of the scalp with local anesthetics as bupivacaine and intravenous fentanyl.
Conclusion
Our results suggest that a significant reduction of the hemodynamic effects caused by insertion of the MSP can be achieved by the use of combined intravenous fentanyl and bupivacaine infiltration. Total TIVA alone with propofol and fentanyl cannot protect against these hemodynamic stimuli.
References
- Ayesha Arshad, Muhammad Shahzad Shamim, Muhammad Waqas, Hina Enam, Sayed Ather Enam (2013) How effective is the local anesthetic infiltration of pin sites prior to application of head clamps: A prospective observational cohort study of hemodynamic response in patients undergoing elective craniotomy. Surg Neurol Int 4: 93. 10.4103/2152-7806.115237.
- Gomaa Zohry, Hazem Hosny, Dalia Nabil, Mona T. El-Ghoneimy (2006) Lidocaine Infiltration versus Intravenous Fentanyl for Preventing the Hemodynamic Response to Pin Insertion in Craniotomy Patients: A Transcranial Doppler study 43(1)
- Yildiz K, Madenoglu H, Dogru K, Kotanoglu MS, Akin A, et al., (2005) The effects of intravenous fentanyl and intravenous fentanyl combined with bupivacaine infiltration on the hemodynamic response to skull pin insertion. J Neurosurg Anesthesiol 17(1): 9-12.
- Geze S, Yilmaz AA, Tuzuner F (2009) The effect of scalp block and local infiltration on the haemodynamic and stress response to skull-pin placement for craniotomy. Eur J Anaesthesiol 26(4): 298-303. doi: 10.1097/EJA.0b013e32831aedb2.
- Doblar DD, Lim YC, Baykan N, Frenette L (1996) A comparison of alfentanil, esmolol, lidocaine, and thiopental sodium on the hemodynamic response to insertion of headrest skull pins. J Clin Anesth 8(1): 31-35.
- Ozköse Z, Yardim S, Yurtlu S, Doğulu F, Kaymaz M, Paşaoğlu A (2001) The effects of intravenous fentanyl and lidocaine infiltration on the hemodynamic response to skull pin placement. Neurosurg Rev 24(1): 35-37.
- Smith FJ, van der Merwe CJ, Becker PJ (2002) Attenuation of the haemodynamic response to placement of the Mayfield skull pin head holder: alfentanil versus scalp block. Southern African Journal of Anaesthesia & Analgesia 8(4). 10.1080/22201173.2002.10872972.
- Pinosky ML, Fishman RL, Reeves ST, Harvey SC, Patel S, et al., (1996) The effect of bupivacaine skull block on the hemodynamic response to craniotomy Anesth Analg 83(6): 1256-1261.
- Schaffranietz L, Rüffert H, Trantakis C, Seifert V (1999) [Effect of local anesthetics on hemodynamic effects during Mayfield skull clamp fixation in neurosurgery using total intravenous anesthesia]. Anaesthesiol Reanim 24(2): 51-54.
- Rubial M, Castells MV, Gargallo MC, Madrid JL (1992) Regional blockage for arterial blood pressure control during placement of head holder in neurosurgery Rev Esp Anestesiol Reanim 39(5): 282-284.
- Mathieu D, Beaudry M, Martin R, McLelland H, Robert B, et al., (1992) Effect of the local anesthetic agent bupivacaine prior to application of the skull-pin holder for craniotomies. J Neurosurg 98(6): 1194–1197.
- Jamali S, Archer D, Ravussin P, Bonnafous M, David P, et al., (1997) The effect of skull-pin insertion on cerebrospinal fluid pressure and cerebral perfusion pressure: influence of sufentanyl and fentanyl Anesth Analg 84(6):1292-1296.





