Effectiveness of AccuVein AV400 Device versus ultrasound-guided Cannulation of the Great Saphenous vein at the Ankle in Infants: A Randomized Controlled Trial
Rehab Abd El- Raof Abd El -Aziz*, Yasser Mohamed Osman*
Assistant Professor, Department of Anesthesia and Surgical Intensive Care, Egypt.
Faculty of Medicine, Alexandria University, Egypt.
*Corresponding Author
Rehab Abd El-Raof Abd El -Aziz,
Assistant Professor, Department of Anesthesia and Surgical Intensive Care, Egypt.
Faculty of Medicine, Alexandria University, Egypt.
Tel/Fax: 01001073703
E-mail: trcium2002@yahoo.com
Received: April 10, 2020; Accepted: April 29, 2020; Published: April 30, 2020
Citation: Rehab Abd El-Raof Abd El -Aziz, Yasser Mohamed Osman. Effectiveness of AccuVein AV400 Device versus ultrasound-guided Cannulation of the Great Saphenous vein at the Ankle in Infants: A Randomized Controlled Trial. Int J Anesth Res. 2020;8(3):594-599. doi: dx.doi.org/10.19070/2332-2780-20000118
Copyright: Rehab Abd El-Raof Abd El -Aziz© 2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: In pediatric patients, peripheral venous access can be very difficult and repeated attempts may be needed. Several devices have been developed to facilitate venous cannulation. Some of them used the near-infrared rays reflecting system for venous visualization. Other used ultrasound to perform venous cannulation. The primary goal was to investigate the practicability of ultrasound-guided vascular access versus AccuVein AV 400 for cannulation of great saphenous vein at the level of the medial malleoli in infants ≤12 months.
Methods: Prospective, double blinded and randomized study on eighty patients in each group. ASA I and II Infants’ ≤12 months were enrolled in the study. Infants were randomly assigned into two groups; an AV400 group and an ultrasound guided group .The observer recorded the time of tourniquet application, the time of successful cannulation and the number of cannulation attempts. The puncture site was evaluated to detect possible hematoma or local infection.
Results: There was significant statistical difference in cannulation time and tourniquet time between the two groups. In ultrasound group, mean time for tourniquet was 54.05 ± 26.7 seconds and for AV400, it was 33.95 ± 19.1 seconds. As regard the cannulation time, the mean time in the ultrasound group was 41.4 ± 24.9 seconds and it was 25.1 ± 17.8 seconds in the AV400 group.
Conclusion: AccuVein 400 and ultrasound-guided vascular access in infants ≤12 months are a promising techniques to be used in pediatric anesthesia. But with the AccuVein 400 the time of tourniquet and cannulation was shorter than with the use of the ultrasound.
2.Introduction
3.Materials and Methods
4.Results and Discussions
5.Acknowledgement & Declarations
6.Conclusion
7.References
Keywords
AccuVein AV400; Ultrasound-Guided; Great Saphenous Vein; Infants.
Introduction
Peripheral venous cannulation is essential during anesthesia for infants undergoing surgeries [1]. It is the commonest root used for perioperative administration of drugs and fluids. In the pediatric age group, the peripheral venous access can be very difficult and repeated attempts may be needed to establish an acceptable venous line [2, 3]. Catheterization of veins in the dorsal network of the hands and feet are usually selected as they are the most visible or at least palpable veins especially in infants and pediatric patients. On the other hand, the dorsal network veins may be very small, invisible or impalpable due to pre-operative dehydration or thick subcutaneous tissue [4]. The peripheral venous cannulation in these cases can be difficult and time-consuming [5]. There are several methods to facilitate the peripheral venous cannulation in these cases such as local warming, epidermal nitroglycerine, translumination, and venous cut down [6-8]. However, many of these methods are rarely used and may be time consuming. The use of Ultrasonography to guide peripheral vein catheterization in children is an easy and non-invasive technique especially for challenging veins [9]. Using ultrasound in peripheral veins cannulation in infants may be very difficult as most of the peripheral veins are too superficial and too small for direct visualization with standard ultrasound equipment [4, 10]. An alternative choice to the superficial dorsal veins could be the great saphenous vein (GSV) at the level of the medial malleolus due to the adequate diameter and the relatively deep position relative to the skin [1]. Nowadays, several devices have been developed with near-infrared rays (NIR)-reflecting system for venous visualization [11-13]. NIR can be transmitted through the subcutaneous tissue and is absorbed by hemoglobin in the blood [14-16]. The AccuVein AV400 (AccuVein Inc., Huntington, New York, United States) device which detects the hemoglobin in the vessels by red and infrared light reflection is one of these devices as it shows the vasculature map by reflecting light [17, 18]. The primary goal of the present study was to investigate the practicability of ultrasound-guided vascular access versus the AccuVein AV 400 for cannulation of the great saphenous vein at the level of the medial malleoli in infant’s ≤12 months.
This prospective, randomized study was conducted from September 2019 till January 2020; eighty patients were allocated and statistically analyzed in each group after examining 263 patients and excluding patients how did not meet the inclusion criteria or failure of the cannulation procedure. The clinical trial took place at the Alexandria Main University Hospital after approval of the Medical Ethics Committee. Informed written consent was obtained from the patient’s parents. Infants’ ≤12 months with ASA physical status I and II, undergoing elective surgery with no visible veins at the dorsum of the hands or feet were enrolled in the study. Exclusion criteria were parental refusal, previous cannulation attempts of the great saphenous vein, or hemodynamic instability.
It was registered at ClinicalTrials.gov (NCT04164862). Infants were randomly assigned, by using a block of randomization provided by www.randomization.com, into two groups; an AV400 group (using the AccuVein AV400 for peripheral venous insertion) and an ultrasound guided group (using the ultrasound for peripheral venous insertion). The cannulation was done by expert anesthetists, having a minimum of 5 times experience in ultrasound guided IV cannula insertion and with the AccuVein AV400 device.
Preoperatively for all infants, the medial malleolar areas in both legs were prepared with EMLA cream. 1 mg/ kg rectal midazolam (maximum dose 15 mg) was given 30 minutes preoperatively. Establishment of standard monitoring (SpO2, ECG, non-invasive arterial pressure) and then induction of general anesthesia was done via a face mask with sevoflurane FIO2 40% - O2/air and after successful induction of general anesthesia, the EMLA tapes were removed. Assisted ventilation via the face mask was done until establishment of venous access either through using Acc Vein AV400 or through ultrasound guided for the great saphenous vein.
On each occasion, the observer recorded the time of tourniquet application, the time of successful cannulation and the number of cannulation attempts. A cannulation attempt was defined as any backward and forward movements of the needle, regardless of whether the needle was out of the skin. Successful cannulation was defined by the absence of tissue swelling around the puncture point after injection of five ml of crystalloid solution. In both groups, a maximal number of three attempts for establishment of venous access in one GSV were performed. If the third attempt failed, the contra lateral GSV was punctured. If successful establishment of venous access in the contra lateral GSV failed, the case was counted as failure. In these cases, the external jugular vein was used as an alternative approach for venous access. After successful establishment of venous access, the anesthetic procedure was continued depending on surgical requirements. Twentyfour hours after establishment of the venous access, the puncture site was evaluated to detect possible hematoma or local infection.
Data were analyzed using SPSS software package version 20.0. Qualitative data were described using number and percent. Qualitative data were described using rang (minimum and maximum), mean and standard deviation. Significance of the obtained results was judged at the 5% level. T-test was used to compare betweenboth groups. Chi-square test was used for categorical variables. A value of P<0.05 was considered statistically significant.
was done using Med Calc statistical software. A minimum sample size of 50 patients in each group was determined based on the success rate of cannulation using ultrasound. Type I and type II errors (α 0.05, β 0.2). The power of the study was 90.0%. The actual sample size included all the patients recruited during the study period of 6 month (160 patients).
After examining 263 infants and excluding infants who did not meet the inclusion criteria or failure of the cannulation procedure; eighty patients were allocated and statistically analyzed in each group as shown in the flow chart (Figure 1). Not all the patients who started the study completed it successfully. There was no statistical difference as regard the sex of the patients in both groups the females constituted about 43.75% of the patients tested in (AV400) group and 46.25% in (ultrasound) group with a p valve of 0.75.
The cannulation success rate was 87.912% with ultrasound method and 93.023% using the AV400 device with a p value of 0.241denoting no statistical difference between them. The numberof skin punctures till cannulation success or failure were not significantly different between both groups (p-value = 0.094) (Table 1).
On the other hand, there was significant statistical difference in the cannulation time and tourniquet time between the two groups of the study. In the ultrasound group, the mean time for tourniquet was 54.05 ± 26.7 secondswhile for the group using the AV400 device 33.95 ± 19.1 seconds. By Comparing between the two groups, it was found that the mean time for tourniquet was statistical significantly lower when using the AV400 device in cannulation with a P value of <0.001. As regard the cannulation time, it was also statically lower when using the AV400 device. With a mean time of 25.1 ± 17.8 seconds compared to 41.4 ± 24.9 seconds when using ultrasound and the P value was <0.001.
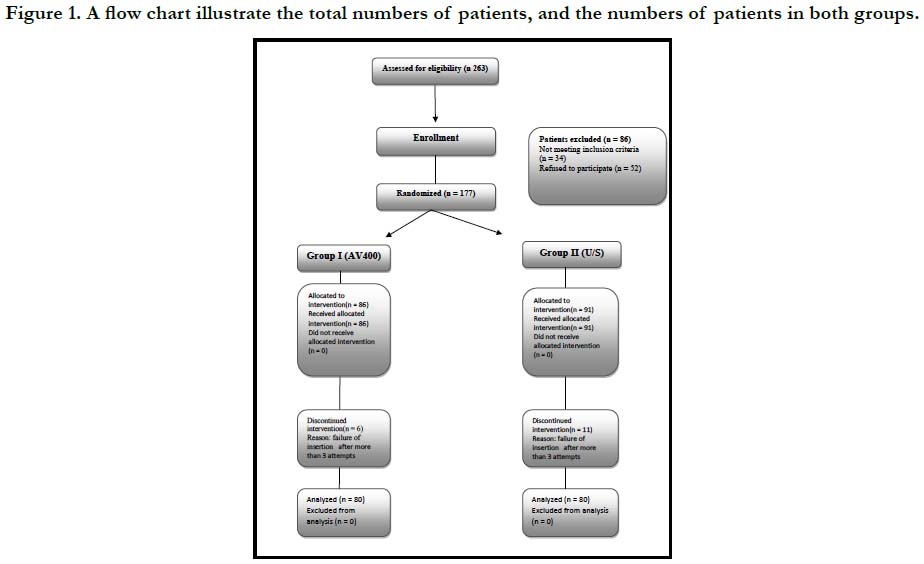

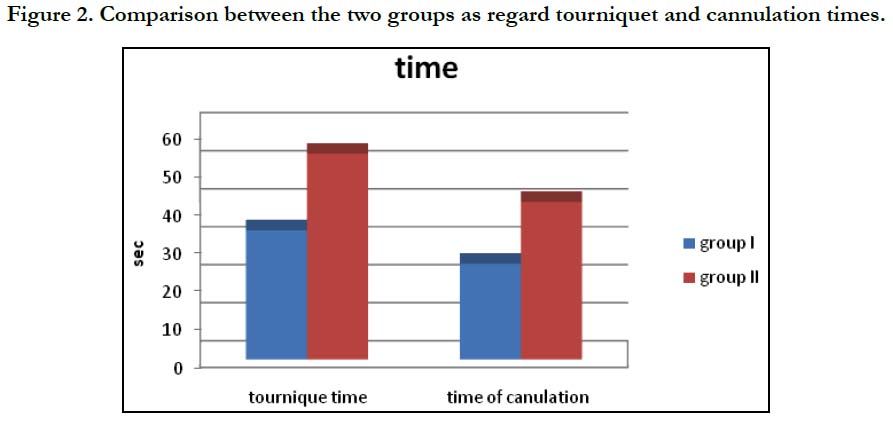

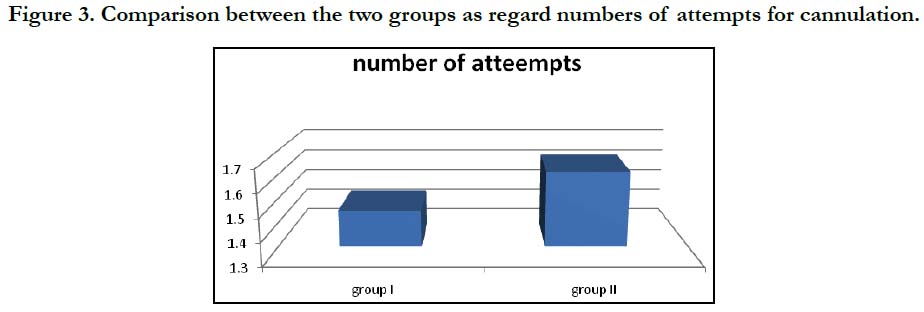
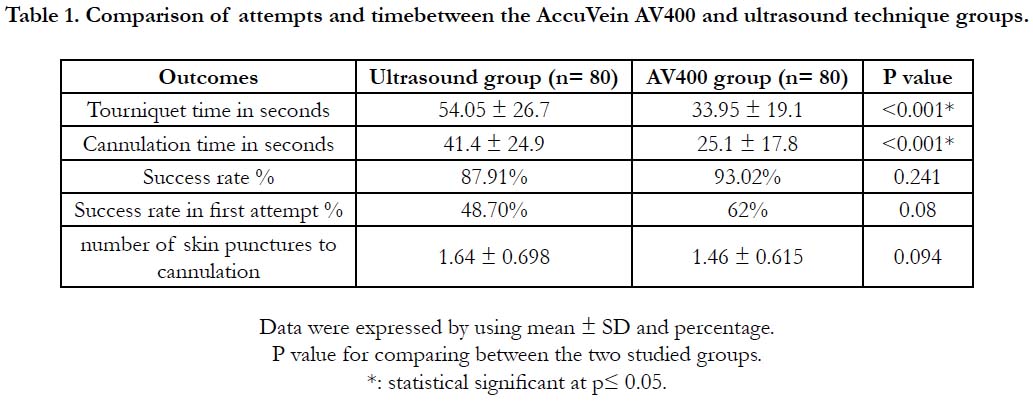

Table 1. Comparison of attempts and timebetween the AccuVein AV400 and ultrasound technique groups.
In this study, we found no significant difference between using the AccuVein AV400 device and the ultrasound guided technique in the success rate of GSV cannulation in infants’ ≤ 12 months as p value was 0.241. As regard the number of skin punctures till successful cannulation, there was no difference between the two groups as p-value equaled to 0.094. But, the time for successful cannulation using the AV400 device was significantly shorter than when using the ultrasound with P value <0.001. these findings suggest that cannulation of the GSV in infants is easer and much faster when using the AccuVein AV400 device but have the same success rate of the ultra sound when used for the cannulation. This suggestion is also supported by the significant shorter Tourniquet time demonstrated in this study.
Unfortunately no previous studies compared between the infrared devices and ultrasound to guide venous cannulation, but there are some studies compared this new technique with standard method for cannulation. Caglar, Inal and et al., [18], in their randomized controlled trial examined the efficacy of vein visualization devices and the routine method for insertion of peripheral intravenous catheters (PIVCs) in preterm infants. The study was conducted on 90 preterm infants who were randomly assigned to three groups the infrared group (n = 30), the transilluminator group (n = 30) and the control group (n = 30). Time to successful cannulation was significantly lower for the infrared group (8.70 ± 2.56 seconds) than for the transilluminator group (45.27 ± 30.83 seconds) and the control group (17.30 ± 8.40 seconds) (P ≤ .001). Success of the first attempt was significantly higher in the infrared and transilluminator groups than in the control group (P ≤ .05). Dwell time of the PIVC in place was significantly higher in the infrared group than in the transilluminator and control groups (P ≤ .05). The use of an infrared device provides efficacy in time to successful cannulation, success of the first attempt, and length of the time the catheter is in place. The shorter time of successful cannulation using the infrared device in Caglar study may be explained by the difference in the cannulation site as we used the great saphenous vein and Caglar cannulated superficial peripheral veins. Demir et al., [19], in another study reached the same conclusion that infrared vein visualization technology was effective during first-attempt of PIVCs placement.
Also de Graaff et al., [13] assessed near-infrared light to aid peripheral intravenous cannulation in children in randomized clinical trial of three devices. They included 1913 children between birth and 18 years scheduled for elective surgery. Suitable veins for cannulation were more easily visible with the Vein Viewer (307/322 (95.3%)) and AccuVein (239/254 (94.1%)) devices than with VascuLuminator (229/257 (89.1%)) (p = 0.03). However, success at the first attempt was not significantly different among groups, ranging from 73.1% to 75.3% (p = 0.93. They conclude that although vein visibility is enhanced, near-infrared devices do not improve cannulation.
Kaddoum et al., [20] conducted a randomized controlled trial on 146 patients under 17 years old, comparing the AccuVein AV300 device to standard insertion technique for intravenous cannulation and recorded the number of skin punctures, cannulation attempts required, and the time between tourniquet application and successful cannulation. The first-attempt success rates were 75% using AV300 and 73% using the standard method (P = 0.85). The difference between the two treatment groups in number of skin punctures and the time to insertion was not significant. Although the AV300 was easy to use and improved visualization of the veins, they found no evidence that it was superior to the standard method of intravenous cannulation in unselected pediatric patients under anesthesia. The higher first-attempt success rates demonstrated by Kaddoum compared to the present study may be due to that the patients enrolled in his study are much older and so cannulation is much easier.
Rothbart et al., [3] couldn’t demonstrate any significant reduction in neither the time nor number of attempts until a successful venous cannulation when using the AV300 device. Their studyincluded 238 pediatric patients under the age of 17 years allocated into two groups: a control group (124 patients) and an intervention group (114 patients) in a non-random way. In the control group, peripheral IV cannulation was performed without any supporting device, while in the intervention group the cannulation was supported by using the AV300 device. The mean time until successful cannulation was 2 min in the intervention group and 1 min in the control group (p < 0.01). Median number of attempts was higher in the intervention group than in the control group. Rate of successful cannulation at first attempt was 0.45 in the intervention group and 0.73 in the control group (p < 0.01). This may be explained by the fact that the patients enrolled in the study did not have a difficult venousaccess so no added advantage was obtained by using the AV300 device.
There are many studies investigated ultrasound guidance for venous cannulation in infants, as Triffterer et al., [1] in their study, ninety infants ≤12 months undergoing elective surgery were included and divided into two age groups (0-6 and 7-12 months). After anesthesia induction with sevoflurane, an ultrasound investigation of both GSVs at the level of the medial malleoli was performed. Subsequently, venous access in one GSV was established under direct ultrasound control. Anatomical ultrasound data and success rates of venous accesses were analyzed. The success rate in infants ≤6 months was 96%, whereas in older infants, the success rate was 100%. The overall success rate in all infants was 98%. They concluded that, Ultrasound facilitates venous puncture of the GSV with direct visualization in the vast majority of infants ≤12 months. Benkhadra et al., [21] also conducted a randomized study on 40 children with difficult venous access and younger than 3 years old. They concluded that US guidance significantly increased the first-attempt success rate (85%) when compared to using traditional methods(35%) anddecreased the time needed for cannulation.On the other hand Bair et al., [22] found that the success rate of venous cannulation did not improve by using ultrasound guidance in comparison with the standard technique. This may bedue to the fact that they used ultrasound to detect the vein and then mark its position on theskin thenimmediately used this skin impression as a landmark for cannulation attempts that is to say they did not use a real time ultrasound to guide venous cannulation.
In 2013 Girgis [4], conducted a study on 80 children, younger than 6 years of age, and having difficult venous access. The patients were randomized to either US guidance (the US group, n = 40) or transillumination using the Veinlite EMS (the Veinlite group, n = 40). The first-attempt success rate was significantly higher in the US group (82.5%) compared with the Veinlite group (57.5%, P < 0.05). Both groups showed a high overall success rate (92.5% in the US group and 80% in the Veinlite group, P = 0.19). The time to achieve successful cannulation was significantly shorter in the US group (67.1 ± 19.3 s) than in the Veinlite group (94.1 ± 49.9 s, P < 0.01). The number of attempts required was not significantly different between the two groups. He concluded that,Both US guidance and transillumination facilitate peripheral intravenous cannulation in pediatric patients with difficult venous access, resulting in a high overall success rate of cannulation. US guidance is superior as it results in a higher first-attempt success rate with less time required to achieve successful cannulation compared with transillumination. The higher first time success rate when using the ultrasound in Girgis study compared to this study may be due to that Girgis used the superficial vein in older aged group patients never the less the all over success rate is comparable to each other. On the other hand the overall results obtained in this study using the AccuVein 400 is much better than the results obtained by using the transillumination device (Veinlite EMS) in spite of the age difference in both studies.
Acknowledgement & Declarations
No external funding or competing interests declared. The study was supported from anesthesia department (Alexandria University, Egypt).
Conclusion
Both AccuVein 400 and ultrasound-guided vascular access in the GSV at the level of the medial malleolus in infants ≤12 months are promising techniques that have the potential to be used routinely in pediatric anesthesia with no statistical difference in the success rate for cannulation between the two groups. But with the AccuVein 400 the time of tourniquet and cannulation was shorter than with the use of the ultrasound.
References
- Triffterer L, Marhofer P, Willschke H, Machata AM, Reichel G, Benkoe T,et al. Ultrasound-guided cannulation of the great saphenous vein at the ankle in infants. Br J Anaesth. 2012 Jul;109(1):129-30.Pubmed PMID:22696570.
- Nafiu OO, Burke C, Cowan A, Tutuo N, Maclean S, Tremper KK. Comparing peripheral venous access between obese and normal weight children. Paediatr Anaesth.2010 Feb;20(2):172-6.Pubmed PMID:19922428.
- Rothbart A, Yu P, Lobeck LM, Spies CD, Wernecke KD, Nachtigall I.Peripheral intravenous cannulation with support of infrared laser vein viewing system in a pre‑operation setting in pediatric patients. BMC Res Notes.2015 Sep 21;8:463.Pubmed PMID:26391665.
- Girgis KK. Ultrasound guidance versus transillumination for peripheral intravenous cannulation in pediatric patients with difficult venous access. Egypt J Cardiothorac Anesth. 2014 Jan 1;8(1):39.
- Costello JM, Clapper TC, Wypij D. Minimizing complications associated with percutaneous central venous catheter placement in children: recentadvances. Pediatr Crit Care Med.2013 Mar;14(3):273-83.Pubmed PMID:23392365.
- Lenhardt R, Seybold T, Kimberger O, Stoiser B, Sessler DI.Local warming and insertion of peripheral venous cannulas: single blinded prospective randomised controlled trial and single blinded randomised crossover trial. Br Med J. 2002 Aug 24;325(7361):409-10.Pubmed PMID:12193353.
- Goren A, Laufer J, Yativ N, Kuint J, Ben Ackon M, Rubinshtein M, et al. Transillumination of the palm for venipuncture in infants. Pediatr Emerg Care. 2001 Apr;17(2):130-1.Pubmed PMID:11334094.
- Chappell S, Vilke GM, Chan TC, Harrigan RA, Ufberg JW. Peripheral venous cutdown. J Emerg Med.2006 Nov;31(4):411-6.Pubmed PMID:17046484.
- Samoya SW. Real-time ultrasound-guided peripheral vascular access in pediatric patients. Anesth Analg.2010 Sep;111(3):823-5.Pubmed PMID:20733172.
- Leyvi G, Taylor D, Reith E, Wasnick JD. Utility of ultrasound-guided central venous cannulation in pediatric surgical patients: a clinical series. Paediatr Anaesth.2005 Nov;15(11):953-8.Pubmed PMID:16238556.
- Aulagnier J, Hoc C, Mathieu E, Dreyfus JF, Fischler M, Guen M. Efficacy of AccuVein to facilitate peripheral intravenousplacement in adults presenting to an emergency department: a randomized clinical trial. Acad Emerg Med. 2014 Aug;21(8):858-63.Pubmed PMID:25176152.
- Sun CY, Lee KC, Lin IH, Wu CL, Huang HP, Lin YY, et al. Near-infrared light device can improve intravenous cannulation in critically ill children. Pediatr Neonatol. 2013 Jun;54(3):194-7.Pubmed PMID:23597539.https://www.ncbi.nlm.nih.gov/pubmed/23597539
- de Graaff JC, Cuper NJ, Mungra RA, Vlaardingerbroek K, Numan SC, Kalkman CJ.Near-infrared light to aid peripheral intravenous cannulation in children: a cluster randomized clinical trial of three devices. Anaesthesia. 2013 Aug;68(8):835-45.Pubmed PMID:23763614.
- Perry AM, Caviness AC, Hsu DC (2011) Efficacy of a near-infrared lightdevice in pediatric intravenous cannulation: a randomized controlledtrial. Pediatr Emerg Care. 2011 Jan;27(1):5-10. Pubmed PMID:21178814.
- Chapman LL, Sullivan B, Pacheco AL, Draleau CP, Becker BM. VeinViewerassisted intravenous catheter placement in a pediatricemergency department. Acad Emerg Med. 2011 Sep;18(9):966-71.Pubmed PMID:21854488.
- Kim MJ, Park JM, Rhee N, Je SM, Hong SH, Lee YM, et al. Efficacy of Vein-Viewer inpediatric peripheral intravenous access: a randomized controlledtrial. Eur J Pediatr. 2012 Jul;171(7):1121-5.Pubmed PMID:22415409.
- Sriparkdee C, Sawangwong S, Curry P, Tatiyanupunwong S.A randomized controlled trial comparing the AccuVein AV400 device to standard insertion technique for peripheral intravenous cannulation by experienced nurse anesthetists in obese patients undergoing elective surgery. Thammasat Medical Journal.2016;16(4): 546- 52.
- Caglar S, Buyukyılmaz F, Bakoglu I, Inal S, Salihoglu O. Efficacy of Vein Visualization Devices forPeripheral Intravenous CatheterPlacement in Preterm Infants. A randomized clinical trial. J Perinat Neonat Nurs.2019 Jan/Mar;33(1):61-67.Pubmed PMID:30676463.
- Demir D, Inal S(2017)Does the use of a vein visualization devicefor peripheral venous catheter placement increase successrate in pediatric patients? Pediatr Emerg Care. doi:10.1097/PEC.0000000000001007.
- Kaddoum RN, Anghelescu DL, Parish ME, et al (2012) A randomized controlled trial comparing the AccuVein AV300 device to standard insertion technique for intravenous cannulation of anesthetized children. Pediatr Anesth. 22(9):884–9.
- Benkhadra M, Collignon M, Fournel I, Oeuvrard C, Rollin P, Perrin M, et al(2012) Ultrasound guidance allows faster peripheral IV cannulation in children under 3 years of age with difficult venous access: a prospective randomized study. Paediatr Anaesth 22:449–54.
- Bair AE, Rose JS, Vance CW, Andrada-Brown E, Kuppermann N (2008) Ultrasoundassisted peripheral venous access in young children: a randomized controlled trial and pilot feasibility study. West J Emerg Med 9:219–24.





