Patterns Of Intensive Care Unit Admission And Associated Factors Among Surgical Patients In Jimma University Medical Center. Jimma, South West Ethiopia
Sakalo, Birhanu Mengistu*, Yeabsira Tesfaye
Institute of Health, Faculty of Medical Sciences, Jimma University, Jimma, Ethiopia.
*Corresponding Author
Sakalo, Birhanu Mengistu,
Institute of Health, Faculty of Medical Sciences, Jimma University, Jimma, Ethiopia.
Tel: +251937146926
E-mail: birhanumengistu8@gmail.com
Received: September 30, 2021; Accepted: January 25, 2022; Published: February 04, 2022
Citation: Sakalo, Birhanu Mengistu, Yeabsira Tesfaye. Patterns Of Intensive Care Unit Admission And Associated Factors Among Surgical Patients In Jimma University Medical Center. Jimma, South West Ethiopia. Int J Anesth Res. 2021;09(03):668-672.
Copyright: Sakalo, Birhanu Mengistu© 2022. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: An intensive care unit (ICU) is a specially staffed and equipped, separated area in a hospital, dedicated to the
management of patients with life threatening illnesses and which incorporates patients that need advanced respiratory, airway
or hemodynamics support. Even though there is ICU in JUSH the quality as well as the quantity is inadequate. Therefore studying
the frequency of admissions in the ICU, reasons for admission in the ICU, the average duration of stay in the ICU and also
whether or not the admitted patient needed mechanical ventilation or not, may help understand the problems present regarding
to the ICU and help advance the service.
Objective: To review the pattern of admission and associated factors among surgical patients admitted to the ICU of JUSH,
Jimma, Ethiopia in the last one year (January 2020-January2021).
Method: One year retrospective analysis was done on patterns of ICU admission among all surgical patients of JUSH. The
study includes the cause of admission, the average duration of stay in ICU. The data was collected using questionnaire and
obtained result is displayed using tables and graph .The data collected is analyzed manually by using scientific calculator.
Result: There were 152 surgical admissions to ICU making 39.69% of total ICU admissions male to female ratio was 1.47:1.
Twenty eight patients (18.42%) were pediatric surgical patients. The total duration of ICU stay was 853. 75 days and the median
duration of ICU stay was 5.62+ 6.33 days. Seventy eight patients were mechanically ventilated out of which 48 patient were
died; only 15 patients were died out of 42 patients who were not mechanically ventilated. Majority of admissions were due to
acute abdomen 36.84% and head injury patients 26.97% . Over all sixty seven patients (44.08%) were survived while seventy
nine patients (51.98%) were died. Seventy eight patients are mechanically ventilated. The highest mortality was seen in head
injury patients 65.85% and acute abdomen 55.36%.
Conclusion: Acute abdomen and head injury were by far the commonest of admission to ICU and have highest mortality as
well. Mechanical ventilation was also associated with high mortality. Reduction of preventable causes of admission that leads
to high mortality and morbidity like severe head injury will not only lessen the burden of care but also improve the outcome
of our ICU care.
Recommendation: Based on the finding of the study collaborative effort of both government and JUSH is important to
reduce admission and mortality.
2.Introduction
3.Methodology
4.Results
5.Discussions
6.Conclusion
7.Acknowledgments
8.References
Keywords
ICU; Jimma University; Surgery.
Abbreviations
AMI: Acute Myocardial Infraction; BPH: Benign Prostate Hyperplasia; DKA: Diabetic Ketoacidosis; HW:
Health Workers; ICU: Intensive Care Unit; LOS: Length of Stay; LUTH: Lagos Teaching Hospital; MICU: Medical Intensive
Care Unit; SICU: Surgical Intensive Care Unit; TAH: Total Abdominal Hysterectomy.
Introduction
Intensive care unit (ICU) is a special unit primarily concerned
with the care of patients with critical illness and demands a broad
based knowledge to provide for all aspects of management of
these patients to achieve good outcome. [1]
In 1854, Florence Nightingale left for the Crimean war, where triage was used to separate seriously wounded soldiers from the lessseriously
wounded was observed. Until recently, it was reported
that Nightingale reduced mortality from 40% to 2% on the battle
field.
Although this was not the case, her experiences during the war
formed the foundation for her later discovery of the importance
of sanitary conditions in hospitals, a critical component of intensive
care. [2]
In 1950, anesthesiologist peter Safar established the concept of
advance support of life, keeping patients sedated & ventilated in
an intensive care environment. Safar is considered to be the first
practitioner of intensive care unit medicine. [2]
In response to polio epidemic (where many patients required
constant ventilation and services), Bjorn Agelbsen established the
first ICU in Copen Hagen in 1953. [2]
The first application of this idea in the United States was by Dr.
William Mosenthal, a surgeon at the Dartmouth-Hitchcock medical
center.
In the 1960s, the importance of cardiac arrhythmias as a source
of morbidity and mortality in myocardial infarction (heart attack)
was recognized. This used to the routine use of cardiac monitoring
in ICUs, especially after heart- attack. [2]
Over the years ICU have emerged as a distinct discipline and
ranged in scope from general, medical, surgical, neuro- surgical,
cardiothoracic, Neonatal, pediatric, coronary care, burn, and trauma
ICUs to name but few. [2]
Worldwide, ICU requires a vast use of up to date resources like,
advanced monitors, organ support equipment’s and highly skilled
staff. This however, often takes the most resilient health system
even of the developed nations. In most developing countries
where there are several financial limitations resulting from poor
funding of the health care generally and the ICU specially, there
is often a limit to the availability and specialization of this form
of care. [3]
Even though there is no published data showing about the JUSH,
ICU, generally in developing countries ICU is confounded by
inadequate staffing, training, diagnostic and interventions limitations.
Statement of the Problem
Caring for critically ill patient is a challenge in developing countries,
where health needs often out strip available resources. Necessary
equipment is scarce and often malfunctions, and trained
man power is limited.[2]
Intensive care unit in such settings is reduced to high dependency
nursing care, yet the patients are critically and need intensive care,
and so cannot to be turned away from the hospital.[10]
Intensive care unit in most of the developed nations are high
technology facilities with the most advanced medical technologies,
electronic monitoring, mechanical ventilation and other life support measures, as well as up to date drugs and highly trained
and skilled personal. In tropics however, various levels of care for
the critically ill patients have been described, and intensive care in
the developing countries have been defined as doing the best for
the critically ill with the resources available. [3, 4]
Methods and Materials
Study Area & Period
The study will be conducted in JUSH, Intensive care unit. JUSH
is found in Jimma zone, Jimma Town, located 350km southwest
of Addis Ababa. It was established in 1930. It is the only referral
hospital located in southwest Ethiopia serving over 2.8 million
people. It has a bed capacity of 800 and a total of greater than
750 staffs of both supportive and professional. Provides services
for 15,000 in patient and 160,000 outpatient attendances in a year;
coming from the catchment area of about 15 million people. It
provides surgical service for over 500 patient’s. It has nine operation
rooms and one adult ICU room which have six beds in my
study period which is from January 2020 to January 2021.
Study Design
Retrospective analysis of surgical patients admitted ICU of JUSH
over the last one year will be done.
Population
Source population: All surgical patients admitted to ICU of
JUSH
Study population: All surgical patients admitted to ICU of
JUSH in last 1 year (January 2020-January2021)
Inclusion and exclusion criteria: Inclusion criteria - surgical
patient in ICU.
Exclusion criteria - non surgical patient in ICU
Sampling technique and sample size
No sampling technique is used. All surgical patients admitted to
ICU of JUSH in the study period were included.
Study variables
Dependent variable : Pattern of ICU admission.
Independent variables
Age
Sex
Length of ICU stay
Co- morbidity
Trauma
Post-operative surgery
Data collection instrument and methods
Data collection tool was adapted after review of relevant literature. Data was collected by two trained data collectors used to
retrieve information about patient socio demographic characteristic,
causes of ICU, admission, ICU stay and patient out come
through patient record or card review.
Data quality control
The data collection instrument was pretested on 10% of surgical
patients admitted to ICU in the last year prior to the actual data
collection to check missed information so as to make possible
amendments. Selection and training of two diploma level nurses
for data collection was done. To checking for completeness
and consistency of collected data at the end of each days done
throughout data collection period.
Data processing and analysis
After checking the completeness of the data, it was tallied and
compiled on tally sheets and analyzed manually using scientific
calculator. Finally data was presented in tables and graphs as necessary
and cross tabulation with the statistical test for association.
Ethical consideration
Prior to data collection a formal letter of permission was collected
from JU student research program office and forwarded to
JUSH administrative office. Patients records was kept confidential
Limitation of the study
Some of the patients records (cards) was incomplete available or
lost. Some of the patient had been discharged without being registered
in to ICU patients register log book.
Dissemination of Results
After data analyzed conclusion and recommendation was made,
the result was result submitted to concerned body.
Results
Description of surgical patients admitted to ICU
152 (39.69%) surgical patients were admitted to ICU out of
383 patients in the last one year, among which 89 patients were
male and 63 patients were female making male to female ratio of
1.41:1. 28 (18.42%) were pediatric surgical patients and the rest
124 patients (81.58%) were adult. Out of adult patients 36.84%,
17.76%,20.4%, 6.58% were in age group 16-30, 31-45,46-60 and
>61 years old respectively (Table 1).
Length of stay
The total length of ICU stay was 853.75 day and the lowest and
highest stay was 6hrs and 24 days respectively making the range
of 23.75 days .The mean length of ICU stay was 5.62+6.33 days.
78(51.32%) stayed in ICU for <5 days and 5(3.29%) patients
stayed for >3 weeks, while 38 (25%), 24 (15.79%) and 7 (4.6%)
were stayed for 4-7, 8-14, 15-21 and >21 days in ICU (Table 2).
Cause of Admission
The leading causes of surgical admission to ICU were acute abdomen
56 (36.84), head injuries 41(26.97%), post thyroidectomy
19(12.50%), Extracraninal injuries 12 (7.89%), burn injuries
7(4.60%) and other (post elective surgeries like BPH, esophageal
cancers, colon ca. and submandibular abscess and upper air way
obstruction), 17 (11.18%) (Fig1).
Highest mortality was seen in head injury (65.83%) patients and
acute abdomen (57.14%) while post thyroidectomy, burn and extra
cranial injuries had mortality rate of 47%,37% ,28,57% and
25% respectively. The other which includes BPH, malignant cancers,
and necrotizing fasciitis which account 35% (Fig 1).
Care given to the patients
The patient admitted to JUSH ICU were provided necessary care
and monitored using frequent vital sign monitoring and system monitoring in addition to routine nursing care and medical therapies.
Out of care given, 120 patients were analyzed for mechanical
ventilation from which 78 (65%) were ventilated and 15(35.7%)
of non-ventilated patients were died.
The study showed that there is an association between ventilation
and poor outcome (Table -3).
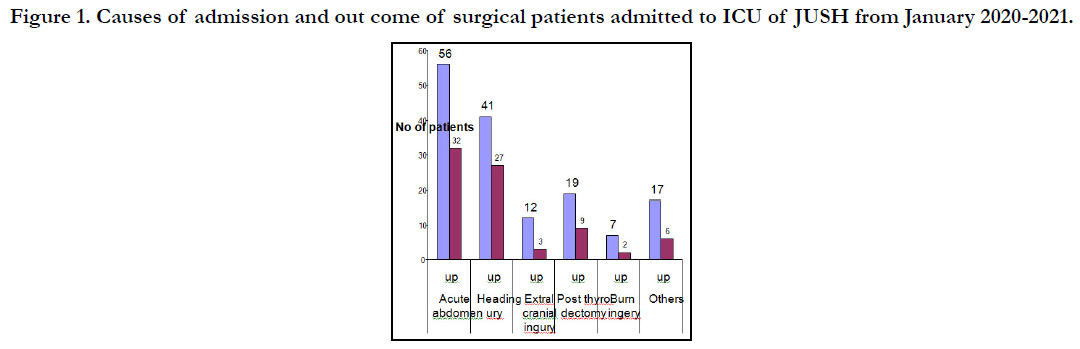



Table 1. Frequency of cases of surgical patients admitted to ICU of JUSH by age group, January 2020 - January 2021.

Table 2. Length of ICU stay of surgical patients admitted to the ICU of JUSH from January 2020-January 2021.

Table 3. Association between mechanical ventilation and outcome of surgical patients admitted to ICU of January 2020- January 2021.
Discussion
In this review 39.9% of the cases admitted to JUSH ICU the
last one year This was near to the study done in ICU of prince
Rashid Hospital of Jordan, where 29% of ICU admissions were
surgical patients. The slight difference can be In the studies made
in Nigeria and Burkina Faso it showed 66.7% and 81% of total
ICU admissions were surgical respectively. This difference can be
explained by the fact that they included gynecology and Obstetrics
patients as surgical. There was male to female ratio of 1.41:1
which was similar to that of study done in Malawi. [7, 10, 11].
18.42% were pediatric surgical patients and the rest 81.58% were
adult patients. Of the adult patients 36.84% were in the age group
16-30 years. And 20.4% were in the age group of 46-60 years,
while 17.76% were in 31-45 years and 6.58% were in the group
of 61-75 years age. In the study done at price Rashid hospital,
Jordan, pediatric surgical patients were 43% this difference can be
explained by study period.
The total duration of ICU stay was 853.75 days and the median
duration of ICU stay was 5.62+6.33 days. About 51.32% were
stayed in ICU for 3 days or less while only 3.29% were stayed for
more than 3 weeks.25% were stayed in ICU for a period of 4-7
days. 15.79% were stayed for two weeks while 4.6% were stayed
for three weeks. The lowest ICU stay was six hours. This is similar
to the study done in Jamaica where average duration of stay was
6.3+8.4 days [1].
Acute abdomen was the leading cause of admission accounting
for 36.84% followed by head injury patients who accounted for
26.97%.Extra cranial injuries which include chest injury, thoracoabdominal
injury, abdominal injury, pelvic injury and poly- trauma
accounted for 7.89%.Admission to ICU after thyroid surgery was
(12.5%). There were seven burn injury patients (4.60%). The others
were cases post-elective surgery like benign prostatic hyperplasia,
esophageal cancer, colonic cancer, and sub- mandibular
abscess and upper air way obstruction which accounted for seventeen
cases (11.18%). These results are similar to the study done
in Burkina Faso where post-operative cases accounted for 35%
and head injury accounted for 31% of admissions [10]. (Table 2).
There were over all 79 patients (51.98%) died and 67 patients
(44.08%) survived, while the outcome of 6 patients was not indicated
(Table). This figure is high when compared to the reported
ICU mortality rate which varies form 15-35% depending on the
case mix, age LOS and organizational aspect of the unit. This
difference is may be due to socio-demographic and economic
factors the patients admitted at to hospital last stage of disease
after staying at home for a long time and going to the near health
centers.
In this study it was found that acute abdomen was the leading
cause of death followed by head injury. The mortality rate was
highest for head injury patients 67.5% followed by acute abdomen
57.4%. This is similar to the study done in Malawi where
the mortality among the head injury was 70% and the study done
in Burkina Faso where the mortality rate was 70.5% for traumas
and 48.5% for post-operative cases (10.11). These two countries
are among the poorest countries in the world like Ethiopia. Post
thyroidectomy, burn and extra cranial injuries had mortality rate
of 47.08%, 28.57% and 25% respectively. This showed there was
high mortality among head injury patients.
Mechanical ventilation is a supportive measure for all patients in
any form of respiratory failure until the primary cause is reversed.
The cause for respiration failure ranges from a failure of central
nervous control to the peripheral mechanical failure and / or problem in the lungs primary affecting gas exchange.[16]. Although
studies have shown higher mortality in ventilated patients,
ventilator support is essential in cases like acute severe asthma,
multiple trauma and Abdominal sepsis [17]. Seventy eight patients
were mechanically ventilated out of which 48 patients were
died. Only 15 patients were died out of 42 patients who were
not mechanically ventilated. Thirty two patients were not analyzed
because their cards were not found. And this study showed that
there was an association between mechanical ventilation and outcome
of patient similar to studies done in Nigeria and Burkina
Faso. [9, 10].
Accurate record keeping is part of the high standard of care required
of medical personnel and admission and discharge summaries
should be documented for every patient. Accurate records
are helps for the purpose of audit, teaching and research and for
medico- legal issues [14]. In our ICU documents were entered
on log book by nurses, some being illegible to be read. Some patient’s
cards were also not found or lost due to various reasons.
Computerization of the records would have been considerable in
maintaining accuracy and retrieving relevant data.
Conclusion
According to this study 152 surgical patient were admitted to
JUSH ICU in the last one year, making female to male ratio of
1.4:1. The mean length of stay in ICU was 5.62+6.33. Among
determined causes of admission acute abdomen (36.84%) constitutes
the most common diseases entity responsible for admission
in ICU followed by trauma related cases which were severe head
injuries (26.97%) and extra cranial injuries 7.89%. Burning injuries
were the least caused of admissions.
Out of admission 51.98% were died and 44.05% were survived.
The highest mortality was seen in head injuries (65.85%) followed
by acute abdomen (57.14%). The least was extra cranial injuries
25%. Higher mortality in ventilated patient than non-ventilated
patients was observed.
Finally most of causes of admission and out comes were preventable
which then decrease hospitalization and significant amount
of budget of health care.
Recommendation
Based on the finding of the study, the following recommendations
are forwarded.
Emphasis should be given by the government in reducing road
traffic accident to prevent traumas which will directly reduce causes
of admission and hospital and individual budget.
JUSH should give early intervention of case of acute abdomen
as quickly as necessary and should have good interconnection
with satellite hospital and Health centers in referral cases and
training.
JUSH record office should keep all patient records, if possible
its better to computerize data of patients.
Lastly we recommend further study to investigate why mechanical
ventilation had association with mortalities.
Acknowledgment
We would like to acknowledge Jimma university institute to health
for the support to undertake this research. Hereby we declare that
there is no conflict of interest regarding this research paper.
References
- Abubakar AS, Ojo EO, El-Nafaty AU, Edomwonyi NP. An audit of oneyear intensive care practice in a developing country. The internet journal of Anesthesiology. 2008;18(2):1-5.
- Free encyclopedia
- Raff M, James MF. An audit of anaesthetic record keeping. Southern African Journal of Anaesthesia and Analgesia. 2003 Jul 1;9(3):7-9.
- Wattors D. Caring for the critically ill. African Health 1993:16(1):22-24.
- Harahsheh BS, Hiyasat B, Harahsheh A. Audit of paediatric surgical intensive care unit admissions in north Jordan. EMHJ-Eastern Mediterranean Health Journal, 8 (4-5), 671-673, 2002. 2002.
- Merah NA, Okeke CI, Olatosi JO. An audit of surgical admissions to the intensive care unit of the Lagos University Teaching Hospital (1997-2002). The Nigerian postgraduate medical journal. 2006 Jun 1;13(2):153-6.
- Mitchel VT, Scarlet MD, Amata AO.Trauma admissions to the ICU of vaiveggil Hospital of the west Indies, Kingston, Jamaica. Trauma care 2001; 11:86-89.
- Size, M., Borgstein, ES and Haisma HJ. One-year audit of admissions to the intensive care unit of the queen Elizabeth Central Hospital, Blantyre. Malawi Medical Journal. 2005 Jun 1;17(1):12-4.
- Ouédraogo N, Niakara A, Simpore A, Barro S, Ouédraogo H, Sanou J. Intensive care in Africa: a report of the first two years of activity of the intensive care unit of Ouagadougou national hospital (Burkina Faso). Sante (Montrouge, France). 2002 Oct 1;12(4):375-82.
- N. Mato, AC On wuchekena: Pattern of admissions to the university of port Har caurt teaching Hospital intensive care unit.
- Lim BL, Chan YW. Audit of 2431 admissions to the Surgical Intensive Care Unit, Singapore General Hospital. Annals of the Academy of Medicine, Singapore. 1998 May 1;27(3):314-7.
- Vasanthathilaka VNJK, Goonasekera CDA: An audit of admissions to an ICU in a regional center in Sri-lanka.Ceylon Medical Journal 1997; 42; 145-148.
- . Bhat SA, Shinde VS, Chaudhari LS. Audit of intensive care unit admissions from the operating room. Indian Journal of Anaesthesia. 2006 May 1;50(3):193-200.
- Zenebe M, Mengistu A, Kebede O, Getachew T. Pattern of Admission to the MICU of Addis Ababa University Teaching Hospital. EMJ. Jan 2006:4(1).
- Kinfu Betemarium, Gebreyesus Hagos. Pattern of Admission to SICU of TAH for mechanical ventilation. EJHD, 2001; 15(3):193-195.
- Bone RC, Mc Ewe NE, Eubanks DH, Gluck EH. Analysis of indication for intensive care at admission of physicians. Chest 1993:104:1806-11.
- Desikan SR, Bray B, Kurian J, Ali S, Chappel W. Outcome after ICU admission in patients over ninety years old. Anesthesiology. 2007;107:A331.





