Treatment of Lentigomaligna in Dark Skin with Topical Imiquimod Results in Dark Hyperpigmentation
Elberling J*,Wulf H C
Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Copenhagen, 2400, Denmark.
*Corresponding Author
Jesper Elberling
Department of Dermatology, Bispebjerg Hospital,
Bispebjerg Bakke 23,2400 København NV, Denmark.
Tel: +45 40 46 75 20
E-mail: Jelberling@dadlnet.dk
Article Type: Case Report
Received: May 26, 2014; Accepted: June 23, 2014; Published: June 25, 2014
Citation: Elberling J, Wulf H C (2014) Treatment of Lentigomaligna in Dark Skin with Topical Imiquimod Results in Dark Hyperpigmentation. Int J Clin Dermatol Res. 2(3), 19-20. doi: dx.doi.org/10.19070/2332-2977-140005
Copyright: Jesper Elberling© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
LentigoMaligna (LM) is an in situ lesion with a low risk of progression to LM Melanoma (LMM). Treatment of LM is mostly advocated because an invasive component of LMM might be lethal. Recently topical Imiquimod 5% cream was introduced as a new treatment possibility.
We describe here a patient, with skin type IV, with a hyperpigmented LM eruption at his forehead. The lesion was treated 4 weeks with topical Imiquimod 5%, 5 times a week for 8 weeks. Four weeks after cessation of treatment the macular lesion appeared enlarged and darker indicating lack of response. Punch biopsies revealed post-inflammatory hyperpigmentation (PIH) and ruled out LM and LMM. During 6 moths observation the skin normalized.
The present case is a reminder that dark skin comprises an increased risk of PIH that when induced by Imiquimod treatment of LM can be mistaken as lack of therapeutic efficacy or progression to LMM.
2.Case Report
3.Discussion
4.References
Keywords
Imiquimod; Dark Skin; LentigoMaligna; Post-Inflammatory Hyperpigmentation.
Case Report
A previously healthy 63-year-old man with Fitzpatrick skin type IV was referred to our clinic with a sharply demarcated, macular, brownish-colored lesion located on the left temporal area of the forehead. The lesion had developed over a 3 months period. The patient had no personal history of malignant melanoma but reported a grandfather who had died from skin cancer of unknown type. A 3-mm punch biopsy revealed LentigoMaligna (LM). Further physical examination was normal. Topical Aldara® therapy (Imiquimod 5% cream) was prescribed once daily, five times a week for eight weeks. The lesion showed an inflammatory response to topical Imiquimod treatment (Fig. 1A). Four weeks after cessation of the treatment the lesion appeared as an irregular dark brownish macule with a central regression zone. The lesion was enlarged with hyperpigmentation corresponding to 0.5-1 cm treatment margins around the original lesion (Fig. 1B). Still, no lymph node enlargements were present in the head or neck region. In order to rule out malignant transformation three 2-mm punch biopsies were obtained, (two from the dark margins of the lesion and one from the central area with regression). The histological examination of the biopsies revealed superficial perivascular lymphocytic inflammation with a few malanophages, increased pigmentation in the basal layer and a normal number of melanocytes without atypical transformation- or proliferation pattern. The presence of post-inflammatory hyperpigmentation (PIH) was in accordance with the quick development of a hyperpigmented macular lesion corresponding to the area treated with Imiquimod. No further treatment was introduced and the patient was followed for 6 months with complete elimination of the PIH (Fig. 1C). Probably due to a general chronic sun-damage of the surrounding skin the treated area appeared slightly hypopigmented.
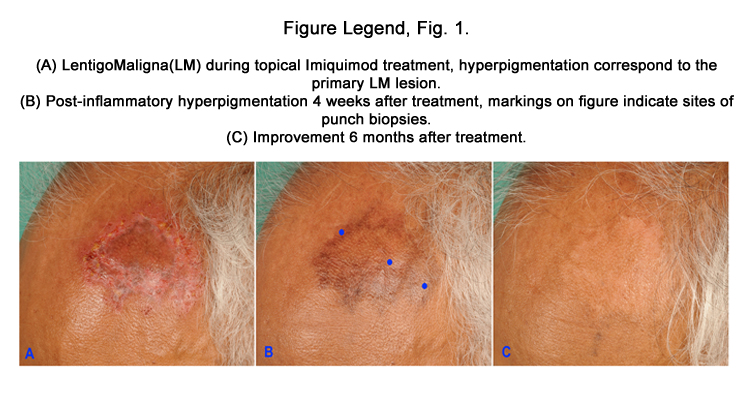
Figure Legend, Fig. 1.
(A) LentigoMaligna(LM) during topical Imiquimod treatment, hyperpigmentation correspond to the primary LM lesion.
(B) Post-inflammatory hyperpigmentation 4 weeks after treatment, markings on figure indicate sites of punch biopsies.
(C) Improvement 6 months after treatment.
Discussion
Lentigomaligna (LM) is the in situ phase of lentigomaligna melanoma (LMM). The risk of LM developing into LMM is unknown, but estimated to be low [1]. Mostly LM occurs on the face in patients with sun-damaged skin. With surgical excision of LM, the risk of leaving disfiguring scars is considerable. Recently, the off label treatment of LM with topical Imiquimod 5% cream was introduced as a cosmetically more acceptable treatment possibility [2]. In prospective studies of patients with LM who were treated with topical Imiquimod, sustained histological clearance were only verified in about 50%, based on post-treatment biopsies in one study [3] and excisions of the entire treated LM-lesions in another [4]. It is likely that the therapeutic efficacy of Imiquimod on LM, however, might be under-estimated in such studies because histologic differentiation between LM and the features of sun-damaged skin is difficult [5-6]. Nevertheless, long-term follow-up on patients with LM treated with Imiquimod, as monotherapy, seems to be recommendable until long-term follow-up data is available. Imiquimod induces inflammation via the toll-like receptors [7]. In our patient with skin type IV, Imiquimod induced severe but transient post-inflammatory hyperpigmentation. Postinflammatory hyperpigmentation consist of macular hyperpigmentation with epidermal and dermal hypermelanosis at the site of inflammation [8].
References
- Weinstock MA, Sober AJ(1987) The risk of progression of lentigomaligna to lentigomaligna melanoma. Br J Dermatol116:303-310.
- Naylor MF, Crowson N, Kuwahara R, Teague K, Garcia C (2003) Treatment of lentigomaligna with topical imiquimod. Br J Dermatol149:66–9.
- Van Meurs T, Van Doorn R, Kirtschig G.(2010) Treatment of lentigomaligna with imiquimod cream: a long-term follow-up study of 10 patients.Dermatol Surgery, 36:853-8.
- Ly L, Kelly JW, O’Keefe R,Sutton T, Dowling JP et al. (2011) Efficacy of imiquimod cream, 5%, for lentigomaligna after complete excision: a study of 43 patients. Arch Dermatol.147:1191-1195.
- Bowen AR, Thacker BN, Goldgar DE, Bowen GM. (2011) Immunohistochemical staining with Melan-A of uninvolved sun-damaged skin shows features characteristic of lentigomaligna. Dermatol Surg. 37:657-663.
- Florell SR, Boucher KM, Leachman SA,Azmi F, Harris RM (2003) Histopathologic recognition of involved margins of lentigomaligna excised by staged excision: an interobserver comparison study. Arch Dermatol. 139:595-604.
- Hemmi H, Kaisho T, Takeuchi O,Sato S, Sanjo H et al. (2002) Small antiviral compounds activate immune cells via the TLR7 MyD88-dependent signaling pathway. Nat Immunol.3:196-200.
- Kundu RV. (2008) Special consideration for topical therapy in ethnic skin: 2142-46. In: Wolff K, ed.Fitzpatrick’s Dermatology in General Medicine,(7thedn), McGraw-Hill Companies, USA.





