Segmental Phenolization for the Treatment of Ingrown Toenails: Technique Report, Follow Up of 150 Patients, and Review of The Literature
Bouzidi H*, Gallouj S, Chakiri R, Mernissi FZ
Dermatology Department of Hassan II University hospital in Fès. Morocco.
*Corresponding Author
Hanae Bouzidi,
Dermatology Department of Hassan II University hospital in Fès,
Morocco.
E-mail: bouzidi.hanae@gmail.com
Article Type: Case Study
Received: March 22, 2015; Accepted: March 27, 2015; Published: March 30, 2015
Citation: Bouzidi H, Gallouj S, Chakiri R, Mernissi FZ (2015) Segmental Phenolization for the Treatment of Ingrown Toenails: Technique Report, Follow Up of 150 Patients, and Review of the Literature. Int J Clin Dermatol Res. 3(2), 50-54. doi: dx.doi.org/10.19070/2332-2977-1500014
Copyright: Bouzidi H© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Ingrown toenail is a common problem causing significant morbidity. Various procedures used for treating this painful condition were discussed in the literature.
Objetctive: Through a prospective study we aimed to evaluate in a long-term follow-up the efficacy of partial nail plate avulsion combined with phenolic chemical matricectomy for the treatment of Ingrown toenails.
Methods: We recruited outpatient from January 2012 to January 2014; all treated by phenol matricectomy and assured a regular follow up.
Results: Consecutive 140 patients with a total of 158 Ingrown toenails were enrolled. There was no significant morbidity and the procedure was tolerated well by all patients. The short-term results were excellent. No severe complications occurred during the 6-month follow-up period. The overall recurrence was 2, 8 %.
Conclusion: Phenol cauterization compared with other surgical ablation techniques may be the treatment of choice of Ingrown toenails. It’s an effective technique for the treatment of Ingrown toenails accompanied by less morbidity and lower recurrence rates.
2.Introduction
3.Methods
4.Procedure
5.Results
6.Discussion
7.References
Keywords
Ingrown Toenails; Phenol; Matricectomy; Nail.
Introduction
Onychocryptosis, also known as an “ingrown toenails” (ING) is a common and frequent foot problem. It typically appears as inflammation of the tissue along the side of toenails. The lateral side of the great toe is the most often affected part. It is mostly seen in adolescents and young adults with active lives and the condition causes pain, discomfort, and functional limitation [1]. Depending on the stage of the disease, treatment options range from conservative measures to invasive ones. Chemical matricectomy with phenol for ING is one of the most effective surgical procedures performed on the foot. The procedure was first described in 1945 by Otto Boll [2]. It is worth mentioning that this method has so far shown very satisfactory therapeutic results. Our aim is to evaluate the effectiveness of the matrix phenolization of the hallux in the management of ING, through a prospective study; follow-up evaluations were performed by the same surgeon.
Methods
We present a monocentric prospective study conducted in the dermatology department of Hassan II University hospital in Fès over a period of two years, from January 2012 to January 2014. During this period, we treated outpatients suffering from ING and describe subsequent follow up by the same surgeon. We included all patients with the classic form of ING (lateral ING) referred to our department. Patients under 15 years old, those who presented with other clinical forms of ING, and those who had a contraindication to anaesthesia were excluded.
The data collected on a standardized sheet for each patient included: age, gender, length of evolution, history of ING, and previous treatment modalities. The risk factors, such as hyperhidrosis, abnormal nail shelf, obesity, poor or tight-fitting shoes, and abnormally sized nails were also described. Our physical examination at the time of the surgery highlighted the position of the ING and the presence of any infection. We have used the “Heifetz” classification process to evaluate the severity of the disease [3].
Grade 1: Pain, reddening and slight swelling of the nail fold.
Grade 2: As above, accompanied by infection and suppuration.
Grade 3: As above with the formation of granulation tissue.
Procedure
The great toe was disinfected with 70% alcohol. After anesthesia by a digital nerve block with 2% lidocaine (without adrenaline), the patients underwent surgery using the “Ross” procedure [4]. Absolute hemostasis was obtained with a plastic tourniquet. This procedure consists in removing three or four millimeters of the nail on the affected side without damaging the nail bed. Any present granulation tissue was curetted. Partial nail plate avulsion was performed and a small cotton bud soaked in 88% phenol was applied to the germinal matrix for two minutes in four applications of 30 seconds each (total time 2 minutes). The tourniquet was removed and the wound was dressed using a tulle gras dressing (Figure 1).
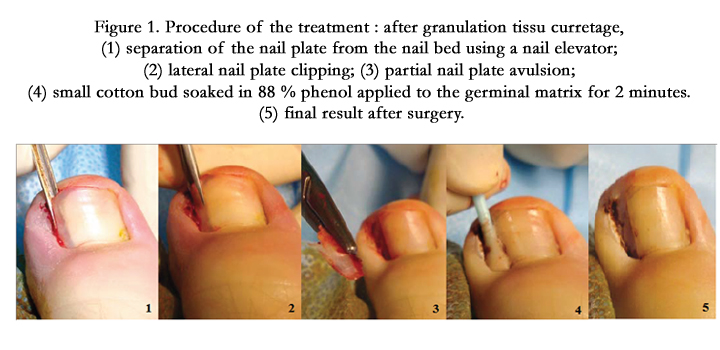
Figure 1. Procedure of the treatment : after granulation tissu curretage, (1) separation of the nail plate from the nail bed using a nail elevator; (2) lateral nail plate clipping; (3) partial nail plate avulsion; (4) small cotton bud soaked in 88 % phenol applied to the germinal matrix for 2 minutes. (5) final result after surgery.
Paracetamol (acetaminophen) was given for pain control and antistaphylococcal antibiotics if necessary and patients were instructed to keep the foot elevated during the first 24 hours. Treatment of lateral nail fold hypertrophy was performed as described by Persichetti [5].
Each of these patients were examined at 48 hours, 15 days, 1, 3, and 6 months following the surgery. The physician assessed the necessity of analgesics, the healing period, any post-operative complications (in particular those specific to the phenol cauterisation), and recurrence. Adverse side effects generally related to phenol include narrow nail, spicule, onycholysis, perionychium burn, and osteitis.
Informed consent was obtained from all patients before study. At the beginning of the study, 166 patients were enrolled after exclusion of 12 patients (see exclusion criteria). Among the 166 patients initially included, 26 failed to follow up. We finally analyzed the 140 patients who completed the full follow up described.
Results
During the study period, 140 patients (males 86/females 54) with a total of affected 158 Ingrown toenails were analyzed (18 patients presented with 2 affected toenails). The characteristics of our patients are summarized in Table 1.
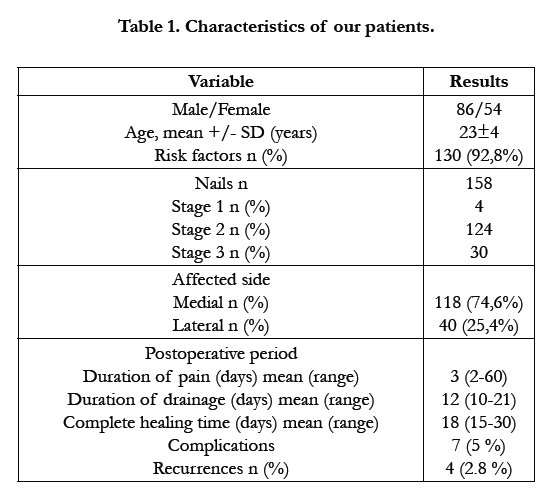

Table 1. Characteristics of our patients.
The average age of the patients was 23±4 (range 15-46) years. Only a small number of patients had presenting comorbid conditions (2.9% diabetes). The median length of time that the patients had experienced problems with the ING before presentation was 6 weeks (range 2-74); 12.3% of patients had experienced problems for more than a year. A number of a risk factors were associated (130 patients) including poor or tight-fitting shoes (90 cases), improper nail trimming (74 cases), focal hyperhidrosis (20 cases), abnormal nails such as racquet thumb (4 cases), plicatured nail (2 cases), and trauma (10 cases). A history of ING was reported in 69 patients (49.2 %). Previous treatment regimens before presentation were simple avulsion (85 %) and avulsion plus surgical matricectomy (15%).
All procedures were performed on the great toes. The medial side of the toenail was affected almost 2.7 times more frequently than the lateral side (medial: 118, lateral: 40). The two sides were affected in 17 patients, among them 6 presented with both great toes affected. Fifteen percent of patients were being treated with oral antibiotics at the time of presentation.
The patients were able to wear their shoes without problems after a median of 4 days (range, 2-40 days) and able to return to their daily work without problems after a median of 3.5 days. Analgesics were used in 115 patients (82,14 %) (means duration: 3 days, range 1-15). The patients could resume normal physical activities after 12.6 (range: 8-25) days on average. Concerning postoperative complications, proximal onycholysis was seen in 2 patients, complicated with onychomadesis and a loss of the nail in 1 case. A perionychium burn was noted in 1 patient. Postoperative infection was seen in 3 patient. No narrow nail, spicule, or osteitis were observed during the follow up period.
During the follow up period (mean 6 months, range: 4-24 months) there were four recurrent ingrowing nails (2.8%). All of them occurred between 3 and 6 months after phenolization. Three patients underwent the same procedure, which was successful, but the other declined it. Cosmetic results were remarkably good (Figure 2,3,4).


Figure 2. Phenol chemical matricectomy: (1) before surgery, (2) 3 months after surgery.


Figure 3. (1) Stage 3 ingrowing toenail, (2) 6 months after treatment with matricectomy and phenolization.


Figure 4 . (1) Preoperative, (2) 6 months after the operation.
Discussion
Partial nail plate avulsion combined with phenolization of the matrix is, in our opinion, the best and least traumatic surgical method for the treatment of ingrown toenails. Phenolization of nail matrix has been considered the most effective technique for definitive treatment of ING, with previous studies showing lower recurrence rates than other surgical matricectomy [6]. Herein we describe the results we obtained, using this technique over a2-year period in a prospective cohort. Ingrown toenail is a frequent and disabling condition, especially among adolescents and young adults, affecting walking and leading to inability to work. In the present study, 158 sites were treated in the 140 patients (86 male and 54 female) who had a mean age of 23 (range 15-46). A number of risk factors are associated with the development of ING, including wearing tight shoes, hyperhidrosis, cutting nails too short, or not cutting the nails straight. These should be investigated and corrected as far as it is possible [7]. We found a predisposing factor in 64, 2% of our patients, with a preponderance of poor or tight-fitting shoes.
A variety of treatment options have been described in ING but the treatments are often a source of significant morbidity with variable rates of recurrence (0 to 90%). The decision to choose one mode of therapy over the others should be guided by the severity of the inflammation, the chronicity of the problem, and the experience of the physician. Stage I of ING can be treated conservatively; surgery is indicated for patients with a persistent condition, Stages II and III [8]. In our cohort, most patients presented with a persistent condition and 49, 2% had a past history of ING. This could be explained by the fact that our department is a tertiary center for health care. Previous results have shown that phenolization may be at least as effective as surgical ablation and has a significant advantage.
A Cochrane review of surgical treatments for IGN concluded that simple nail avulsion combined with the use of the phenol, compared to surgical excisional technique without the use of phenol, is more effective at preventing symptomatic recurrence [6]. The target of the therapy is the chemical destruction of the lateral horns of the matrix and the prevention of future lateral nail plate growth into the lateral nail fold. The technique used in our study, segmental matricectomy with phenol, has been first described by Ross in 1945 [4]. The safety of phenol has long been questioned but many studies have shown safety in the use of this product for both the operator and medical staff. A Spanish study has shown that the phenol concentration measured in the assistant's respiration zone was well below the environmental limit of daily exposure, with an index of only 10% exposure [7].
Concerning the procedure, Tatlican has recently determined optimal times and concentrations necessary to destroy the germinal matrix without causing further soft-tissue damage [8]. Phenol applications of different durations in 3 groups were compared for 1, 2, and 3-minute applications of phenol cauterization. The application of 89% phenol solution for as little as 1 minute was enough time to cause full-thickness necrosis of the epithelium and has a better safety profile than prolonged applications in the treatment of ING [8]. The duration of phenol application in our study did not exceed 2 minutes. A lateral fold plasty procedure alone or combined with segmental matricectomy is also used in treatment of ING. In a recent study, this method has showed satisfactory results [8]. Many surgical procedures described in the literature give good results but are often associated with considerable morbidity, including postoperative pain and an undesirably high recurrence rate [6]. Our study with a long follow-up shows that phenol cauterization has various advantages and it does not involve incision or resection of soft tissue. In our experience, the patient can resume work after a median of 3.5 days after treatment. Finally, we think that the low recurrence rate (2.8 %) found in our study is owing to the fact that only one surgeon is involved in performing this procedure. In our study, the same expert dermatologic surgeon performed 158 procedures using exactly the same technique. The review of the major studies using phenol, have shown a recurrence rate ranging from 0.57% to 4.3%, see Table 2 [9-15].
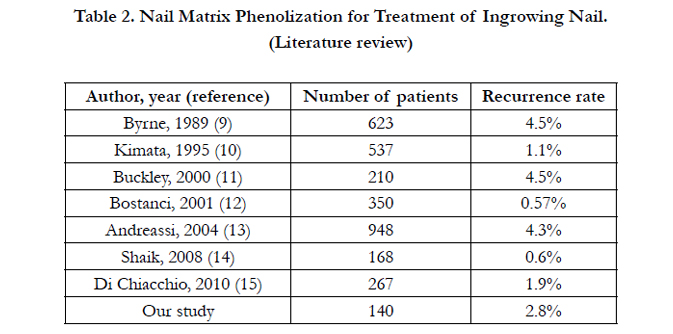
Table 2. Nail Matrix Phenolization for Treatment of Ingrowing Nail.
(Literature review)
Phenol cauterization for chemical matrixectomy has emerged as the treatment of choice for this condition. This method has presented several advantages. First, it is painless because phenol destroys nerve endings, which allows the patient to resume normal physical activities after 15 days on average (12.6 in our study [range: 8-25]) with work resumption within a short period after treatment (3.5 days in our study). Second, the procedure is a noninvasive method with no incision or stitches.
Finally many studies have documented a low recurrence rate (2.8 % in our study). Surgical procedures are often complicated with infection and it has therefore been recommended to postpone operation and put the patient on antibiotics. Because phenol is antiseptic, this is not necessary with phenol matricectomy. Reyzelman’s study showed that the use of oral antibiotics as an adjunctive therapy in treating ING does not play a role in decreasing the healing time or post procedure morbidity [16].
Bos et al investigated different surgical techniques for treating Ingrown toenails and conclude that partial nail avulsion with phenolization gave better results than partial avulsion with matrix excision [17]. Local antibiotics did not reduce signs of infection or recurrence. Use of phenol did not produce more signs of infection than matrix excision [18]. There are currently many surgical options for treating ING. However they tend to have high rates of recurrence (range 4.2-73 %), poor cosmetic results,and low rates of patient satisfaction, see Table 3 [19-27]. Other types of chemical matricectomy have been described, usually with trichloacetic acid and sodium hydroxide, with variable recurrences rates [28, 29]. Because it is relatively new in its use, there is still a lack of evidence to fully support the use of these techniques in the first line treatment of ING.
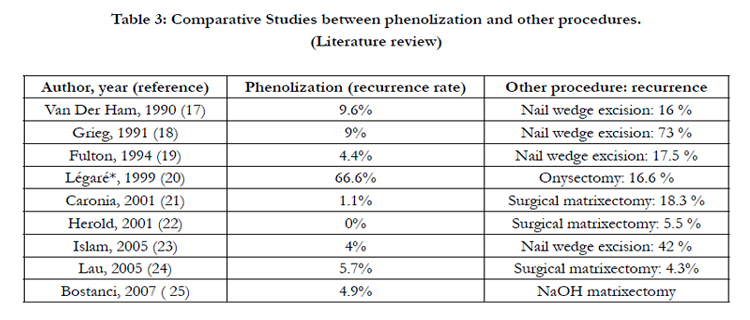
Table 3: Comparative Studies between phenolization and other procedures.
(Literature review)
Given the recurrence rate found in our patients (2.8 %) and the literature data, we could conclude that segmental phenolization is a simple and consistently effective form of treatment for ingrown toenails. Moreover, it is a quick and simple procedure with minimal discomfort, low cost, low morbidity, and high success rate, even in the long term. It can easily be done as an outpatient. It should be the treatment of choice in the case of ingrown toenails not responding to conservative treatment. Phenol is now the treatment of choice in our clinic.
References
- Haneke E (2002) Ingrown and pincer nails: evaluation and treatment. Dermatologic Therapy 15: 148-158.
- Boll O(1945) Surgical correction of ingrowing nails. J Nat Asso Chiropodists 35: 8-9.
- Heifetz CJ (1937) Ingrown Toenail. American Journal of Surgery 38: 298- 315.
- Ross WR (1969) Treatment of the ingrowing toenail. Surg Clinic North Am 49: 1499-1504.
- Persichetti P, Simone P, Li Vecchi G, Di Lella F, Cagli B, et al. (2004) Wedge excision of the nail fold in the treatment of ingrown toenail. Ann Plast Surg 52: 617-20.
- Rounding C, Bloomfield S (2003) Surgical treatments for ingrowing to enails. Cochrane Database of Systematic Reviews 1: CD001541.
- Losa Iglesias ME, Veiga de Cabo J, Tejedor Traspaderne J, Aguilar Franco J, Bernaola Alonso M, et al. (2008) Safety of phenol vapor inhalation during performance of chemical matrixectomy to treat ingrown toenails. Dermatol Surg 34: 1515-9.
- Tatlican S, Yamangöktürk B, Eren C, Eskioğlu F, Adiyaman S (2009) Comparison of phenol applications of different durations for the cauterization of the germinal matrix: an efficacy and safety study. Acta Orthop Traumatol Turc 43: 298-302.
- Aksoy B, Aksoy HM, Civas E, Oc B, Atakan N (2009) Lateral foldplasty with or without partial matricectomy for the management of ingrown toenails. Dermatol Surg 35: 462-8.
- Byrne DS, Caldwell D (1989) Phenol cauterization for ingrowing toenails: a review of five years’ experience. Br J Surg 76: 598-9.
- Kimata Y, Uetake M, Tsukada S, Harii K (1995) Follow-up study of patients treated for ingrown nails with the nail matrix phenolization method. Plast Reconstr Surg 95: 719-24.
- Buckley D (2000) Segmental phenolic ablation for ingrown toenails in general practice. Ir Med J 93: 242-4.
- Bostanci S, Ekmekçi P, Gürgey E (2001) Chemical matricectomy with phenol for the treatment of ingrowing toenail: a review of the literature and follow-up of 172 treated patients. Acta Derm Venereol 8: 181-3.
- Andreassi A, Grimaldi L, D'Aniello C, Pianigiani E, Bilenchi R (2004) Segmental phenolization for the treatment of ingrowing toenails: a review of 6 years experience. J Dermatolog Treat 15:179-81.
- Shaikh FM, Jafri M, Giri SK, Keane R (2008) Efficacy of wedge resection with phenolization in the treatment of ingrowing toenails. J Am Podiatr Med Assoc 98: 118-22.
- Di Chiacchio N, Belda W Jr, Di Chiacchio NG, Kezam Gabriel FV, de Farias DC (2010) Nail matrix phenolization for treatment of ingrowing nail: technique report and recurrence rate of 267 surgeries. Dermatol Surg 36: 534-7.
- Reyzelman AM, Trombello KA, Vayser DJ, Armstrong DG, Harkless LB (2000) Are antibiotics necessary in the treatment of locally infected ingrown toenails? Arch Fam Med 9: 930-2.
- Bos AM, van Tilburg MW, van Sorge AA, Klinkenbijl JH (2007) Randomized clinical trial of surgical technique and local antibiotics for ingrowing toenail. Br J Surg 94: 292-6.
- Van Der Ham AC, Hackeng CA, Yo TI (1990) The treatment of ingrowing toenails. A randomised comparison of wedge excision and phenol cauterisation. J Bone Joint Surg Br 72: 507-9.
- Grieg JD, Anderson JH, Ireland AJ, Anderson JR (1991) The surgical treatment of ingrowing toenails. J Bone Joint Surg Br 73: 131-3.
- Fulton GJ, O'Donohoe MK, Reynolds JV, Keane FB, Tanner WA (1994) Wedge resection alone or combined with segmental phenolization for the treatment of ingrowing toenail. Br J Surg 81: 1074-5.
- Légaré F, Dubé S, Naud A, Laperrière L, Turcot L (1999) Recurrence and satisfaction levels following onysectomy with or without phenolization. Can Fam Physician 45: 926-31.
- Caronia V, Battistioli M, Gualandi O, Marchese M, Bonotto G (2001) Treatment of the ingrown toenail by phenol cauterization. Minerva Chir 56: 199-203.
- Herold N, Houshian S, Riegels-Nielsen P (2001) A prospective comparison of wedge matrix resection with nail matrix phenolization for the treatment of ingrown toenail. Foot Ankle Surg 40: 390-5.
- Islam S, Lin EM, Drongowski R, Teitelbaum DH, Coran AG, et al. (2005) The effect of phenol on ingrown toenail excision in children. J Pediatr Surg 40: 290-2.
- Lau YS, Yeung JMC (2005) Surgical treatment of ingrowing toenails performed by senior house officers: are they good enough? Scott Med J 50: 22-3.
- Bostanci S, Kocyigit P, Gürgey E (2007) Comparison of phenol and sodium hydroxide chemical matricectomies for the treatment of ingrowing toenails. Dermatol Surg 33: 680-5.
- Kim SH, Ko HC, Oh CK, Kwon KS, Kim MB (2009) Trichloroacetic acid matricectomy in the treatment of ingrowing toenails. Dermatol Surg 35: 973-9.
- Kocyigit P, Bostanci S, Ozdemir E, Gürgey E (2005) Sodium hydroxide chemical matricectomy for the treatment of ingrown toenails: comparison of three different application periods. Dermatol Surg 31: 744-7.





