Congenital Multiple Glomangiomas of the Breast Arranged in a Segmental Pattern
Morais P1,2*, Peralta L3, Bettencourt H4, Mota A1,2
1 Department of Dermatology and Venereology, São João Hospital Center, Porto, Portugal.
2 Faculty of Medicine, University of Porto, Porto, Portugal.
3 Department of Pediatrics, Infante D. Pedro Hospital, Aveiro, Portugal.
4 Department of Pathology, São João Hospital Center, Porto, Portugal.
*Corresponding Author
Paulo Morais MD,
Department of Dermatology and Venereology, São João Hospital Center,
Alameda Professor Hernâni Monteiro,
4200-319 Porto, Portugal.
Tel: +351 225 512 117
E-mail: paulomoraiscardoso@gmail.com
Received: November 18, 2015; Accepted: November 26, 2015; Published: December 02, 2015
Citation: Morais P, Peralta L, Bettencourt H, Mota A (2015) Congenital Multiple Glomangiomas of the Breast Arranged in a Segmental Pattern. Int J Clin Dermatol Res. 3(6), 76-77. doi: dx.doi.org/10.19070/2332-2977-1500020
Copyright: Morais P© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A 15-year-old female patient presented with multiple soft, well-defined dark-blue and purple-red papules and nodules, arranged in a segmental or band-like pattern, in the right breast and ipsilateral axilla. The lesions were present since birth, had enlarged with body growth, and were slightly tender to palpation. Histopathologic examination led to the diagnosis of glomangioma. We classify our patient as having a Type 1 segmental manifestation of glomuvenous malformations with histological features of glomangiomas.
2.Case Report
3.Discussion
4.References
Keywords
Glomangioma; Glomus Tumor; Glomuvenous Malformations; Breast; Mosaicism.
Case Report
An otherwise healthy 15-year-old female patient presented with multiple bluish skin papules and nodules located at right breast that had been present since birth. The lesions were slightly tender to palpation and had enlarged with body growth, especially after menarche. Her father presented several lesions with a similar appearance on the upper limbs and trunk. On physical examination, multiple soft, well-defined dark-blue and purple-red papules and nodules were observed, arranged in a segmental or band-like pattern, in the girl’s right breast and ipsilateral axilla (Figure 1a). Dermoscopy of lesions revealed reddish purple structureless areas, without specific features of any skin neoplasm (Figure 1b). A biopsy of a breast nodule was performed. The histological examination revealed a non encapsulated vascular tumor involving the mid and lower dermis. It was composed of multiple dilated, cavernous-like capillaries containing erythrocytes surrounded by endothelial cells, and one to several layers of uniform cuboidal cells with pale or faintly eosinophilic cytoplasm (glomus cells) (Figure 1c). These features were consistent with the diagnosis of glomangioma. Complete blood and platelet counts, coagulation tests and fecal occult blood test were within normal range. Informed about the nature of the lesions and treatment options the patient chose therapeutic abstention.
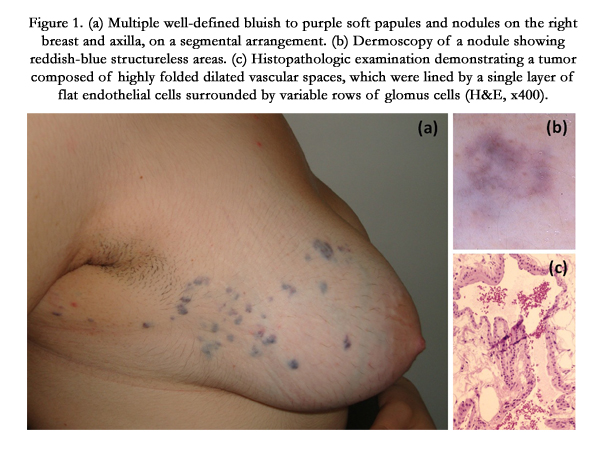
Figure 1. (a) Multiple well-defined bluish to purple soft papules and nodules on the right breast and axilla, on a segmental arrangement. (b) Dermoscopy of a nodule showing reddish-blue structureless areas. (c) Histopathologic examination demonstrating a tumor composed of highly folded dilated vascular spaces, which were lined by a single layer of flat endothelial cells surrounded by variable rows of glomus cells (H&E, x400).
Discussion
Glomus tumors (GTs) are relatively uncommon, benign vascular neoplasms derived from glomus body, a specialized form of arteriovenous temperature-regulating anatomosis [1, 2]. Histologically, they can be classified into solid glomus tumor, glomangioma and glomangiomyoma according to the relative proportions of cellular components [2].
GTs can be solitary or multiple. The solitary form is most commonly found on the extremities, and often is associated with paroxysmal pain, which can be spontaneous or triggered by changes in temperature and pressure. In contrast, multiple GTs, or glomangiomas, have an earlier age of onset than the solitary ones, often appearing during childhood, may also involve systemic organs and are usually asymptomatic [3]. This variant represents a small portion of GTs and is currently called “glomuvenous malformation” (GVM), for it corresponds to the presence of vascular malformation caused by glomulin (GLMN) gene mutation [4]. The involved gene is located in chromosome 1p21-22 [3]. GVMs may be inherited in an autosomal dominant fashion, with incomplete penetrance and variable expressivity. They can be further subdivided into localized/regional, segmental, or disseminated/ widespread types [1, 2]. A congenital plaque-like variant, characterized by either grouped papules coalescing to form indurated plaques or clusters of discrete nodules, is observed in a minority of cases [6].
Segmental forms may manifest cutaneous mosaicism. Two types of segmental arrangements can be described: a) Type 1, characterized by the presence of less severe lesions and reflecting the heterozygosity of the mutation; b) Type 2, originated by the loss of heterozygosity during the first stages of embryogenesis leading to diffuse and severe development of GTs later in life at sites distant from the original lesion [3, 7, 8].
In our patient, the presence since birth of numerous agminated papules and nodules with histological features of glomangiomas and unilateral distribution suggests a cutaneous mosaicism. In this girl, there was no evidence of diffuse involvement, suggesting a Type 1 manifestation of glomangiomatosis. However, it is important to follow up the patient over time, since the appearance of new lesions elsewhere on the skin, during puberty or later in life, may point to a Type 2 involvement [8].
Treatment of GTs is only recommended for symptomatic lesions and includes surgical excision, sclerotherapy, and laser therapy [1,8].
Conclusion
The result of this study was encouraging. It is not only helpful to control the spread of the disease within short time but also indicating a definite role of homeopathic medicine in HPV infection and the risk of pre cancerous stage can be prevented.
References
- Brauer JA, Anolik R, Tzu J, Meehan S, Lieber CD, et al. (2011) Glomuvenous Malformations (Familial generalized multiple glomangiomas). Dermatol Online J 17(10): 9.
- Boon LM, Mulliken JB, Enjolras O, Vikkula M (2004) Glomuvenous malformation (glomangioma) and venous malformation: distinct clinicopathologic and genetic entities. Arch Dermatol 140(8): 971-976.
- Cabral CR, Oliveira Filho J, Matsumoto JL, Cignachi S, Tebet AC, et al. (2015) Type 2 segmental glomangioma: case report. An Bras Dermatol 90(3 Suppl 1): S97-100.
- Solovan C, Chiticariu E, Beinsan D, Zurac S, Baderca F (2012) Multiple disseminated glomuvenous malformations: do we know enough? Rom J Morphol Embryol 53(4): 1077-1080.
- Brouillard P, Ghassibé M, Penington A, Boon LM, Dompmartin A, et al. (2005) Four common glomulin mutations cause two thirds of glomuvenous malformations ("familial glomangiomas"): evidence for a founder effect. J Med Genet 42(2): e13.
- Mallory SB, Enjolras O, Boon LM, Rogers E, Berk DR, et al. (2006) Congenital plaque-type glomuvenous malformations presenting in childhood. Arch Dermatol 142(7): 892-896.
- Happle R, König A (1999) Type 2 segmental manifestation of multiple glomus tumours: A review and reclassification of 5 case reports. Dermatology 198(3): 270-272.
- Munoz C, Bobadilla F, Fuenzalida H, Goldner R, Sina B (2011) Congenital glomangioma of the breast: type 2 segmental manifestation. Int J Dermatol 50(3): 346-349.





