Stevens - Johnson Syndrome Induced by Sorafenib for Hepatocellular Carcinoma
Chakiri R*, Douhi Z, Meziane M, Mernissi FZ
Dermatology, university hospital Hassan II, Fez, Morocco.
*Corresponding Author
Chakiri Radia,
Dermatology, university hospital Hassan II,
Fez, Morocco.
Email: r.chakiri.87@gmail.com
Received: March12, 2016; Accepted : May 09, 2016; Published: May 09, 2016
Citation: Chakiri R, Douhi Z, Meziane M, Mernissi FZ (2016) Stevens - Johnson Syndrome Induced by Sorafenib for Hepatocellular Carcinoma. Int J Clin Dermatol Res. 4(1), 78-80.DOI : dx.doi.org/10.19070/2332-2977-160001
Copyright: Chakiri R© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Sorafenib is a new therapeutic agent being used in hepatocellular carcinoma, renal cell carcinoma and malignant melanoma. The most frequently seen cutaneous side effects due to sorafenib are erythema, exfoliative dermatitis, acne vulgaris and hand-foot skin reaction. Erythema multiforme, stevens-johnson syndrome are rare side effects of sorafenib.
Observation: We present a 34-years-old woman with stevens-Johnson syndrome induced by sorafenib for hepatocellular carcinoma.
Conclusion: Patients treated with sorafenib for HCC should be monitored closely with a multidisciplinary approach, and if SJS is diagnosed, these patients cannot be given sorafenib again.
2.Case Report
3.Discussion
4.Conclusion
5.References
Introduction
Sorafenib is an orally active multikinase inhibitor blocking both tumor cell proliferation and angiogenesis. It is currently approved for the treatment of advanced renal cell cancer and hepatocellular carcinoma.
Skin toxicity, such as hand-foot skin reaction (HFSR), is one of the frequent adverse effects of sorafenib; it is dose dependent and disappears with discontinuation of sorafenib. On the other hand, erythema multiforme (EM) and Stevens-Johnson syndrome (SJS) are the very rare side effects of sorafenib. We report a case of SJS caused by sorafenib for hepatocellular carcinoma.
Case Report
34-year old woman was follow-up in gastroenterology department for hepatocellular carcinoma complicating hepatitis B traited by sebivo, she have been put under Sorafenib (400mg/day), 10 days after the start of Sorafenib the patient presented erythematous itchy rash at the two lower limbs and upper limb with extension to trunk and face.
Dermatological examination had found: erythematous target lesion in the upper limbs and back (Figure 1), urticarial plaques on the trunk, purpuric lesions on the lower extremities and blisters stretched at the back side of 2 feet and achieving of the buccal and genital mucosa (Figure 2).
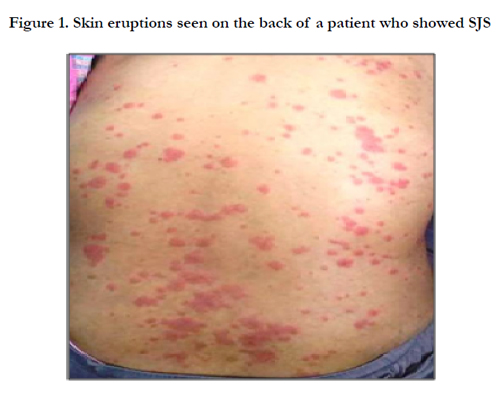

Figure 1. Skin eruptions seen on the back of a patient who showed SJS
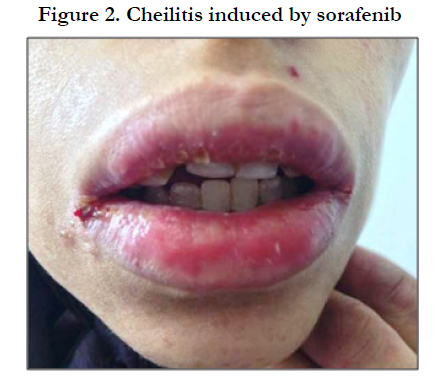

Figure 2. Cheilitis induced by sorafenib
Admission laboratory tests revealed several abnormal finding: hypereosinophilia in 2100 element/mm3 and hepatic cytolysis (SGOT=92 UI/L→2xN, SGPT=188 UI/L→4xN).
Skin biopsy revealed parakeratosis, focal spongiosis, and perivascular inflammation. According to the clinical, biological and histopathologic findings, the patient was diagnosed as having SJS. She discontinued sorafenib therapy and she was treated symptomatically with good clinical and biological outcome.
Discussion
We report the second case of SJS induced by sorafenib for hepatocellular carcinoma; the first one was reported by Ikeda et al in patient with metastatic renal cell carcinoma [1].
Sorafenib belongs to the family of targeted therapies that are new anti-cancer drugs entering clinical practice that target specific mechanisms responsible for cell growth, spread and survival. One new drug, sorafenib, has been introduced in the treatment of hepatocellular carcinoma, to radically change the prognosis of these patients [2].
Sorafenib is a potent inhibitor of Raf-1, a key enzyme in the Ras/ Raf/MEK/ERK signaling pathway leading to cell proliferation. It interferes with both the angiogenesis and the endothelial growth factor receptor (EGFR) pathway. Early trials have demonstrated the antitumor potential of sorafenib in patients with hepatocellular carcinoma, melanoma, non–small cell lung cancer (NSCLC), cancers of the pancreas and colon, and other solid tumors [2, 3].
Extra-dermatological side effects related to sorafenib are fatigue, hypertension, Arterial thromboembolic events, Hemorrhage complications, including epistaxis, hemoptysis, hematemesis, gastrointestinal, vaginal and cerebral hemorrhage, have been described as severe and mortality-related adverse effects in patients treated with sorafenib [4].
Skin toxicity is the most common adverse events induced by sorafenib. W.J.Lee et al reported that hand-and-foot skin reaction (HFSR ) was the most common cutaneous toxicity (48%) characterized by well-demarcated, tender, erythematous papules and plaques with grayish blisters or hyperkeratotic, callus-like formations on palmoplantar surfaces and distal phalanges. Others cutaneous toxicities included alopecia (26%), stomatitis (26%) and erythematous eruption on the trunk (20%) [5].
Stevens-Johnson syndrome was first described in 1922 as an extraordinary, generalized epidermal eruption. It is accompanied by fever, inflammation of the buccal mucosa, and severe purulent conjunctivitis. Incidence of this disorder is unknown, but it is thought to be very low. The etiology of this disorder is multiple, including drugs such as (Nevirapine, Carbamazepine, Phenytoin, Phenobarbital, Allopurinol and Quinolones …), infectious agents, and idiopathic causes [6, 7].
Clinically, SJS is characterized by confluent purpuric macules or atypical flat targetoid lesions, with blisters and erosions covering <10% of body surface area [7].
The mortality rate mainly depends on the age and health of the patient, and rates can range from 30 to 100 percent. Individuals at opposite ends of the age spectrum, the very young and the old, are usually fatal cases. Death is commonly due to infectious complications [6].
Ikeda et al. reported the first Sorafenib-induced SJS. They described a 67-year-old man with lymph node and bone metastases from clear-cell received sorafenib(800mg/day). As in our case, ten days after sorafenib initiation, the patient presented clinical sign of SJS. The patient discontinued sorafenib treatement and was treated with prednisolone (15mg/day) and betamethasone butyrate propionate cream for 2 weeks with good clinical outcome. But in our case: discontinuation of sorafenib associated with symptomatic treatement allowed good clinical and biological outcome.
The pathophysiology steven johnson syndrome is like any severe drug reactions is unknown, but the most plausible theory is the assumption that a reactive metabolite is responsible [8].
According to this theory, severe drug reactions result from exposure to an increased amount of reactive metabolites (oxidative), a reduced production of nontoxic metabolites normal soluble and / or a reduced ability to detoxify reactive metabolites. But the sorafenib molecular mechanism of this type of toxicity remains unknown and further studies will be required to elucidate it as well as identify an effective treatment strategy [8].
Whatever the pathophysiological mechanism, sorafenib cannot be readministered to a patient who has had this toxic skin reaction.
Conclusion
The new targeted therapies have been commonly used in patients with metastatic carcinoma.
Patients treated with sorafenib for HCC should be monitored closely with a multidisciplinary approach, and if SJS is diagnosed, these patients cannot be given sorafenib again.
We recommended dermatologic examination of patients who have cutaneous eruptions while receiving multikinase inhibitors, and, if necessary, skin biopsy must be performed for distinguishing the cutaneous side effects of these agents. We must be very careful and follow up these patients with a multidisciplinary approach.
References
- Ikeda M, et al. (2013) Stevens-Johnson Syndrome Induced by Sorafenib for Metastatic Renal Cell Carcinoma. Urologia internationalis 91(4): 482–483.
- Cemal Bilac, et al. (2009) Sorafenib-induced erythema multiforme in metastatic renal cell carcinoma. Cutaneous and Ocular Toxicology 28(2): 90–92.
- Heidary N, Naik H, Burgin S (2008) Chemotherapeutic agents and the skin: an update. J Am Acad Dermatol 58(4): 545-570.
- Ye Li, Zu-Hua Gao, Xian-Jun Qu (2015) The Adverse Effects of Sorafenib in Patients with Advanced Cancers. Basic & Clinical Pharmacology & Toxicology 116(3): 216–221.
- Lee WJ, Lee JL, Chang SE (2009) Cutaneous adverse effects in patients treated with the multitargeted kinase inhibitors sorafenib and sunitinib. Br J Dermatol 161(5): 1045–1051.
- Stitt VJ Jr (1988) Stevens-Johnson Syndrome: A Review of the Literature. J Natl Med Assoc 80(1): 106-108.
- Schwartz, McDonough, Lee (2013) Toxic epidermal necrolysis: Part I. Introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol 69(2): 173-e1.
- Bachot N, Roujeau JC (2001) Physiopathology and treatment of severe drug eruptions. Curr Opin Allergy Clin Immunol 1(4): 293-298.





