Phlyctenular Conjunctivitis and Tuberculosis
Tomar M1*, Sharma G2, Sood T3
1 Senior resident, Department of Ophthalmology, Dr, RPGMC Tanda, District kangra, Himachal Pradesh, India.
2 Assistant Professor, Department of Ophthalmology, Dr, RPGMC Tanda, District Kangra, Himachal Pradesh, India.
3 Ophalmologist, Civil Hospital Sarkaghat, District Mandi, Himachal Pradesh, India.
*Corresponding Author
Mandeep Tomar,
Senior Resident, Department of Ophthalmology, Dr. RPGMC Tanda,
District Kangra, Himachal Pradesh, Pin -176001, India.
Tel: 09459266181
Fax: 01892267115
E-mail: sunnyigmc85@gmail.com
Received: April 27, 2016; Accepted: July 05, 2016 ; Published: July 07, 2016
Citation: Tomar M, Sharma G, Sood T (2016) Phlyctenular Conjunctivitis and Tuberculosis. Int J Ophthalmol Eye Res. 4(6), 233-236.DOI : dx.doi.org/10.19070/2332-290X-1500048
Copyright: Tomar M© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Phlyctenular keratoconjunctivitis is a nodular affliction characterized by the formation of a small, circumscribed lesion at the corneal limbus and now accepted as a morphologic expression of delayed hypersensitivity to diverse antigens. The condition is one of several corneal disorders that arise as an expression of altered immune mechanisms [4].
Materials and Methods: A 2.5 years old male child presented with a history of watering and redness from his left eye since 3-4 days.On ocular examination, an elevated nodule of approximately 2x1 mm in size with central erosion at 1‘0 clock and of size 1x1 mm was present at 6:0 clock position at the limbus. History of ATT intake in the mother for a period of 6 months ,at 1 year of age, was present. Monteux was 25x26 mm(Figure 3), ESR was 34mm in 1st hour,chest radiograph revealed perihilar shadows.
Results: Child was put on Antitubercular therapy in the form of rifampicin (10mg/kg/day), isoniazid (10mg/kg/day), pyrazinamide (25mg/kg/day) for 2 months (2HRZ) and isoniazid and rifampicin for another 4 months (4HR). Phlyctens resolved after a follow up of 1 month.
Conclusion: Phlyctenular keratoconjunctivitis should be evaluated for tuberculosis and with a positive test, should be referred for tuberculosis therapy.
2.Introduction
3.Case Report
4.Discussion
4.1.Differential Diagnoses for Corneal nodule and irritation
5.Conclusion
6.References
Keywords
Phlyctenular; Conjunctivitis; Tuberculosis.
Introduction
Phlyctenular keratoconjunctivitis is a nodular affliction characterized by the formation of a small, circumscribed lesion at the corneal limbus. At one stage the lesion may resemble a blister, but the small red nodule of lymphoid tissue characteristically develops into a microabscess that ulcerates and heals in 10 to 14 days. Ostler and Lanier [1] and Thygeson [2] reported the relationship between phlyctenular keratoconjunctivitis and tuberculoprotein. Thygeson believed that the incidence of phlyctenulosis on a worldwide basis appeared to parallel the incidence of tuberculosis [3]. Phlyctenular keratoconjunctivitis is now accepted as a morphologic expression of delayed hypersensitivity to diverse antigens. The condition is one of several corneal disorders that arise as an expression of altered immune mechanisms [4].
Case Report
A 2.5 years old male child presented to the eye OPD at Dr. RPGMC Tanda with a history of watering and redness from his left eye since 3-4 days. There was no H/O any diminision of vision, pain and purulent discharge from the eye. There was no history of tuberculosis, diabetes, hypertension and other systemic complaints in the child. But, history of ATT intake in the mother for pulmonary tuberculosis for a period of 6 months was present,when the child was of 1 year of age. On ocular examination, lids and adnexa were normal. An elevated yellowish white nodule of approximately 2x1 mm in size with central erosion and fluorescein uptake with surrounding engorged hyperemic vessels was present at 1‘0 clock position at limbus (Figure 1). Another nodule of size approximately 1x1 mm was present at 6:0 clock position at the limbus (Figure 2). Conjunctival injection was present surrounding the nodules. On investigatons, Monteux was 25x26 mm (Figure 3), ESR was 34mm in 1st hour, chest radiograph revealed perihilar shadows. Following all these findings, child was put on Antitubercular therapy in the form of rifampicin (10mg/ kg/day), isoniazid (10mg/kg/day), pyrazinamide (25mg/kg/day) for 2 months (2HRZ) and isoniazid and rifampicin for another 4 months (4HR). Phlyctens resolved after a follow up of 1 month and conjunctival inflammation subsided leaving residual scarring at the limbus(Figure 4 and 5) .


Figure 1. Phlycten with surrounding conjunctival injection at 1’ 0 clock position.


Figure 2. Phlycten with surrounding conjunctival injection at 6’ 0 clock position.


Figure 3. Induration with scarring following monteux test.
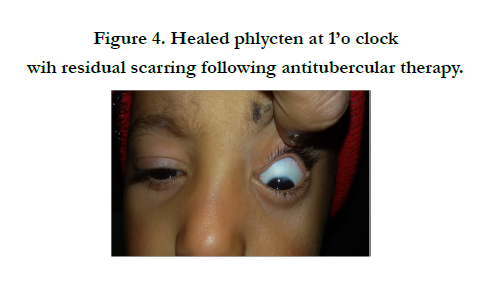

Figure 4. Healed phlycten at 1’o clock wih residual scarring following antitubercular therapy.


Figure 5. Healed phlycten at 6’o clock following antitubercular therapy.
Discussion
Phlyctenular keratoconjunctivitis has been associated in the past with poor, undernourished, sickly children, with tuberculosis strongly implicated. Duke-Elder described the pitiable position of these children: “During the day the child hides away in a dark corner, burying his face in his hands; and during the night he curls up under the blankets” [5]. Phlyctenular keratoconjunctivitis has a worldwide distribution. It is found most commonly during the first and second decades of life in children living in crowded, impoverished quarters. All observers report a higher incidence (60% to 70% of reported cases) in girls than in boys [6, 7]. Sorsby reported that phlyctenular keratoconjunctivitis occurs more often in spring and summer than in late autumn or winter [7].
Although the precise mechanism by which phlyctenules are produced has not been determined, it is assumed from clinical evidence that the patient has been sensitized to the offending antigen in the past. In patients with tuberculosis, this sensitization presumably occurred as part of a bacteremia from an early infection in the lungs or lymph glands. For nontuberculous phlyctenular keratoconjunctivitis caused, for example, by Staphylococcus, the antigen probably comes from the pathogenic staphylococci that inhabit the lid margins of all people from time to time. The attack of phlyctenular keratoconjunctivitis may be precipitated by the presentation of the antigen to the sensitized ocular tissue, either by the bloodstream in the event of a recrudescence of a focus of infection elsewhere or by an exogenous inoculation of bacteria into the conjunctival sac from the lid margin. A phlyctenule may occur on the conjunctiva or on the cornea (Figure 6). The different locations give different symptoms and signs, and they have a different prognosis for vision.
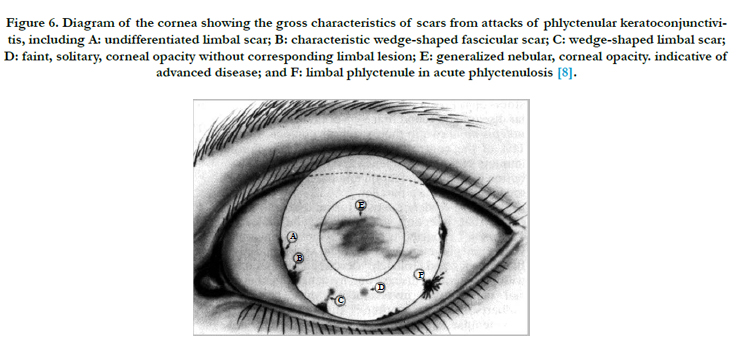
Figure 6. Diagram of the cornea showing the gross characteristics of scars from attacks of phlyctenular keratoconjunctivitis, including A: undifferentiated limbal scar; B: characteristic wedge-shaped fascicular scar; C: wedge-shaped limbal scar; D: faint, solitary, corneal opacity without corresponding limbal lesion; E: generalized nebular, corneal opacity. indicative of advanced disease; and F: limbal phlyctenule in acute phlyctenulosis [8].
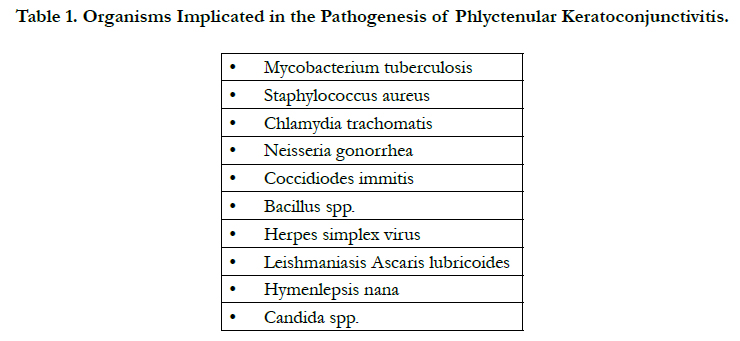

Table 1. Organisms Implicated in the Pathogenesis of Phlyctenular Keratoconjunctivitis.
- Staphylococcal marginal keratitis with phlyctenule
- Microbial keratitis
- Inflamed pseudopterygium
- Salzmann's nodule
- Corneal foreign body
Conclusion
The patient with phlyctenular keratoconjunctivitis should be evaluated for tuberculosis. An intermediate-strength tuberculin test should establish the state of the tubercular reaction. Children and young adults younger than 20 years of age with a positive test, as well as any adult with a recently converted test result, should be referred for tuberculosis therapy. If the patient with a positive tuberculin test and phlyctenulosis is a child, a thorough investigation of the family for tuberculosis should be made.
References
- Ostler HB, Lanier JD (1974) Phlyctenular keratoconjunctivitis with special reference to the staphylococcal type. Transactions of the Pacific Coast Otoophthalmology Society Annual Meeting 55: 237.
- Thygeson P (1974) Non-tuberculous phlyctenular keratoconjunctivitis. In Golden B (edn): Ocular Inflammatory Disease. Springfield, IL, Charles C Thomas. 50.
- Thygeson P (1951) Etiology and treatment of phlyctenular keratoconjunctivitis. Am J Ophthalmol 34(9): 1217-1236.
- Beauchamp GR, Gillette TE, Friendly DS (1981) Phlyctenular keratoconjunctivitis. J Pediatr Ophthalmol Strabismus 18(3): 22-28.
- Duke-Elder S (1965) System of Ophthalmology. St. Louis, CV Mosby 8.
- Philip RN, Comstock GW, Shelton JH (1965) Phlyctenular keratoconjunctivitis among Eskimos in southern Alaska: I. Epidemiologic characteristics. Am Rev Respir Dis 91: 171.
- Sorsby A (1942) The aetiology of phlyctenular ophthalmia. Br J Ophthalmol 26(4): 159-179.
- Philip RN, Comstock GW, Shelton JH (1965) Phlyctenular keratoconjuntivitis among Eskimos in southern Alaska: I. Epidemiologic characteristics. Am Rev Respir Dis 91: 171.





