Observation of Peripheral Retina Using Video Laryngoscopy For Screening of Retinopathy of Prematurity
Yamada S1, Takayama K1, Sakamoto H2, Takegawa M2, Yoshii M2, Taguchi H1, Akimoto M1*
1 Departments of Ophthalmology, Osaka Red Cross Hospital,Japan.
2 Departments of Pediatrics, Osaka Red Cross Hospital, Japan.
*Corresponding Author
Masayuki Akimoto MD, PhD
Ophthalmology, Osaka Red Cross Hospital,
5-30 Fudegasakicho, Tennojiku,Osaka 543-8555, Japan.
Tel: +81-6-6774-5111
Fax: +81-6-6774-5131
E-mail: masayuki@akimoto3.com
Received: July 13, 2016; Accepted: September 06, 2016; Published: September 14, 2016
Citation: Akimoto M, et .al., (2016) Observation of Peripheral Retina Using Video Laryngoscopy For Screening of Retinopathy of Prematurity. Int J Ophthalmol Eye Res. 4(8), 246-248.DOI : dx.doi.org/10.19070/2332-290X-1500051
Copyright: Akimoto M© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background and Objective: Retinal observation in immature infants is highly important to screen and evaluate the progression of retinopathy of prematurity (ROP). Sharing the information with pediatricians and ophthalmologists is also important. Although video laryngoscopy is a tool for observation of the larynx to secure the airway, a recent study showed that it can visualize posterior fundi and allow diagnosis of shaken-baby syndrome even by pediatricians.
Material and Methods: We evaluated the potential to observe the retinal periphery using video laryngoscopy in comparison with other imaging systems.
Results: Video laryngoscopy can visualize avascular zones, ridges, and spots of photocoagulation.
Conclusion: It is a good alternative for recording findings for the diagnosis of ROP.
2.Introduction
3.Technique and Discussion
4.References
Keywords
Retinopathy of Prematurity; Fundus Photograph; Video Laryngoscopy.
Introduction
Sharing the information on fundus status of prematurity with pediatricians and ophthalmologists is highly important because retinopathy of prematurity can be fatal for visual acuity if the disease progresses [1-4]. To share the fundus status, photographs can be taken by using commercially available special fundus cameras such as RetCam III (Clarity, Pleasanton, CA). However, RetCam III is too expensive for many hospitals to install.
Video laryngoscopy is a relatively new and inexpensive technique that supports intratracheal intubation by direct viewing and recording of the larynx for intratracheal intubation with its charged-coupled device (CCD) camcorder. It is a common technique used in hospitals, especially in emergency units. Video laryngoscopes consist of a CCD camcorder, a light-emitting diode (LED), and a recording unit. The system has two different probes, a large one for adults and a smaller one for children.
A previous report indicated that pediatricians can record retinal hemorrhages in the posterior pole of the eyes of 2-month-old boys by using video laryngoscopy [5]. The quality of the obtained pictures of retinal hemorrhages in the posterior pole was good enough to be used as evidence of shaken-baby syndrome.
We hypothesized that video laryngoscopy can be used to observe the peripheral retina in prematurity. The fundus photographs recorded willbe useful to share with pediatricians and ophthalmologists.
Technique and Discussion
After the safety of the LED power against retinal phototoxicity was confirmed, we recorded the prematurity fundus image by using GlideScope (Verathon Inc. Bothell, WA), a video laryngoscope,and compared the image with that obtained using RetCam III, a commercial pediatric ophthalmoscope, and VersaCam (Nidek, Aichi, Japan), a handy fundus camera (Figure 1).
Six premature babies were included in the present study. All the investigations adhered to the tenets of the Declaration of Helsinki, and the study was approved by the institutional review board and ethics committee of our hospital. After the possible consequences of the study were explained to the parents of the participating subjects, written informed consent was obtained from them.
The subjects were aged 1 to 8 months (mean ± SD, 4.5 ± 3.5 months). All the subjects underwent fundus examination with three instruments, namely GlideScope, RetCam III, and VersaCam. With GlideScope, a small probe was used for the pediatric patients, a corneal protective drop solution was applied in the eye, and the probe was attached on the cornea. VersaCam was used in combination with a 20-D objective lens.
The quality of the obtained image is shown in (Figure 1). We obtained fundus images for all patients by using RetCam III, with good quality. Fundus images were obtained for all the patients by using GlideScope. By changing the probe angle to the cornea, peripheral images were obtained by using GlideScope without scleral indentation (Figure 2). The quality of the images obtained using GlideScope was good enough to record and share the fundus status but not good as the quality of the images obtained using RetCam III, probably because of the lens panfocus and low CCD density of GlideScope. We also obtained post-pole fundus images by using VersaCam but had difficulty obtaining peripheral images.
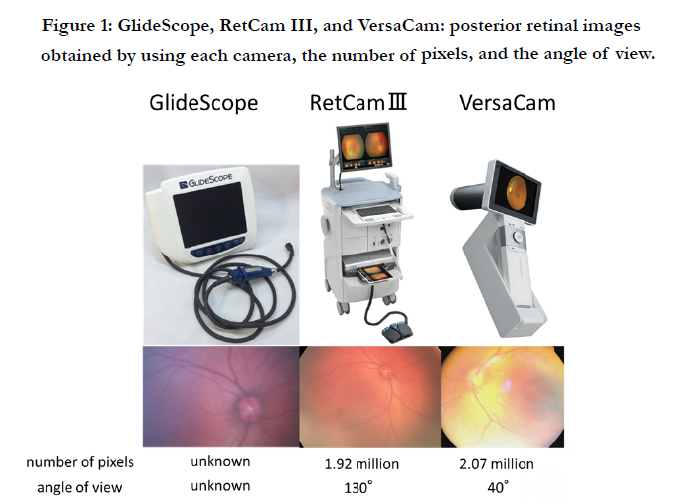

Figure 1: GlideScope, RetCam III, and VersaCam: posterior retinal images obtained by using each camera, the number of pixels, and the angle of view.
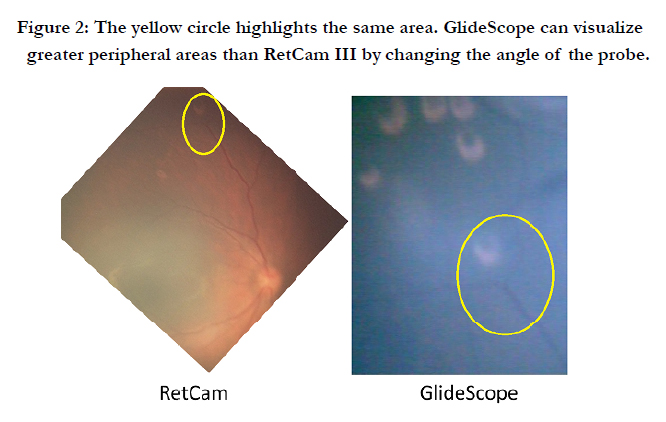
Figure 2: The yellow circle highlights the same area. GlideScope can visualize greater peripheral areas than RetCam III by changing the angle of the probe.
Although the best-quality fundus images were obtained using RetCam III, video laryngoscopy can be used to record fundus images of infants, not only in the posterior pole but also in the periphery.
In conclusion, video laryngoscopy is a good alternative to record pediatric or prematurity fundus when special fundus recording instruments such as RetCam III are unavailable.
References
- Beligene N, Perumalswamv V, Tandon M, et al., (2015) Retinopathy of prematurity and neurodevelopmental disabilities in premature infants. Semin Fetal Neonatal Med. 20(5): 346-53.
- Vinekar A, Jayadev C, Mangalesh S, Shetty B, Vidyasagar D (2015) Role of tele-medicine in retinopathy of prematurity screening in rural outreach centers in India: a report of 20,214 imaging sessions in the KIDROP program. Semin Fetal Neonatal Med. 20(5): 335-45.
- Prakalapakorn SG, Wallace DK, Freedman SF (2014) Retinal imaging in premature infants using the Pictor noncontact digital camera. J AAPOS. 18(4): 321-6.
- Prakalapakorn SG, Freedman SF, Wallace DK (2014) Evaluation of an indirect ophthalmoscopy digital photographic system as a retinopathy of prematurity screening tool. J AAPOS. 18(1): 36-41.
- Kitamura M, Kasai M, Kurosaka N, Matsui H (2014) Pediatric ophthalmoscopy by video laryngoscope. Intensive Care Med. 40(8): 1159.





