Steroid Sparing Symptomatic Control of Thygeson’s Superficial Punctate Keratitis (TSPK)
U Agraval*, M Edington, K Ramaesh
Department of Ophthalmology, Gartnavel General Hospital, Great Western Rd, Glasgow G12 0YN, UK.
*Corresponding Author
Umiya Agraval,
Department of Ophthalmology, Gartnavel General Hospital 1053 Great Western Rd,
Glasgow G12 0YN, UK.
E-mail: umiya.agraval@nhs.net
Received: September 01, 2016; Accepted: October 03, 2016; Published: October 07, 2016
Citation: U Agraval, M Edington, K Ramaesh (2016) Steroid Sparing Symptomatic Control of Thygeson’s Superficial Punctate Keratitis (TSPK). Int J Ophthalmol Eye Res. 4(9), 249-252.
doi:dx.doi.org/10.19070/2332-290X-1600052
Copyright: U Agraval© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Thygeson’s superficial punctate keratitis (TSPK) is a chronic, recurrent disorder affecting the anterior surface of the cornea. Common symptoms include photophobia, epiphora, pain and blurred vision. The management of TSPK is challenging, and long-term combined therapy is often required, namely steroids. We present a case of TSPK that was managed with a novel regenerative agent (RGTA) resulting in the symptomatic control of the condition.
Methods: Observational case report.
Case: A 25-year-old male patient with bilateral TSPK presented with ongoing symptoms of irritation, photophobia and foreign body sensation. Previous treatment included steroids, bandage contact lens, antibiotics and various lubricants. While steroids controlled his symptoms, he was concerned about side effects of long-term use and unwilling to persevere with treatment. He was intolerant to cyclosporin drops. As an alternative, he was started on regenerative agent poly (carboxymethylglucose sulphate) known as Cacicol™. Over weeks of treatment, his symptoms were documented using a pain and photophobia score, and improved considerably. The appearance of his corneal surface also improved although epithelial defects did not completely resolve.
Discussion: Literature suggests that medical interventions do not modify the natural history of TSPK and therefore treatment should be aimed at achieving symptomatic relief. During treatment with RGTA, our patient’s symptomatic relief was striking. Although, RGTA may not modify the pathogenesis of TSPK, it appears to promote healing of epithelial defects and reduce associated pain, and there is evidence to suggest it may be a useful alternative therapy to control the symptoms of TSPK.
2.Introduction
3.Case
4.Discussion
5.References
Keywords
Thygeson’s Keratitis; Therapy; Regenerative Agent; Carboxymethylglucose Sulphate.
Introduction
Thygeson’s superficial punctate keratitis (TSPK) was first described by Phillips Thygeson in 1950 [1]. It is a chronic, usually bilateral disorder affecting the anterior surface of the cornea and characterised by small, elevated, white-grey, oval intra-epithelial opacities with a central distribution [2]. The common symptoms include photophobia, tearing, burning, foreign body sensation, pain and blurred vision [3]. Episodes are recurrent, and can last a few months. During acute episodes, multiple lesions are present on the intra-epithelial cornea but tend to resolve without scarring [5, 6]. The course of the disease is variable but in most cases it resolves completely within 4 years of onset [3]. Conversely, there have been cases reported of the disease lasting more than 20 years [4].
The pathophysiology of TSPK remains unknown; both viral and immunologic mechanisms have been postulated. The histopathology is characterised by intra and intercellular oedema on the cornea epithelium and exudates under the lesions [7]. Abnormalities in the sub-epithelial nerve plexus, Bowman’s membrane and anterior stroma have been found in more severe conditions [8]. Confocal microscopy of the intra-epithelial lesions show the keratocytes have highly reflective nuclei and the cell bodies are of irregular size and shape, with no evidence of inflammatory cells in the areas of corneal stroma adjacent to the lesions [7]. A recent study showed three consistent findings in all patients with TSPK; highly reflective ‘starburst’ deposits which may correspond with the punctate lesions at the superficial and basal epithelial cell layers, invasion of Langerhans cells at the basal epithelial layer, and a sub-epithelial haze [9].
Over the years, various strategies have been implemented in the management of TSPK, some more successful than others. Antibiotics and antivirals have not been found to be effective; however, mild improvements have been reported with trifluridine therapy, which is not widely available [10, 11]. Topical lubricants are helpful but only partially relieve the symptoms [12].
The most effective and mainstay treatment of TSPK is topical steroids [5, 10]. In most cases, the steroids are tapered slowly over months until a minimum dosage is achieved which controls the symptoms [13]. However, the use of long-term steroids has known side effects. Topical cyclosporin had been proposed as a safer alternative to steroids and shown to be effective [14, 15]. However, no clinical trial comparing the two treatments has been undertaken and compliance may be an issue as cyclosporin drops can be cause discomfort and irritation on instillation.
The use of a therapeutic soft contact lens is an alternative treatment and has been shown to be effective in severe cases, although there is a potential risk of microbial keratitis [16]. Excimer laser phototherapeutic keratectomy has been shown to partially improve symptoms, however resulted in a higher recurrence rate [17].
The management of TSPK is therefore challenging and literature indicates that combined therapy is often required, as well as regular monitoring for possible side effects of the treatment. We present a case of TSPK that was managed with a novel regenerative agent (RGTA) resulting in the symptomatic control of the condition.
Case
A 25-year-old male patient was seen at the cornea clinic for ongoing symptoms of irritation, photophobia and foreign body sensation affecting both eyes. He was diagnosed with bilateral TSPK at the age of eight. Previous treatment included steroids, bandage contact lens, antibiotic and various lubricants. He was healthy apart from a history of asthma managed with inhalers.
On presentation his visual acuity was 6/6 bilaterally and he had active TSPK with corneal lesions and epithelial defects in both eyes. He was treated initially with topical fluorometholone (FML) once a day, which reduced his symptoms. However, he was reluctant to persevere with steroids due to the known longterm side effects and treatment was discontinued. His symptoms recurred shortly thereafter, and topical cyclosporin 0.3% three times a day was initiated as an alternative. Unfortunately, he was not able to tolerate the cyclosporin due to stinging sensation and he had another flare up of symptoms three months after stopping the drops. He was therefore restarted on topical FML every other day.
He was reviewed two months later, and scored the severity of photophobia 7 out of 10 and pain 3 out of 10. The visual acuity was 6/6 and 6/9 in the right and left eye respectively. Examination revealed characteristic central corneal lesions, which stained with fluorescein. As the patient was reluctant to increase the dose of steroids or remain on them long-term, he was started on topical regenerative agent poly (carboxymethylglucose sulphate), also known as Cacicol, once a day on alternate days to both eyes (Figure 1).
Two weeks later, his symptoms were improving and his vision was 6/6 in both eyes. He reported a photophobia score of 2 out of 10 and pain score of 1 out of 10. Examination of the cornea showed fewer lesions; however, the lesions had not completely resolved and there were still epithelial defects present. The treatment was continued once a day on alternate days.
After four weeks on the treatment, his vision remained stable and eyes were less photophobic but the patient reported a persistent gritty sensation and lesions with epithelial defects were stillvisualised on examination. The treatment was increased to once a day to both eyes, and after six weeks corneal surface improved.
After ten weeks of treatment the patient still reported mild irritation and photophobia, and the frequency of drops was increased to twice daily. However, this did not seem to have any additional effect on symptoms or corneal appearance, so frequency was reduced back to once daily. At nineteen weeks, the corneal surface had again improved slightly but there were persistent scattered epithelial defects. After twenty-seven weeks on the treatment, despite some persistent epithelial defects, photophobia score was 0 out of 10 and pain score 1 out of 10.
Discussion
Regenerative agent (RGTA) poly (carboxymethylglucose sulphate) is a large biopolymer containing carboxymethyl dextran sulphate that binds matrix proteins that affect corneal healing [23]. It is engineered to replace or imitate heparin sulphate molecules, which in turn restores the extracellular microenvironment (ECM) and improves the production of signals and essential growth factors for tissue healing and re-epithelislisation [18, 23]. Histological studies have shown that the effects of this regenerative agent include amelioration of tissue oedema, fibrosis and inflammation [24, 25]. The efficacy and safety of this treatment in the cornea has been demonstrated in previous studies, where it has been used with encouraging results in neurotrophic ulcers, chronic neurotrophic keratitis, corneal dystrophies, persistent epithelial defects and more recently in wound healing following cross linking therapy for keratoconus [18-22].
In our case, the patient was unable to tolerate cyclosporin and unwilling to remain on topical steroids long-term. The published literature, previous safety records, and our observations prompted us to consider RGTA as an alternate agent to manage the patient’s symptoms.
Although corneal lesions did not resolve completely, the use of the regenerative agent improved the pain and photophobia scores (Table 1). Individual corneal lesions healed rapidly but seemed to appear in different locations (Figure 1). It appears therefore, that while RGTA may not modify the initial pathogenesis of TSPK, it may promote healing once the epithelial defect is established by mimicking heparan sulphate molecules. Heparan is a key ECM component, holding collagen fibrils together and providing binding sites for growth factors. Injury to tissues results in loss of heparan in the ECM and the bound growth factors. Polymers that mimic the binding action of heparan may offer a matrix for growth factors to bind and cue cell migration and proliferation. Tissue regenerating agents encourage healing by mimicking the action of destroyed heparan-sulphate molecules, thereby recreating a cellular environment in which cells can multiply and migrate.
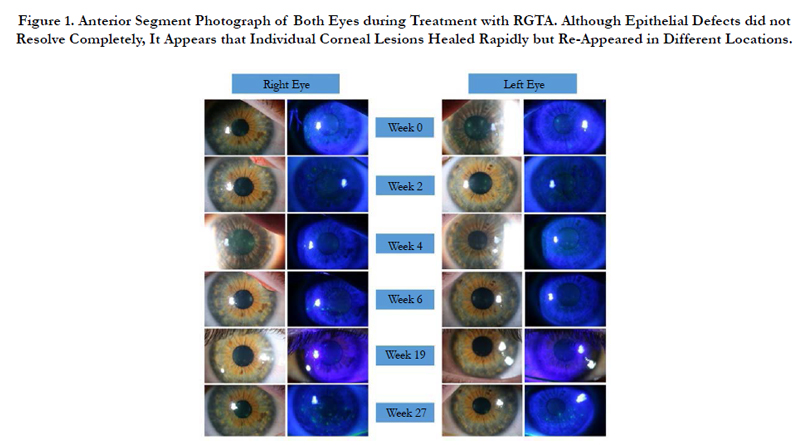

Figure 1. Anterior Segment Photograph of Both Eyes during Treatment with RGTA. Although Epithelial Defects did not Resolve Completely, It Appears that Individual Corneal Lesions Healed Rapidly but Re-Appeared in Different Locations.
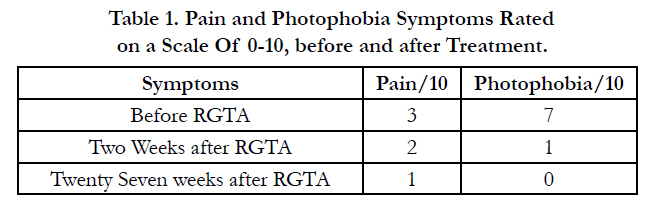

Table 1. Pain and Photophobia Symptoms Rated on a Scale Of 0-10, before and after Treatment.
During therapy with RGTA, the symptomatic relief is striking. Additional mechanisms may be suggested for the pain reliving actions of the drug. There is evidence to suggest RGTA possesses some anti-inflammatory properties, which may help to reduce pain and photophobia. RGTA may also form a protective layer around exposed nerves and thereby reduce the pain. These observations may provide basis for further explorations and scientific rationale to expand the clinical indications of RGTA.
TSPK is an unusual condition and the pathogenic mechanism remains a puzzle. Previous literature suggests that medical interventions do not modify the natural history of the disease and it simply must run its course. The treatment is therefore aimed at achieving symptomatic relief. The symptomatic relief achieved with RGTA was striking in our case. Application of RGTA is not known to cause any local or systemic adverse effects, making it a safe and effective topical agent for numerous corneal disorders.
References
- Thygeson P (1950) Superficial punctate keratitis. JAMA. 144 (18): 1544- 1549.
- Thygeson P (1961) Further observations on superficial punctate keratitis, Arch Ophthalmol. 66(2): 158-162.
- Darrell RW (1981) Thygeson’s superficial punctate keratitis: natural history and association with HLA-DR3. Trans Am Ophthalmol Soc. 79: 486-516.
- Tanzer DJ, Smith RE (1999) Superficial punctate keratitis of Thygeson: the longest course on record? Cornea. 18(6): 729-30.
- Thygeson P (1966) Clinical and laboratory observation on superficial punctate keratitis. Am J Ophthalmol. 61(5): 1344-9.
- Fintelmann RE, Vastine DW, Bloomer MM, Margolis TP (2012) Thygeson superficial punctate keratitis and scarring. Cornea. 31(12): 1446-8.
- Cheng LL, Young AL, Wong AK, Law RW, Lam DS (2004) In vivo confocal microscopy of Thygeson’s superficial punctate keratitis. Clin Exp Ophthalmol. 32(3): 325-7.
- Watson SL, Hollingsworth J, Tullo AB (2003) Confocal microscopy of Thygeson’s superficial punctate keratopathy. Cornea. 22(4): 294-9.
- Kobayashi A, Yokogawa H, Sugiyama K (2011) In Vivo Laser Confocal Microscopy Findings of Thygeson Superficial Punctate Keratitis. Cornea. 30(6): 675–680.
- Tabbara KF, Ostler HB, Dawson C, Oh J (1981) Thygeson's superficial punctate keratitis. Ophthalmology. 88(1): 75-7.
- Nesburn AB, Lowe GH 3rd, Lepoff NJ, Maguen E (1984) Effect of topical trifluridine on Thygeson’s superficial punctate keratitis. Ophthalmology. 91(10): 1188-92.
- Gock G, Ong K, McClellan K (1995) A classical case of Thygeson’s superficial punctate keratitis. Aust NZ J Ophthalmol. 23(1): 76-7.
- Duszak RS (2007) Diagnosis and management of Thygeson’s superficial punctate keratitis. Optometry. 78(7): 333-338.
- Reinhard T, Sundmacher R (1999) Topical cyclosporin A in Thygeson's superficial punctate keratitis. Graefes Arch Clin Exp Ophthalmol. 237(2):109- 112.
- Del Castillo JM, Del Castillo JB, Garcia-Sanchez J (1996) Effect of topical cyclosporin-A on Thygeson’s superficial punctate keratitis. Doc Ophthalmol. 93(3): 193–8.
- Forstot SL, Bender PS (1979) Treatment of Thygeson´s superficial punctate keratopathy with soft contact lenses. Am J Ophthalmol. 88(2):186-189.
- Goldstein MH, Feistmann JA, Bhatti MT (2002) PRK-pTK as a treatment for a patient with Thygeson´ superficial punctate keratopathy. CLAO J. 28(4): 172-3.
- Chebbi CK1, Kichenin K, Amar N, Nourry H, Warnet JM, et al., (2008) Pilot study of new matrix therapy agent (RGTA OTRA4120) in treatment resistant corneal ulcers and corneal dystrophy. J Fr Ophtalmol. 31(5): 465-471.
- Aifa A, Gueudry J, Portmann A, Delcampe A, Muraine M (2012) Topical treatment with a new matrix theraphy agent (RGTA) for the treatment of corneal neurotrophic ulcers. Invest Ophthalmol Vis Sci. 53(13): 8181-8185.
- De Monchy I1, Labbé A, Pogorzalek N, Gendron G, M'Garrech M, et al., (2012) Management of herpes zoster neurotrophic ulcers using a new matrix therapy agent (RGTA): a case report. J Fr Ophtalmol. 35(3): 187.
- Kymionis GD, Liakopoulos DA, Grentzelos MA, Diakonis VF, Klados NE, et al., (2014) Combined topical application of a regenerative agent with a bandage contact lens for the treatment of persistent epithelial defects. Cornea.33(8): 868-872.
- Kymionis GD1, Liakopoulos DA, Grentzelos MA, Tsoulnaras KI, Detorakis ET, et al., (2015) Effect of the Regenerative Agent Poly(Carboxymethylglucose Sulfate) on Corneal Would healing after corneal cross-linking for keratocomus.Cornea. 34(8): 928-931.
- Barritault D, Caruelle JP (2006) Regernating agents (RGTAs): a new therapeutic approach. Ann Pharm Fr. 64(2): 135-144.
- Brignole-Baudouin F1, Warnet JM, Barritault D, Baudouin C (2013) RGTA- based matrix therapy in severe experimental corneal lesions: safety and efficacy studies. J Fr Ophtalmol. 36(9): 740-747.
- Cejkova J, Olmiere C, Cejka C, Trosan P, Holan V (2014) The healing of alkali-injured cornea is stimulated by a novel matrix regenerating agent (RGTA, CACICOL20): a biopolymer mimicking heparin sulfates reducing proteolytic, oxidative and nitrosative damage. Histol Histopathol. 29(4): 457-478.





